Physiology of pain saq mbbs
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content needed for a complete, exam-ready SAQ answer. Here it is:
Physiology of Pain - MBBS SAQ
Definition
Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage. It is both a sensation and an emotion - acute pain is accompanied by behavioral arousal, elevated BP, heart rate, pupil dilation, and cortisol release. - Harrison's Principles of Internal Medicine, 22E
Types of Pain
| Type | Character | Fiber | Speed |
|---|---|---|---|
| Fast (First) Pain | Sharp, pricking, well-localized | Aδ (thin myelinated) | ~15 m/s |
| Slow (Second) Pain | Dull, burning, aching, poorly localized | C (unmyelinated) | 0.5-2 m/s |
1. Peripheral Mechanisms - Nociceptors
Nociceptors are free nerve endings (peripheral terminations of sensory neurons) found in skin, connective tissue, blood vessels, periosteum, and most visceral organs.
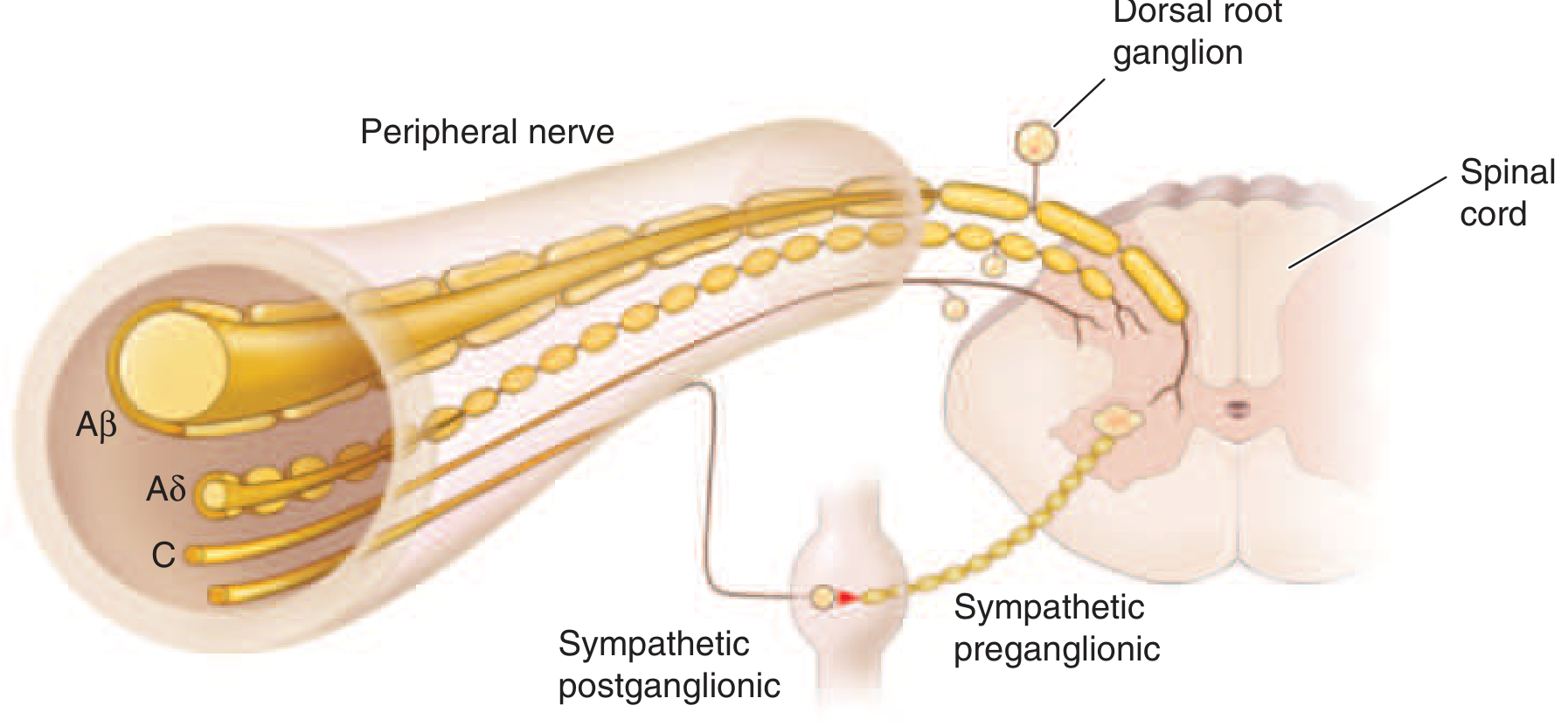
Fiber types in a peripheral nerve. Aβ: large myelinated (non-pain); Aδ: small myelinated (fast pain); C: unmyelinated (slow pain). - Harrison's Principles of Internal Medicine, 22E
Three categories of nociceptors:
- Mechanoreceptors - respond to intense mechanical stimuli; transmitted by Aδ fibers
- Thermoreceptors - respond to extreme heat/cold; mainly C fibers
- Polymodal nociceptors - respond to mechanical, thermal, and chemical stimuli; C fibers (majority)
Adequate stimuli differ by tissue:
- Skin: pricking, cutting, crushing, burning, freezing
- Viscera: distension, ischemia, inflammation (NOT cutting)
- Muscle: ischemia (e.g., intermittent claudication), spasm
- Joints: synovial inflammation, ligament tearing
2. Chemical Mediators of Pain (Peripheral)
When tissue is damaged, proteolytic enzymes release pain-producing substances that excite nociceptor terminals:
- Histamine - from mast cells
- Prostaglandins (PGs) - sensitize nociceptors
- Serotonin (5-HT)
- Bradykinin (BK) - one of the most potent algogenic substances
- Potassium ions (K+)
- Leukotrienes
- Substance P - released from C fiber endings; causes vasodilation, edema (mast cell histamine release), and attracts leukocytes -> neurogenic inflammation (axon reflex of Lewis)
3. Sensitization
Peripheral Sensitization
Repeated/prolonged noxious stimuli lower the threshold of nociceptors - they fire more readily and at higher frequency. Caused by BK, PGs, nerve growth factor activating intracellular signaling, increasing membrane insertion of ion channels.
Central Sensitization
Activity generated by peripheral nociceptors enhances excitability of dorsal horn neurons. This leads to:
- Hyperalgesia - increased pain from the same noxious stimulus
- Allodynia - pain from normally innocuous stimuli (e.g., sunburned skin is painful to gentle touch)
Silent nociceptors - Aδ and C fibers in viscera that are normally insensitive but become active during inflammation; explain why visceral disease causes severe pain.
4. Pain Pathways (Spinal Cord and Ascending Tracts)
First-order neurons (Primary afferents)
- Cell bodies in the dorsal root ganglion (DRG)
- Aδ and C fibers enter the dorsal horn and synapse in Rexed laminae I, II, and V
- Aδ fibers: mainly laminae I and V
- C fibers: mainly lamina II (substantia gelatinosa)
Neurotransmitters at dorsal horn
- Excitatory amino acids (glutamate, aspartate)
- Neuropeptides: Substance P, CGRP, CCK
Second-order neurons (Dorsal horn)
- Nociceptive-specific (NS) neurons - respond only to noxious input
- Wide dynamic range (WDR) neurons - respond to both nociceptive and non-nociceptive stimuli
Axons of most second-order neurons cross in the anterior white commissure and ascend in the anterolateral quadrant as the spinothalamic tract (STT).
Two components of the spinothalamic tract:
| Tract | Other name | Thalamic nucleus | Cortex | Pain type |
|---|---|---|---|---|
| Lateral STT | Neospinothalamic | VPL nucleus | Primary sensory cortex (S1) | Fast, well-localized |
| Medial STT | Paleospinothalamic | Central/laminar nuclei (via PAG, brainstem) | Limbic system, insula | Slow, poorly localized, emotional |
Third-order neurons
- VPL -> primary somatosensory cortex (S1), parietal operculum
- Multiple cortical areas activated: S1, S2, thalamus, PAG, supplementary motor, insular cortex (confirmed by fMRI and PET)
5. Gate Control Theory (Melzack and Wall, 1965)
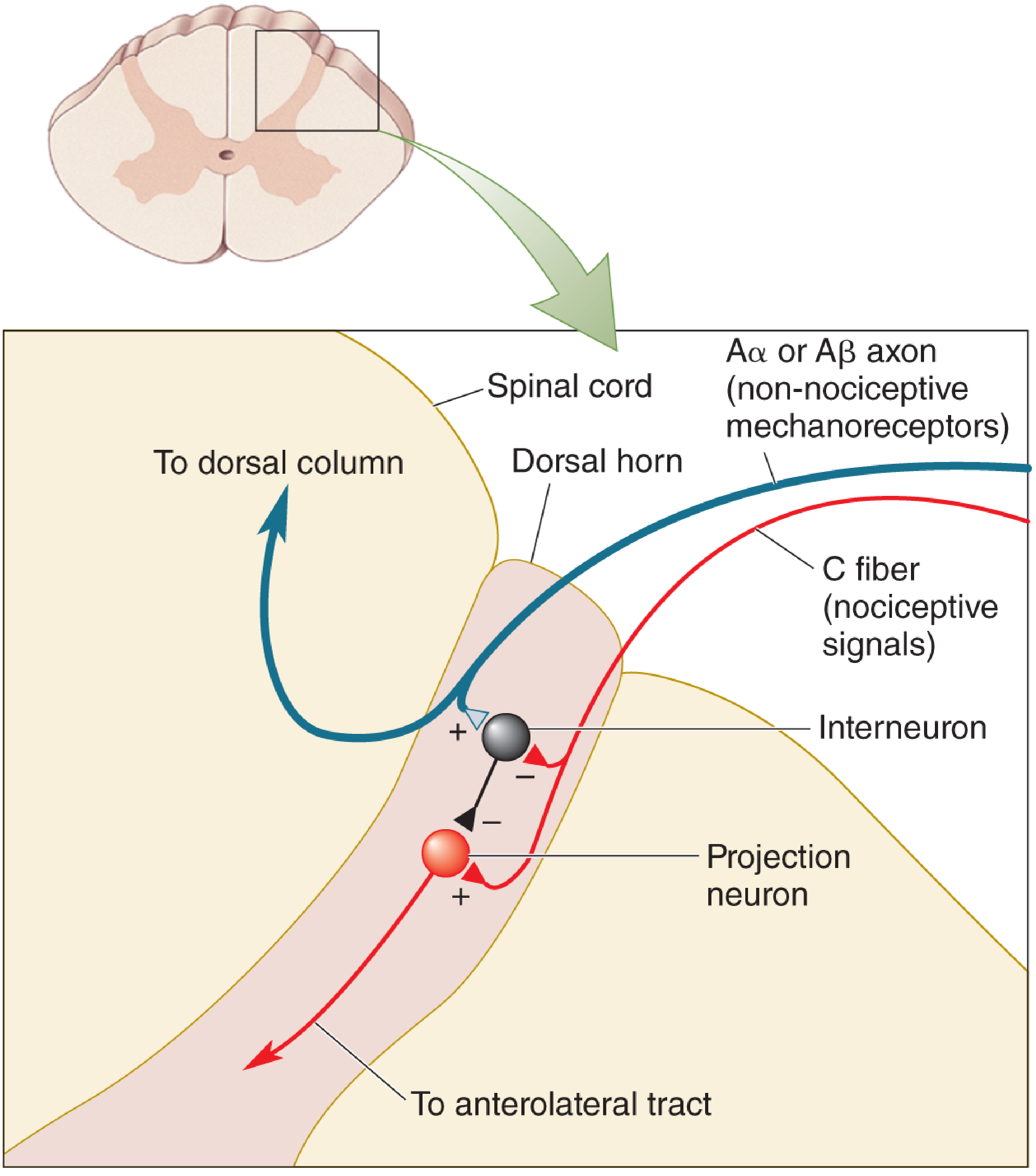
Gate control theory - Neuroscience: Exploring the Brain, 5th Ed.
Concept: The transmission of pain signals from dorsal horn projection neurons is regulated by the balance of input from large-diameter (Aβ) and small-diameter (Aδ/C) fibers, mediated via inhibitory interneurons.
Mechanism:
- Large Aβ fibers (touch) --> excite inhibitory interneurons (I cells) --> close the gate (presynaptic inhibition of T/projection cells) --> pain reduced
- Small C fibers (pain) --> inhibit I cells --> open the gate --> pain transmitted
Clinical application:
- Rubbing injured skin (activates Aβ) reduces pain
- Transcutaneous electrical nerve stimulation (TENS) works on this principle
- Descending modulation from brainstem, thalamus, and limbic lobes also controls the gate
6. Descending Pain Modulation (Endogenous Analgesia)
Emotional stress, fear, or strong distraction can suppress pain via a descending inhibitory system:
- Periaqueductal gray (PAG) - midbrain; receives input from cortex, hypothalamus, amygdala (emotional signals). Key control center.
- PAG --> Raphe nuclei (medulla; serotonergic) and Locus coeruleus (noradrenergic)
- These project down to the dorsal horn, inhibiting nociceptive transmission
Endogenous Opioids
The brain produces three families of morphine-like peptides:
- Endorphins
- Enkephalins
- Dynorphins
These bind to opioid receptors (μ, κ, δ) concentrated in PAG, raphe nuclei, and dorsal horn. Their effects:
- Suppress release of glutamate from presynaptic terminals
- Hyperpolarize postsynaptic neurons
- Net result: block transmission of nociceptive signals through the dorsal horn
Naloxone (opioid antagonist) can block these effects, confirming the opioid mechanism. - Neuroscience: Exploring the Brain, 5th Ed.
7. Perception and Threshold
- Pain threshold = lowest intensity stimulus perceived as pain; approximately equal in all persons
- Inflammation lowers the threshold (sensitization)
- Local anesthetics, opioids, and certain CNS lesions raise the threshold
- Placebos reduce pain in ~1/3 of patients (endogenous opioid release)
- Distraction and suggestion reduce awareness but not the threshold itself
8. Referred Pain
Pain arising from visceral or deep somatic structures is "referred" to a body surface area. Mechanism: visceral and somatic afferents converge on the same second-order (WDR) neurons in the dorsal horn. The brain misidentifies the source as the more familiar somatic structure.
Examples:
- Cardiac ischemia -> left arm/jaw pain
- Appendicitis -> periumbilical (early), then right iliac fossa (late)
- Diaphragmatic irritation -> shoulder tip pain
Summary for SAQ
Pain physiology involves: (1) Peripheral nociceptors (Aδ - fast; C - slow); (2) Chemical mediators (BK, PGs, substance P); (3) Sensitization (peripheral and central); (4) Spinal cord relay (dorsal horn laminae I/II/V -> STT -> thalamus -> cortex); (5) Gate control (Aβ closes, C fibers open the gate); (6) Descending inhibition (PAG -> raphe/locus coeruleus -> dorsal horn, via endorphins/enkephalins).
Sources: Harrison's Principles of Internal Medicine 22E; Adams and Victor's Principles of Neurology, 12th Ed.; Bradley and Daroff's Neurology in Clinical Practice; Neuroscience: Exploring the Brain, 5th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.