Ultrasonography genetics
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material. Let me compile the full, detailed overview.
Ultrasonography and Genetics: A Comprehensive Overview
Prenatal ultrasonography sits at the intersection of imaging and clinical genetics. It serves as the primary non-invasive window into fetal anatomy, and its findings directly guide genetic testing, counseling, and management decisions. Below is a structured overview of the entire topic.
1. The Role of Ultrasound in Prenatal Genetic Screening
Ultrasound does not diagnose a genetic disorder on its own - it identifies structural markers and anomalies that raise or lower the probability of a chromosomal or single-gene disorder. When combined with biochemical markers and, increasingly, cell-free DNA (cfDNA) analysis, it forms the backbone of the prenatal screening pathway.
Ultrasonography cannot detect disorders whose phenotype:
- Develops only after birth (e.g., many metabolic disorders)
- Has no structural/imaging component (e.g., most intellectual disability syndromes without dysmorphic features)
2. First-Trimester Screening
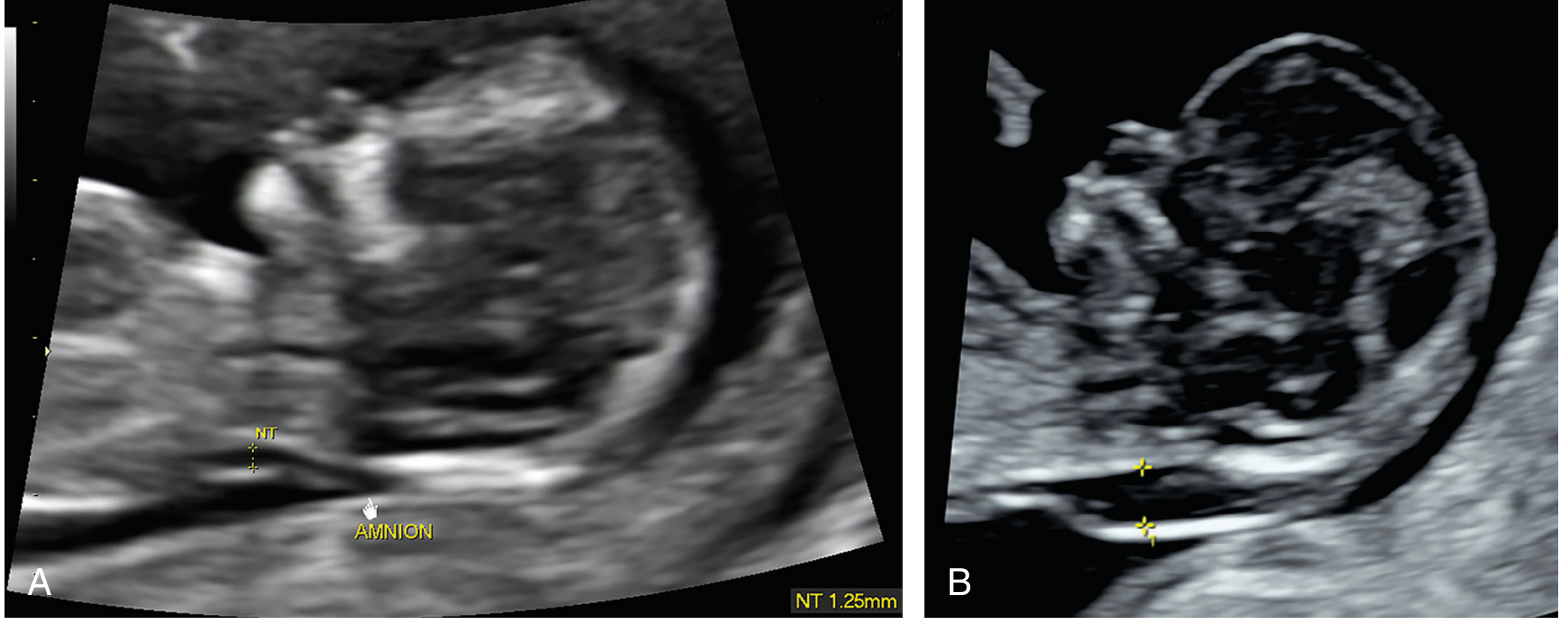
Nuchal Translucency (NT)
NT is the echo-free fluid space beneath the fetal skin in a sagittal view, measured between 11+0 and 13+6 weeks.
- Normal values: ~1.2 mm at 11 weeks (95th percentile ≤2 mm); ~1.5 mm at 14 weeks (95th percentile ≤2.6 mm)
- An increased NT is associated with a wide spectrum of genetic conditions (see table below)
Common causes of increased NT thickness (from Thompson & Thompson Genetics, 9th ed.):
| Category | Examples |
|---|---|
| Chromosomal aneuploidy | Trisomies 21, 13, 18; Monosomy X; Triploidy |
| Pathogenic copy number variants | Microdeletions/microduplications |
| Congenital heart defects | Structural CHD |
| RASopathies | Noonan syndrome, Costello syndrome |
| Skeletal dysplasias | Thanatophoric dysplasia, osteogenesis imperfecta |
| Other single-gene disorders | Varied |
Combined First-Trimester Screening
When NT is combined with maternal serum markers (free beta-hCG + PAPP-A) and maternal age, the combined first-trimester screen achieves:
- ~85-93% detection rate for trisomy 21 at a 5% false-positive rate (data from major trials: BUN, FASTER, SURUSS, Nicolaides 2005 - pooled 167,210 pregnancies, DR 88.2%)
Nasal Bone Assessment (Creasy & Resnik's Maternal-Fetal Medicine)
The fetal nasal bone (NB) can be assessed in the first trimester. Its absence correlates with trisomy 21:
- NB absent in 73% of trisomy 21 fetuses vs. only 0.5% of euploid fetuses
- Absent NB increases the likelihood of trisomy 21 by 87-fold
- Adding NB to maternal age + NT raises detection to ~93% (FPR 5%) or ~85% (FPR 1%)
- Caveat: NB absence is more common in fetuses of African ancestry (~9% of euploid African fetuses), so ethnicity-adjusted LRs are used
3. Second-Trimester Screening
Quadruple Screen (Quad Screen)
Measures four maternal serum analytes at 15-20 weeks:
| Analyte | Trisomy 21 | Trisomy 18 |
|---|---|---|
| MSAFP | ↓ | ↓ |
| uE3 (unconjugated estriol) | ↓ | ↓ |
| hCG | ↑ | ↓ |
| Inhibin A | ↑ | normal |
- A very low uE3 can indicate rare conditions: steroid sulfatase deficiency, Smith-Lemli-Opitz syndrome
- Screen-positive cutoff is usually set at a false-positive rate <5%
Second-Trimester Ultrasound "Soft Markers"
Soft markers are minor anatomical variants that individually have low predictive value but, when combined, modify aneuploidy risk:
- Echogenic intracardiac focus (EIF)
- Choroid plexus cysts (CPC - associated with trisomy 18)
- Short femur or humerus
- Pyelectasis
- Sandal-gap toe (wide gap between 1st and 2nd toe - Down syndrome)
- Echogenic bowel
4. Major Structural Anomalies by Aneuploidy
The table below summarizes the typical major anomalies visible on prenatal ultrasound for the four most common aneuploidies (Thompson & Thompson Genetics, 9th ed.):
| Trisomy 21 | Trisomy 13 | Trisomy 18 | Monosomy X (45,X) |
|---|---|---|---|
| 50% have sonographic findings | 80-90% have findings | 80-90% have findings | Up to 90% have findings |
| Cystic hygroma | Cystic hygroma | Cystic hygroma | Cystic hygroma |
| CHD (VSD, AVSD) | CHD | CHD (polyvalvular disease) | CHD (HLHS, aortic coarctation) |
| Duodenal atresia ("double bubble") | Polydactyly | Clenched fist | Renal anomalies (horseshoe kidney) |
| Wide gap 1st-2nd toe | Holoprosencephaly | Omphalocele | Hydrops |
| Cleft lip/palate | Omphalocele | Rocker-bottom feet | Foot edema |
| Cleft lip/palate | Fetal growth restriction |
5. Ultrasound in Single-Gene and Multifactorial Disorders
Ultrasound can raise suspicion for specific single-gene disorders even when chromosomes are normal:
Skeletal Dysplasias
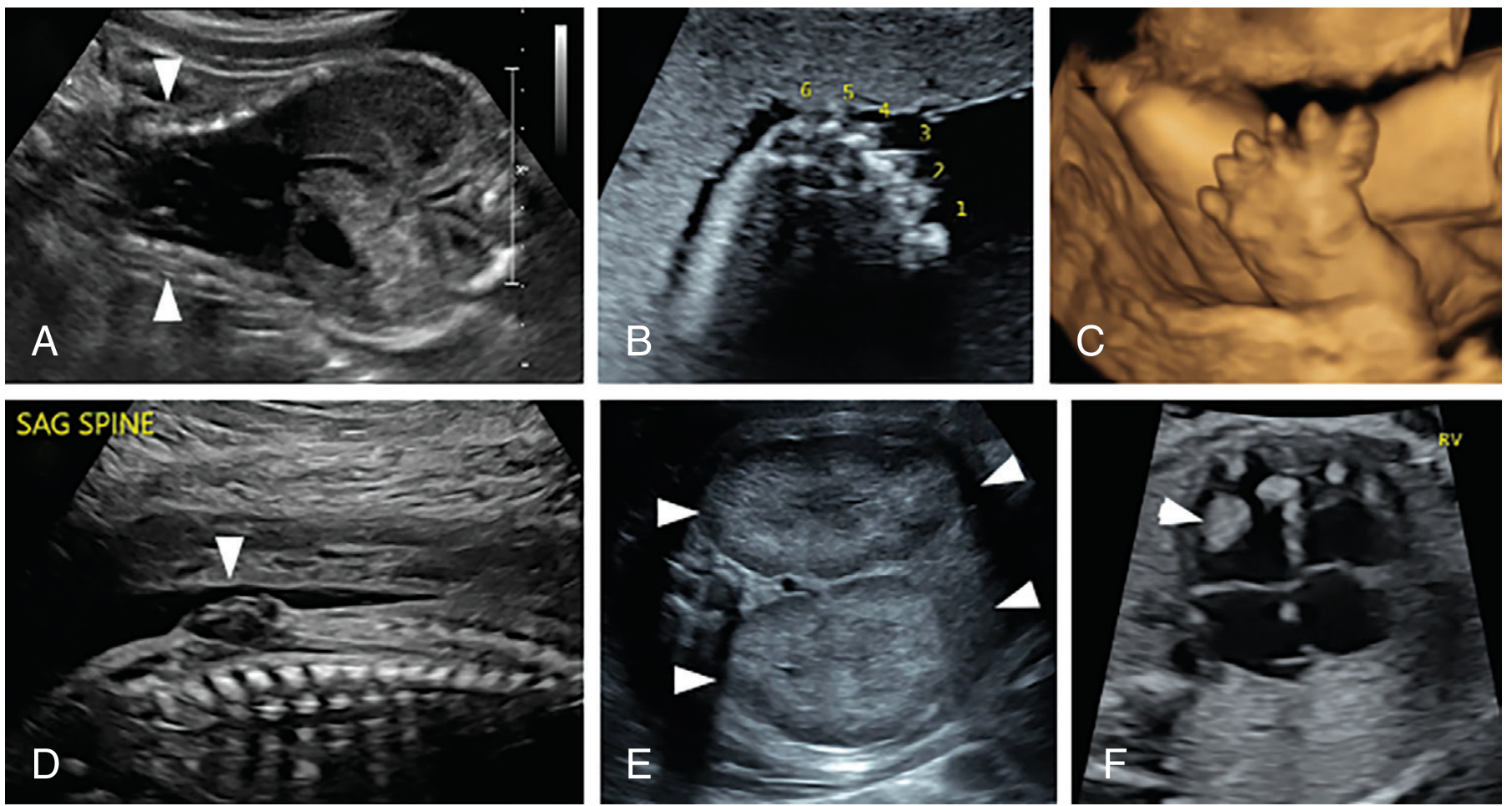
- Thanatophoric dysplasia (FGFR3 gain-of-function): very short limbs, cloverleaf skull, small chest
- Osteogenesis imperfecta (COL1A1/COL1A2 mutations): fractures, bowing of limbs, narrow chest (see image D above)
- Long-bone measurements (femur, humerus, tibia) plotted against gestational age are key; significant shortening below the 5th percentile triggers genetic workup
Multifactorial / Complex Disorders Detected by Ultrasound
- Neural tube defects (NTDs): meningomyelocele, anencephaly - recurrence risk ~2-5% (multifactorial)
- Cleft lip/palate: recurrence risk ~4%
- Congenital heart defects (CHD): detected by fetal echocardiography; triggers further genetic workup (fetal indications: chromosome abnormality, NT thickening, arrhythmia, hydrops)
X-linked Disorders
- Ultrasound can determine fetal sex as early as 13 weeks
- This guides decisions about genetic testing for X-linked recessive carriers (e.g., hemophilia, Duchenne muscular dystrophy)
- cfDNA can screen fetal chromosomal sex from 10 weeks
Specific Syndromes
- Tuberous sclerosis: cardiac rhabdomyomas visible on fetal echo
- Infantile polycystic kidney disease: markedly enlarged, echogenic kidneys
- Hydrops fetalis: skin edema, ascites, pleural/pericardial effusion - can signal lysosomal storage disorders, RASopathies, or chromosomal abnormalities
6. Diagnostic Testing Triggered by Ultrasound Findings
When ultrasound identifies a structural anomaly or increased NT, the following diagnostic tests are offered:
| Test | What it detects | Timing |
|---|---|---|
| Chorionic villus sampling (CVS) | Chromosomes, CMA, single-gene | 10-13 weeks |
| Amniocentesis | Chromosomes, CMA, single-gene, exome | ≥15 weeks |
| Chromosomal microarray (CMA) | Aneuploidy + copy number variants (CNVs) | Added to CVS/amnio |
| Exome/genome sequencing | Single-gene disorders, when CMA negative | After structural anomaly with normal CMA |
| cfDNA (NIPT) | Screening only - trisomy 21, 18, 13, sex aneuploidies | From 10 weeks |
Key principle from Thompson & Thompson: cfDNA is a screening test, not a diagnostic test. CVS or amniocentesis with CMA is more expansive - it surveys the entire genome for aneuploidy and pathogenic copy number variants. A positive NIPT must be confirmed with diagnostic sampling.
7. Copy Number Variants (CNVs) and CMA
When structural anomalies are found on ultrasound but standard karyotype is normal, CMA detects an additional ~6% of clinically significant CNVs not visible on routine karyotype. Common genomic disorders that may present with ultrasound findings include:
| Locus | Deletion Syndrome | Duplication Syndrome |
|---|---|---|
| 7q11.23 | Williams-Beuren syndrome | WBS duplication syndrome |
| 15q11-q13 | Angelman / Prader-Willi | 15q11-q13 duplication |
| 16p11.2 | 16p11.2 deletion (autism/ID) | 16p11.2 duplication |
| 17p11.2 | Smith-Magenis syndrome | Potocki-Lupski syndrome |
| 22q11.2 | DiGeorge/velocardiofacial | 22q11.2 duplication |
(Data: Creasy & Resnik's Maternal-Fetal Medicine, Table 2.1)
8. Genetic Counseling Principles
Before and after any genetic test triggered by ultrasound findings, counseling addresses (Thompson & Thompson Genetics, 9th ed.):
- The reason/indication for testing and alternative options
- The risk that the fetus is affected
- The nature and prognosis of the condition tested
- The risks and limitations of the procedure
- The possibility of a variant of uncertain significance (VUS) - a result of unknown clinical significance
- The possibility of incidental/secondary findings and the option to opt out
- Personal, ethical, religious, and social considerations
Summary: The Screening Pathway
Maternal age + family history
↓
First-trimester combined screen (NT + PAPP-A + free β-hCG ± nasal bone)
↓
If high risk → cfDNA (NIPT) for confirmation, or proceed directly to CVS
↓
Second-trimester anatomy scan (18-22 weeks)
↓
Soft markers or structural anomaly → amniocentesis + CMA
↓
CMA normal but anomaly persists → exome/genome sequencing
- Thompson & Thompson Genetics and Genomics in Medicine, 9th ed., Chapter 18
- Creasy & Resnik's Maternal-Fetal Medicine, Chapters 2 and 30
This is a shared conversation. Sign in to Orris to start your own chat.