Explain regarding cranial nerve 2
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have rich, comprehensive content from multiple authoritative sources. Let me compile the full answer.
Cranial Nerve II - The Optic Nerve
Overview
The optic nerve (CN II) is not a true cranial nerve in the strict sense - it is an extension of the brain itself, carrying afferent visual information from the retina to the visual centers of the brain. Because of this, it is surrounded by all three cranial meninges (dura, arachnoid, and pia mater), and its subarachnoid space is continuous with the cerebral subarachnoid space. - Gray's Anatomy for Students
Anatomy
Structure
- Carries approximately 1.2 million afferent nerve fibers, each originating from a retinal ganglion cell
- The fibers are divided into ~600 bundles by fibrous septae derived from the pia mater
- Most fibers synapse at the lateral geniculate body (LGB); a smaller proportion reach the pretectal nuclei in the midbrain (for pupillary light reflex)
- Nearly one-third of all fibers subserve the central 5° of the visual field
Four Anatomical Segments
| Segment | Length | Notes |
|---|---|---|
| Intraocular (optic disc) | ~1 mm deep, 1.5 mm diameter | The visible portion is the optic disc (papilla) |
| Intraorbital | 25-30 mm | Surrounded by the annulus of Zinn at the orbital apex |
| Intracanalicular | ~6 mm | Fixed to the canal wall - vulnerable in head trauma |
| Intracranial | 5-16 mm (avg 10 mm) | Long segments vulnerable to pituitary adenomas and aneurysms |
- Kanski's Clinical Ophthalmology, 10th ed.
Surrounding Layers
- Innermost: delicate, vascular pia mater
- Middle: arachnoid mater (subarachnoid space contains CSF, continuous with cerebral CSF)
- Outermost: dura mater (fuses with the sclera anteriorly and the periosteum of the optic canal)
Blood Supply
- Ophthalmic artery (from internal carotid artery) runs inferior to the optic nerve in the optic canal
- Central retinal artery enters the optic nerve 8-12 mm behind the globe, supplying the inner retina
- Optic nerve head receives blood from the circle of Zinn-Haller (fed by posterior ciliary arteries, choroidal vessels, and the pial arterial network)
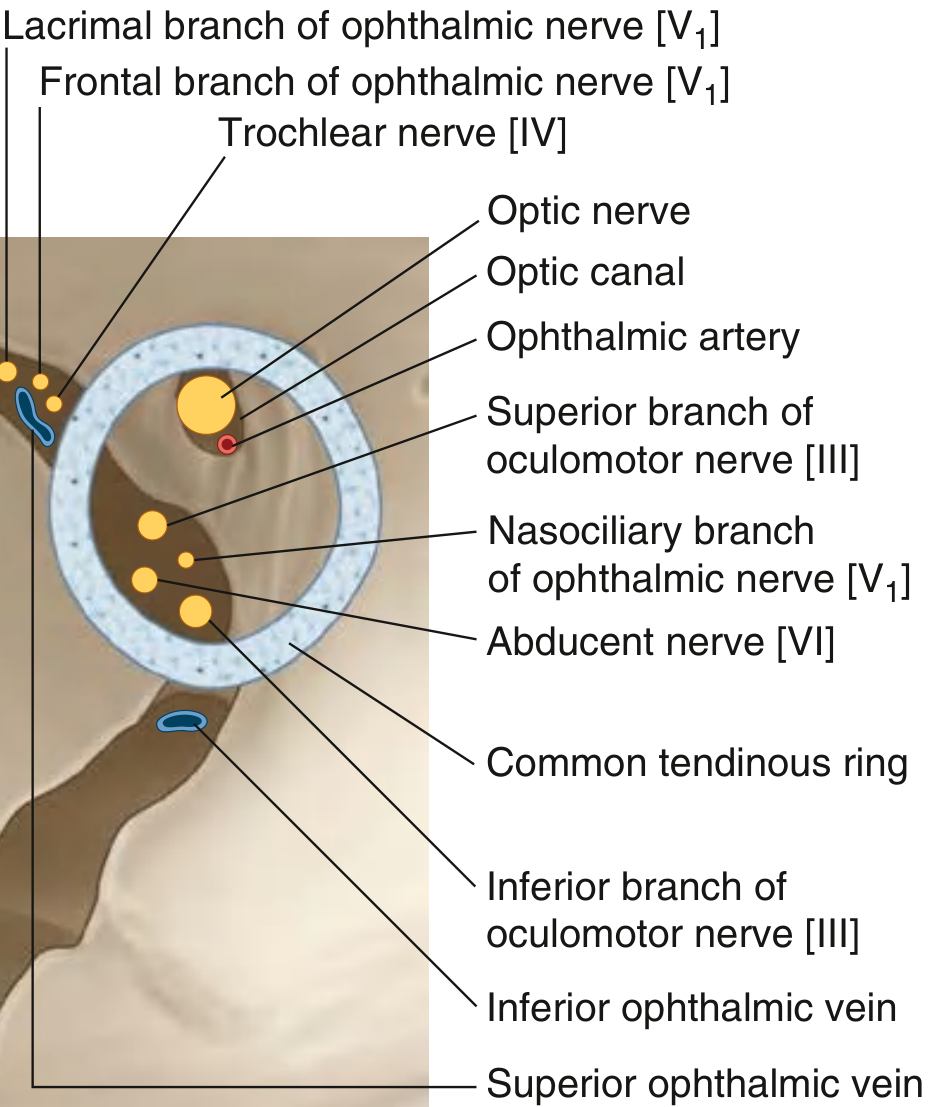
Course and Optic Canal
The nerve leaves the orbit through the optic canal, accompanied by the ophthalmic artery. The diagram below shows its relationship to other orbital structures:
The Visual Pathway
From the retina, visual information travels through a series of relay stations:
- Retina - ganglion cell axons form the optic nerve
- Optic chiasm - nasal retinal fibers (carrying temporal visual field) cross to the opposite side; temporal retinal fibers (carrying nasal visual field) remain ipsilateral
- Optic tract - carries visual information from the contralateral visual hemifield of both eyes
- Lateral geniculate nucleus (LGN) - primary thalamic relay
- Optic radiation - axons project to the primary visual cortex (V1) in the occipital lobe
- Primary visual cortex (Brodmann area 17, calcarine cortex)
- Eric Kandel, Principles of Neural Science, 6th ed.
Visual Field Defects by Lesion Location
| Level of Lesion | Visual Field Defect |
|---|---|
| Optic nerve (unilateral) | Total monocular blindness (ipsilateral eye) |
| Optic chiasm | Bitemporal hemianopia (loss of both temporal fields) |
| Optic tract | Contralateral homonymous hemianopia |
| Meyer's loop (temporal lobe) | Upper contralateral quadrantic anopia ("pie in the sky") |
| Visual cortex (upper calcarine bank) | Contralateral inferior quadrantic deficit |
| Visual cortex (lower calcarine bank) | Contralateral superior quadrantic deficit |
Key rule: Lesions of the retina and optic nerve produce defects in the ipsilateral eye only. Only a chiasmal lesion produces a bilateral field defect with crossing pattern. - Localization in Clinical Neurology, 8e; Bradley & Daroff's Neurology
Papilledema and Intracranial Pressure
Because the subarachnoid space surrounding the optic nerve is continuous with the cerebral CSF, any rise in intracranial pressure transmits into this perineural space. This impedes venous return through the retinal veins, causing papilledema (optic disc edema) - visible on fundoscopy. This is why fundoscopy is a key clinical tool for assessing raised ICP. - Gray's Anatomy for Students
Signs of Optic Nerve Dysfunction
- Reduced visual acuity (non-specific but common)
- Relative afferent pupillary defect (RAPD) - a key objective sign
- Dyschromatopsia - impaired color vision, classically red-green; easily tested with Ishihara plates
- Diminished light brightness sensitivity (may persist after acuity recovers, e.g., post-optic neuritis)
- Diminished contrast sensitivity
- Visual field defects - central scotomas, centrocecal scotomas, arcuate/nerve fiber bundle defects, altitudinal defects
Visual Evoked Potential (VEP)
A functional test that records electrical activity of the visual cortex in response to retinal stimulation. Used to:
- Assess optic neuropathy (especially demyelination)
- Monitor visual function in infants
- Investigate functional (non-physiological) visual loss
In optic neuropathy: prolonged latency and decreased amplitude are found. - Kanski's Clinical Ophthalmology, 10th ed.
Clinical Disorders of CN II
1. Optic Neuritis
- Demyelinating inflammation of the optic nerve
- Presents with painful, subacute monocular vision loss + RAPD + dyschromatopsia
-
50% of patients eventually develop multiple sclerosis
- Retrobulbar neuritis: disc looks normal initially but central/paracentral scotoma present
- Optic neuritis from MS is not steroid-responsive; treat underlying MS
- Also seen in: SLE, vasculitis, sarcoidosis (may be steroid-responsive), neuromyelitis optica (NMO) (with anti-AQP4 antibodies + transverse myelitis)
2. Ischemic Optic Neuropathy
- Non-arteritic (NAION): small vessel disease; associated with hypertension (50%) and diabetes (25%); causes altitudinal visual field defect
- Arteritic (AAION): usually giant cell arteritis (GCA); consider in patients >50 years; treat with oral glucocorticoids
3. Compressive Optic Neuropathy
- Tumors or space-occupying lesions between orbit and chiasm cause gradual central vision loss or sector field defect
- Chronic compression leads to optic atrophy
- Pituitary adenomas can compress the intracranial segment
4. Toxic/Nutritional Optic Neuropathy
- Ethambutol (TB treatment): dose/duration-dependent; bilateral painless blurring, red-green dyschromatopsia; dose should not exceed 15 mg/kg/day; baseline and 6-monthly screening recommended
- Isoniazid: rare toxic optic neuropathy, risk higher when combined with ethambutol
- Methanol poisoning, tobacco amblyopia
- B-vitamin deficiency (especially thiamine)
5. Leber Hereditary Optic Neuropathy (LHON)
-
Mitochondrial inheritance
-
Bilateral central/cecocentric scotomas
-
Young males predominantly affected
-
Goldman-Cecil Medicine; Kanski's Clinical Ophthalmology, 10th ed.
Summary Table
| Feature | Detail |
|---|---|
| Type | Extension of brain (not a true cranial nerve) |
| Function | Special somatic afferent - vision |
| Fiber count | ~1.2 million |
| Entry to skull | Optic canal (with ophthalmic artery) |
| Relay station | Lateral geniculate nucleus |
| End target | Primary visual cortex (occipital lobe, area 17) |
| Meningeal covering | All three meninges + CSF-filled subarachnoid space |
| Key reflex | Afferent limb of pupillary light reflex |
Grading for anti gravity muscle in human body
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
MRC Grading of Muscle Strength - Focus on Antigravity Function
The MRC Scale (Medical Research Council Scale)
The MRC scale, proposed by the Medical Research Council of Great Britain, is the most widely used system for grading muscle power. It recognizes 6 grades (0-5):
| Grade | Description | Clinical Meaning |
|---|---|---|
| 0 | No muscle contraction visible | Complete paralysis |
| 1 | Flicker or trace of contraction, but no movement | Muscle fires but cannot move the joint |
| 2 | Active joint movement with gravity eliminated | Muscle too weak to overcome gravity |
| 3 | Active movement against gravity (full ROM) | Antigravity threshold - can lift against gravity but not resistance |
| 4 | Active movement against gravity AND resistance, but weaker than normal | Submaximal strength |
| 5 | Normal power | Full strength against full resistance |
- Adams and Victor's Principles of Neurology, 12th ed.; Localization in Clinical Neurology, 8e; Bailey and Love's Surgery, 28th ed.
The Antigravity Threshold - Grade 3
Grade 3 is the "antigravity grade" - the precise point at which a muscle can move the joint through its full range of motion against gravity alone, but cannot overcome any additional manual resistance.
- At Grade 2 and below: the limb must be supported horizontally (gravity eliminated) to observe active movement
- At Grade 3: the patient can lift the limb against gravity, e.g., raising the arm or leg off the bed
- At Grade 4 and above: movement is also possible against examiner's resistance
As described in Firestein & Kelley's Rheumatology: "grade 3, antigravity function" - this is the pivotal dividing line in clinical assessment.
Modified MRC Grading (with +/- Subdivisions)
Grade 4 is the broadest grade and is frequently subdivided in clinical practice:
| Grade | Meaning |
|---|---|
| 4- | Movement against gravity + minimal resistance (just overcomes gravity + a little more) |
| 4 | Movement against moderate resistance |
| 4+ | Movement against strong resistance but still less than normal |
| 3+ | Can hold against gravity with brief resistance only |
| 3- | Can complete range of motion against gravity but barely |
"Further gradations may be added, specified as 4+ for barely detectable weakness and 4- for easily detected weakness, 3+ and 3-, and so on." - Adams and Victor's Principles of Neurology, 12th ed.
What Are Antigravity Muscles?
Antigravity muscles are those that resist the pull of gravity to maintain upright posture and body position. In neurological terms:
In the Lower Motor Neuron context:
- Lower limbs: Extensors (quadriceps, hip extensors, plantar flexors/gastrocnemius) - maintain the leg extended against gravity during standing and walking
- Upper limbs: Flexors (biceps, wrist and finger flexors) - resist gravity when the arm is held up
Physiological control:
-
Controlled by the vestibulospinal tract and medial reticulospinal tract, which facilitate alpha and gamma motor neurons of antigravity muscles
-
The vestibular nuclei transmit strong excitatory signals to antigravity muscles via the lateral and medial vestibulospinal tracts
-
These muscles have a particularly high density of muscle spindles and are strongly driven by the gamma efferent system
-
Guyton & Hall Textbook of Medical Physiology; Localization in Clinical Neurology, 8e
In UMN (spasticity) pattern:
Spasticity preferentially affects antigravity muscles:
- Upper limb: Flexors (biceps, wrist flexors) - patient develops flexed arm posture
- Lower limb: Extensors (quadriceps, calf muscles) - patient develops extended leg posture
"Spasticity predominates in antigravity muscles (flexors of the upper extremities and extensors of the lower extremities)." - Localization in Clinical Neurology, 8e
Practical Testing Tips
- Grade 2 testing: Lay the limb horizontally on a flat surface (eliminating gravity), then ask for movement - this is gravity-eliminated position
- Grade 3 testing: Have the patient lift the limb vertically against gravity (e.g., straight leg raise, arm elevation)
- Grade 4 testing: Apply progressive manual resistance to the movement
- For trunk and girdle muscles (large, powerful): Manual resistance alone may miss mild weakness - have the patient perform functional tasks: squatting, rising from a chair, walking on toes/heels
- For hand muscles: Use a dynamometer for quantification
- Adams and Victor's Principles of Neurology, 12th ed.
Decerebrate Rigidity and Antigravity Muscles
When the brainstem is sectioned below the mid-mesencephalon (decerebrate state), rigidity develops specifically in the antigravity muscles - the neck, trunk extensors, and leg extensors. This is caused by unopposed activity of the pontine excitatory reticular system, demonstrating just how heavily these muscles are driven by descending facilitatory tracts. - Guyton & Hall Medical Physiology
Summary: MRC Grade vs. Antigravity
Grade 0 ——— No contraction
Grade 1 ——— Trace contraction only
Grade 2 ——— Movement ONLY with gravity eliminated
← ANTIGRAVITY THRESHOLD →
Grade 3 ——— Full movement AGAINST gravity (no resistance)
Grade 4 ——— Against gravity + resistance (submaximal)
Grade 5 ——— Normal (full) power
Clinical shorthand: A patient "antigravity" means Grade 3 or above. "Below antigravity" means Grade 0, 1, or 2 - the limb cannot be lifted against gravity.
How about sternocleidomastoid muscle, is there any other gradings than mrc
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Searching the Web
sternocleidomastoid muscle grading systems beyond MRC Kendall neck flexor testing
Finding Sources
Finding Sources
Finding Sources
Searching the Web
Kendall Daniels Worthingham muscle grading scale neck SCM sternocleidomastoid specific position testing
I now have comprehensive data. Let me compile a thorough, well-structured answer.
Sternocleidomastoid (SCM) Muscle - Anatomy, Testing, and Grading Systems
Anatomy & Function Recap
The SCM is innervated by CN XI (spinal accessory nerve) + C2 cervical plexus branches.
Actions:
-
Unilateral: Rotates the head to the contralateral side + tilts/laterally flexes toward the ipsilateral shoulder
-
Bilateral: Flexes the neck (draws the chin toward the chest)
-
Localization in Clinical Neurology, 8e
How to Test the SCM
Rotation Test (Unilateral SCM)
- Patient turns their head to one side against the examiner's resistance
- The contralateral SCM contracts and should be visible and palpable
- e.g., to test the right SCM: instruct the patient to rotate the head to the left against resistance
Flexion Test (Bilateral SCM)
- Patient in supine; lifts the head off the bed (chin tuck/head raise)
- Both SCMs contract simultaneously
- Assessed for bilateral symmetry and ability to hold against resistance
Lateral Flexion Test
-
Patient tilts the head toward one shoulder against resistance
-
The ipsilateral SCM contracts
-
Localization in Clinical Neurology, 8e
Grading Systems Beyond the MRC
There are three principal manual muscle testing (MMT) grading systems in clinical use. All of them apply to the SCM and all neck muscles:
1. MRC Scale (Medical Research Council)
The standard 0-5 scale already discussed. Applied to SCM as to any other muscle.
2. Kendall & McCreary Scale (0-100% / Percentage Scale)
Designed to test a specific muscle in isolation rather than movement in general. Requires the examiner to align resistance precisely along the muscle's line of pull and demands selective muscle recruitment by the patient.
| Kendall % | MRC Equivalent | Description |
|---|---|---|
| 100% | 5 | Holds test position against maximal resistance |
| 80% | 4 | Holds test position against moderate resistance |
| 50% | 3 | Holds test position against gravity only (antigravity) |
| 20% | 2 | Moves through full ROM with gravity eliminated |
| 5% | 1 | Visible/palpable contraction, no movement |
| 0% | 0 | No contraction |
For the SCM specifically (Kendall approach):
- The patient must selectively recruit the SCM while the examiner palpates it
- Resistance is applied along the precise vector of the muscle's fiber direction
- This approach is more anatomically specific but demands greater examiner skill
3. Daniels & Worthingham Scale (Named/Functional Grades)
More functional - tests a movement (using all agonists + synergists), with named grades plus +/- subdivisions:
| Kendall % | MRC | Daniels & Worthingham | Description |
|---|---|---|---|
| 100% | 5 | Normal (N) | Full ROM against gravity + maximal resistance |
| ~90% | 4+ | Good+ (G+) | Holds against moderate-to-strong resistance |
| 80% | 4 | Good (G) | Full ROM against gravity + moderate resistance |
| ~70% | 4- | Good- (G-) | Holds against slight-to-moderate resistance |
| ~60% | 3+ | Fair+ (F+) | Holds against gravity + slight resistance |
| 50% | 3 | Fair (F) | Full ROM against gravity only |
| ~40% | 3- | Fair- (F-) | Gradual release from antigravity position |
| ~30% | 2+ | Poor+ (P+) | Partial ROM against gravity OR full ROM gravity-eliminated + holds against pressure |
| 20% | 2 | Poor (P) | Full ROM with gravity eliminated |
| ~10% | 2- | Poor- (P-) | Less than full ROM in gravity-eliminated position |
| 5% | 1 | Trace (T) | Palpable contraction, no movement |
| 0% | 0 | Zero (Z) | No contraction |
Key Differences Between the Three Systems
| Feature | MRC | Daniels & Worthingham | Kendall & McCreary |
|---|---|---|---|
| Scale | 0-5 | Named grades + +/- (0-5 range) | 0-100% |
| Tests | Movement | Movement (all agonists) | Specific muscle isolation |
| Subdivisions | + and - can be added | + and - built in | Percentage intervals |
| Best for | Quick clinical assessment, neurology | Rehabilitation, PT | Specific muscle dysfunction, anatomy research |
| SCM position | Supine (gravity eliminated for grade 2) | Supine/sitting | Supine, precise fiber alignment |
4. IMACS 10-Point Scale (Myositis-Specific)
For inflammatory myopathies (e.g., polymyositis, dermatomyositis), the International Myositis Assessment and Clinical Studies (IMACS) group uses a 10-point extrapolation of the MRC 5-point scale, providing finer discrimination between grades - particularly useful for tracking treatment responses in neck flexor weakness.
- Rheumatology, 2-Volume Set (Elsevier, 2022)
5. Dynamometry
For quantitative SCM strength (in Newtons or kg), handheld dynamometers or isokinetic devices measure force objectively. This removes the subjectivity of manual grading and allows tracking of small incremental changes - especially useful in research settings and neuromuscular disease monitoring.
SCM-Specific Clinical Correlations
| Finding | Interpretation |
|---|---|
| Unilateral SCM weakness (cannot rotate head contralaterally) | CN XI lesion (ipsilateral) - e.g., after neck surgery, trauma |
| Bilateral SCM weakness (head falls back on standing) | Bilateral CN XI or cervical spine lesion, motor neuron disease, myopathy |
| SCM spasm/shortening | Torticollis (wry neck), especially in infants (congenital muscular torticollis) |
| Spasticity with UMN lesion | SCM (a neck flexor) may be relatively spared as UMN lesions preferentially affect antigravity muscles |
"Bilateral sternocleidomastoid paresis causes weakness of neck flexion, with the head tending to fall backward when the patient attempts to stand erect." - Localization in Clinical Neurology, 8e
Summary
| System | Grade for "antigravity SCM" | Notes |
|---|---|---|
| MRC | Grade 3 | Can raise head off bed against gravity |
| Daniels & Worthingham | Fair (F) / Grade 3 | Same threshold, named grades |
| Kendall | 50% | Muscle holds test position against gravity |
| IMACS | ~5/10 | Used in myositis only |
| Dynamometry | Measured in N/kg | Objective, research-grade |
This is a shared conversation. Sign in to Orris to start your own chat.