What is l2a0a3 in medical
L2A0A3 obstetric notation medical meaning
L2A0A3 - Obstetric Notation Explained
| Code | Meaning |
|---|---|
| L2 | 2 Living children - the woman currently has 2 living children |
| A0 | 0 Abortions (induced/elective) - no history of induced/therapeutic abortions |
| A3 | 3 Abortions (spontaneous/miscarriages) - 3 pregnancy losses before 20 weeks gestation |
Note: When two "A" values appear, the first A typically refers to induced (elective) abortions, and the second A refers to spontaneous abortions (miscarriages).
Context within the Full Obstetric Notation System
- G - Gravida (total number of pregnancies)
- T - Term deliveries (at 37+ weeks)
- P - Preterm deliveries (20-36 weeks)
- A - Abortions/losses (before 20 weeks)
- L - Living children
Putting It Together
- 2 living children
- No induced abortions
- 3 spontaneous abortions (miscarriages)
In male patient
L2A0A3 medical notation male patient meaning classification
"L2" "A0" "A3" leprosy classification Ridley-Jopling OR dermatology male
leprosy disability grading "L2" "A0" "A3" WHO eyes hands feet
L2 A0 A3 - Leprosy WHO Disability Grading
| Code | Region | Grade | Meaning |
|---|---|---|---|
| L2 | Lower limbs (Feet) | Grade 2 | Visible deformity or damage present (e.g., plantar ulcer, foot drop, toe clawing) |
| A0 | Arms/Hands | Grade 0 | No disability - no anesthesia, no visible deformity |
| A3 | Eyes | Grade 3* | Severe visual loss or blindness due to leprosy |
*Some WHO versions use a 0-2 scale for eyes (Grade 2 = severe visual loss/blindness), while others extend to Grade 3.
WHO Leprosy Disability Grading Scale
- Grade 0 - No disability; no anesthesia, no visible deformity
- Grade 1 - Loss of protective sensation (anesthesia) but no visible deformity
- Grade 2 - Visible deformity or damage (ulcers, clawing, contractures, foot drop, lagophthalmos)
Important Note
What is the use of the thyroxine in the congental nephrotic syndrome
thyroxine supplementation congenital nephrotic syndrome thyroid hormone loss mechanism
https://www.endocrine-abstracts.org/ea/0095/ea0095p157
Thyroxine in Congenital Nephrotic Syndrome (CNS)
Why Is Thyroxine Needed?
| Protein Lost in Urine | What It Carries |
|---|---|
| Thyroid-binding globulin (TBG) | Carries ~70% of circulating T4 |
| Transthyretin (TTR/prealbumin) | Carries ~10-15% of T4 |
| Albumin | Carries ~10-15% of T4 |
Purpose of Thyroxine (Levothyroxine) Supplementation
| Goal | Explanation |
|---|---|
| Correct hypothyroidism | Replace the T4 lost in urine to normalize TSH and maintain euthyroid state |
| Protect neurodevelopment | Thyroid hormone is absolutely critical in the first 2-3 years of life for brain maturation; untreated hypothyroidism causes irreversible cognitive impairment |
| Support growth | T4 is needed for normal linear growth and bone maturation in infants |
| Prevent cardiovascular effects | Hypothyroidism causes bradycardia, poor cardiac output, and worsens the already compromised hemodynamics in CNS |
Key Clinical Points
- Higher-than-normal doses are required because the supplemented thyroxine is also being lost in the urine continuously. Doses as high as 17.5 mcg/kg/day (compared to the usual 10-15 mcg/kg/day in standard congenital hypothyroidism) may be needed.
- Frequent monitoring of TFTs (TSH + free T4) is essential, as levels fluctuate with disease activity and albumin infusions.
- Dose adjustment is needed in both directions - increases during active nephrotic syndrome, reductions during remission.
- If the patient undergoes bilateral nephrectomy (done to stop protein loss before renal transplantation), thyroid function can normalize and thyroxine may be tapered/stopped.
- Levothyroxine is typically started early (even in the neonatal period) once abnormal TFTs are detected, since the Guthrie (newborn screening) card will be negative - the baby's thyroid gland is structurally normal.
Summary
In CNS, thyroxine (levothyroxine) is given as replacement therapy for urinary-loss-induced hypothyroidism - not because the thyroid gland is diseased, but because the binding proteins that carry T4 in the blood are being lost through the damaged glomeruli. Without replacement, infants face serious risks of brain damage, growth failure, and cardiovascular compromise.
Gave the management and treatment for the neonatal jaundice
neonatal jaundice management treatment guidelines 2024 phototherapy exchange transfusion
https://emedicine.medscape.com/article/974786-treatment
Management & Treatment of Neonatal Jaundice
Overall Goal
Step 1 - Initial Assessment
| Type | Features |
|---|---|
| Physiological | Appears day 2-3, peaks day 3-5, resolves by 2 weeks (term) |
| Pathological | Appears within 24 hrs, TSB >5 mg/dL on day 1, rising rapidly, or conjugated |
| Breast milk jaundice | Peaks day 10-21, persists 3-10 weeks, otherwise well baby |
- Jaundice within first 24 hours of life
- Elevated direct (conjugated) bilirubin - always pathological
- TSB rising faster than expected or approaching exchange levels
- Jaundice beyond 3 weeks of age
- Sick-appearing infant
- TSB (total serum bilirubin) - fractionated (direct + indirect)
- Transcutaneous bilirubin (TcB) - for screening in well infants >24 hrs
- FBC + peripheral smear
- Direct Coombs (DAT) test - for isoimmune haemolysis
- Blood group (infant and mother)
- Blood glucose, septic screen if sick
Step 2 - General (Supportive) Measures
- Encourage feeding (breast or formula) - stimulates gut motility, reduces enterohepatic circulation of bilirubin
- Adequate hydration - prevents dehydration-related worsening
- Do NOT supplement with water - does not reduce bilirubin and can cause hyponatraemia
- Treat any underlying cause (infection, haemolysis, metabolic disorder)
Step 3 - Phototherapy
Mechanism
When to Start
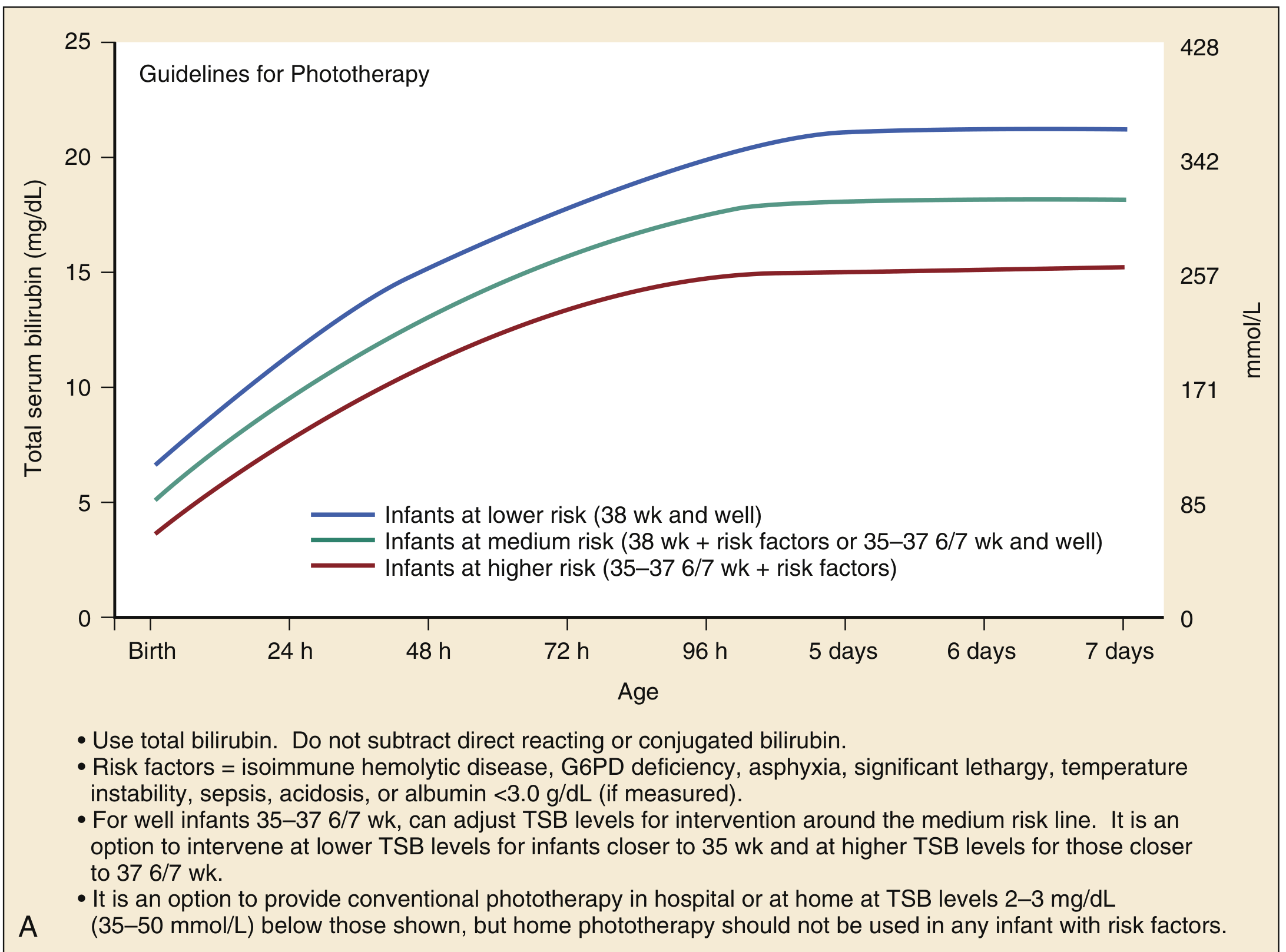
- Isoimmune haemolytic disease (ABO/Rh incompatibility)
- G6PD deficiency
- Asphyxia / significant lethargy
- Temperature instability / sepsis / acidosis
- Albumin <3.0 g/dL
Types of Phototherapy
| Type | Details |
|---|---|
| Conventional | Fluorescent blue-white light (wavelength 430-490 nm), placed 15-20 cm above baby |
| Intensive phototherapy | Maximum irradiance (>30 µW/cm²/nm), multiple lights, fibreoptic blanket below |
| Home phototherapy | Option for low-risk infants when TSB is 2-3 mg/dL below treatment threshold (NOT for infants with risk factors) |
Monitoring
- Check TSB every 4-6 hours initially; extend intervals as bilirubin stabilises
- Discontinue when TSB falls sufficiently below the threshold for the infant's age/risk
- Rebound bilirubin check 12-24 hrs after stopping phototherapy (especially in haemolytic disease)
Step 4 - Intravenous Immunoglobulin (IVIG)
- Dose: 500 mg/kg IV over 2 hours
- Indication: TSB rising rapidly despite intensive phototherapy, or within 2-3 mg/dL of exchange transfusion threshold
- Mechanism: Blocks Fc receptors on macrophages, reducing red blood cell destruction and slowing rate of bilirubin rise
- May be repeated once if needed
- Can reduce the need for exchange transfusion in haemolytic disease
Step 5 - Exchange Transfusion
When to Perform
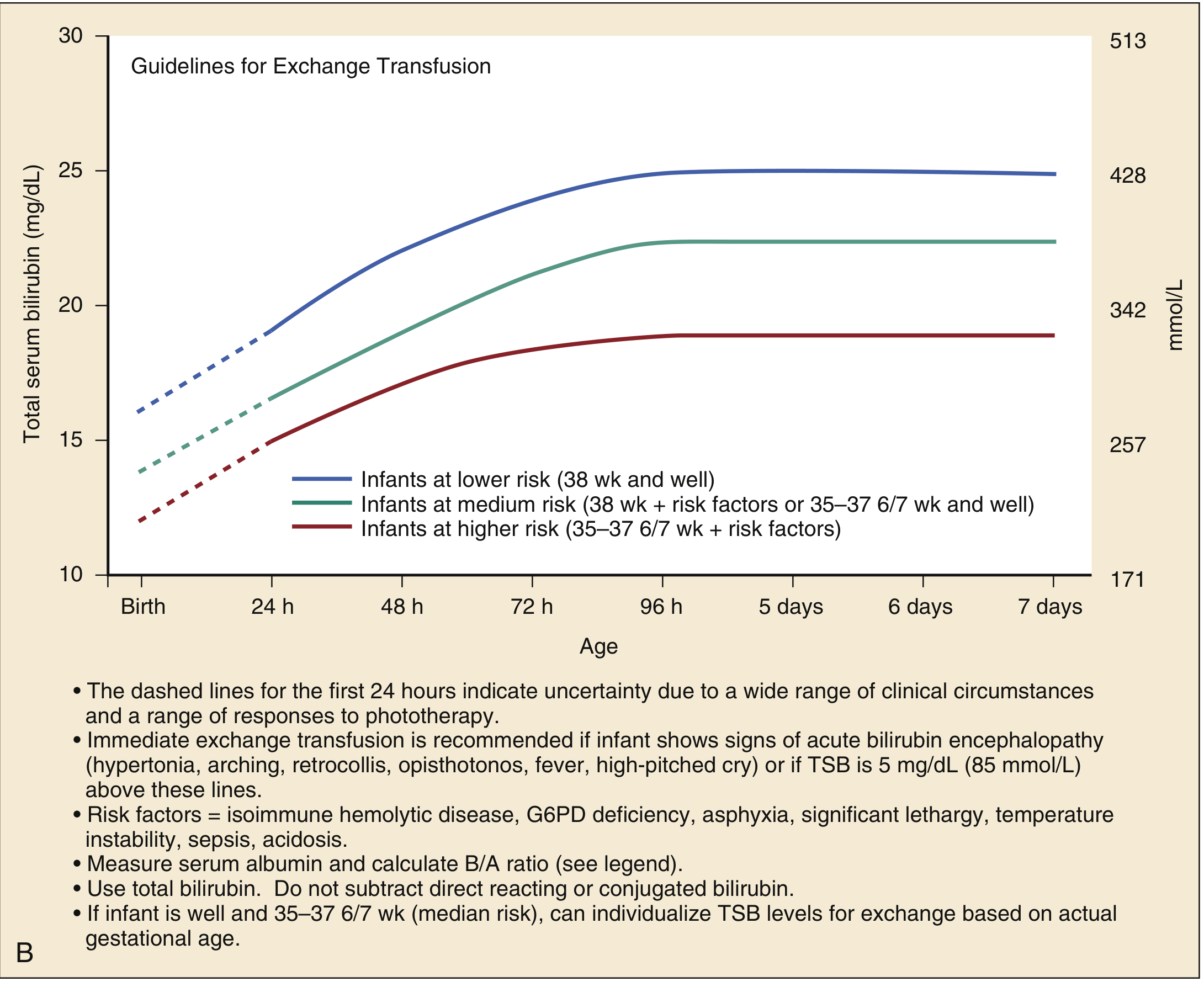
- Signs of acute bilirubin encephalopathy are present (hypertonia, arching, retrocollis, opisthotonos, fever, high-pitched cry)
- TSB is 5 mg/dL (85 µmol/L) above the exchange transfusion threshold line
- TSB continues to rise or remains above threshold despite intensive phototherapy
Procedure (Double-Volume Exchange)
- Uses double the infant's blood volume (~160-200 mL/kg)
- Done via umbilical vein catheter
- Removes sensitised RBCs, bilirubin, and maternal antibodies
- Replaces with O-negative, CMV-negative irradiated packed red cells in fresh frozen plasma
Risks
- Thrombocytopenia, electrolyte imbalance (hypocalcaemia, hyperkalaemia)
- Infection, air embolism, necrotising enterocolitis
- Cardiac arrhythmia, mortality (~0.5-1%)
Step 6 - Additional/Special Treatments
| Situation | Treatment |
|---|---|
| Conjugated (direct) hyperbilirubinemia | Treat underlying cause (biliary atresia → Kasai portoenterostomy; infection → antibiotics) |
| Crigler-Najjar Type I | Phototherapy 12-16 hrs/day + liver transplantation (definitive) |
| Crigler-Najjar Type II | Phenobarbital (induces residual UGT activity) |
| G6PD deficiency | Avoid oxidant drugs/foods; phototherapy/exchange as per bilirubin level |
| Polycythaemia | Partial exchange transfusion with saline |
Summary Algorithm
Neonatal Jaundice
↓
Measure TSB + identify risk factors
↓
Conjugated? → YES → Investigate and treat cause (biliary atresia, infection, metabolic)
↓ NO
Plot TSB on AAP nomogram
↓
Below phototherapy threshold → Monitor + encourage feeding
↓
Above phototherapy threshold → Start PHOTOTHERAPY
↓
Haemolytic disease + rising rapidly → Add IVIG
↓
Above exchange threshold or ABE signs → EXCHANGE TRANSFUSION
Crigler-Najjar Type II Phenobarbital (induces residual UGT activity)
Crigler-Najjar syndrome type II phenobarbital mechanism UGT1A1 treatment
Crigler-Najjar Syndrome Type II - Phenobarbital Mechanism & Management
Background - The Two Types Compared
| Feature | Type I (Crigler-Najjar) | Type II (Arias Syndrome) |
|---|---|---|
| UGT1A1 activity | Completely absent (0%) | Partially reduced (<10% of normal) |
| Gene | UGT1A1 (mutations in exons 2-5, truncating) | UGT1A1 (missense mutations - residual enzyme) |
| Inheritance | Autosomal recessive | Autosomal recessive (dominant in some families) |
| Serum bilirubin | Usually >20 mg/dL (range 17-50), all unconjugated | Usually <20 mg/dL (range 6-45), almost all unconjugated |
| Phenobarbital response | No response | Dramatic reduction in bilirubin |
| Kernicterus risk | Very high - most die in infancy untreated | Little to no risk |
| Treatment | Phototherapy 12-16 hrs/day → liver transplant | Phenobarbital |
| Prognosis | Death in infancy if untreated | Usually normal lifespan |
Why Does Phenobarbital Work in Type II?
The Key Difference
Mechanism of Phenobarbital
- Binds to the promoter region of UGT1A1 upon activation by phenobarbital
- Upregulates transcription of the UGT1A1 gene
- Increases the amount of UGT1A1 enzyme protein in hepatocytes
- The larger pool of (albeit less-efficient) enzyme conjugates more bilirubin
- Conjugated bilirubin (water-soluble) is then excreted into bile normally
Clinical Use of Phenobarbital in Type II
| Aspect | Details |
|---|---|
| Dose | ~60-180 mg/day in adults; weight-based in children (~5 mg/kg/day) |
| Response time | Bilirubin begins falling within 1-2 weeks of starting treatment |
| Degree of response | ~25-50% reduction in total serum bilirubin |
| Diagnostic use | A positive response to phenobarbital helps distinguish Type II from Type I |
| Duration | Long-term / lifelong maintenance |
| Monitoring | LFTs, bilirubin levels, signs of drug toxicity (sedation, ataxia) |
Phenobarbital as a Diagnostic Tool
- No response → strongly suggests Type I → plan for liver transplantation
- Clear bilirubin reduction → confirms Type II → continue phenobarbital long-term
Additional Management in Type II
- Phototherapy - may be needed during acute bilirubin rises (intercurrent illness, fasting, surgery)
- Avoid triggers that worsen hyperbilirubinemia: fasting, dehydration, certain drugs (rifampicin, cyclosporine, valproate which compete with or inhibit UGT)
- Liver transplant - not usually needed in Type II but reserved for severe refractory cases
- Gene therapy - under investigation for both Type I and II (AAV-mediated UGT1A1 delivery)
Key Point Summary
Phenobarbital works in Crigler-Najjar Type II because the enzyme is reduced, not absent. By inducing UGT1A1 gene transcription via the CAR nuclear receptor, phenobarbital amplifies the residual enzyme pool enough to significantly lower bilirubin and prevent kernicterus - allowing these patients to live a normal lifespan, which sharply contrasts with the fatal outcome of untreated Type I.
What other enzyme inducers besides phenobarbital work in Type II?
Crigler-Najjar type II enzyme inducers besides phenobarbital UGT1A1 clofibrate rifampicin treatment
https://pmc.ncbi.nlm.nih.gov/articles/PMC8411811
https://www.mdpi.com/1422-0067/25/20/11006
Crigler-Najjar type II UGT1A1 inducer treatment alternative phenobarbital
Crigler-Najjar type II clofibrate fluphenazine rifampicin UGT1A1 inducers bilirubin reduction
Other Enzyme Inducers That Work in Crigler-Najjar Type II
Documented UGT1A1 Inducers in Type II
| Drug | Receptor/Mechanism | Evidence | Notes |
|---|---|---|---|
| Phenobarbital | CAR (constitutive androstane receptor) | Strong - gold standard | Reduces bilirubin 25-70%; first-line |
| Clofibrate | PPARα (peroxisome proliferator-activated receptor α) | Case reports | Fibrate lipid-lowering drug; induces UGT1A1 via PPARα pathway; used historically |
| Rifampicin (low dose) | PXR (pregnane X receptor) | Limited case reports | A potent inducer of CYP3A4 and some UGTs; paradoxically, high-dose rifampicin can inhibit UGT-mediated conjugation and worsen bilirubin - so dose matters critically |
| Fluphenazine | Uncertain | Older case reports | Antipsychotic phenothiazine; reported to reduce bilirubin in some CNS Type II patients; rarely used today |
| Other barbiturates (e.g., primidone, butabarbital) | CAR | Limited data | Share mechanism with phenobarbital; not preferred over phenobarbital |
Why These Work - Receptor Pathways
Phenobarbital → CAR activation → UGT1A1 gene transcription ↑
Clofibrate → PPARα activation → UGT1A1 gene transcription ↑
Rifampicin → PXR activation → UGT1A1 gene transcription ↑
↓
More UGT1A1 enzyme
↓
More bilirubin conjugated → excreted
↓
Serum bilirubin falls
Important Caveat - HNF-1α Promoter Mutations
- The promoter cannot be activated by CAR, PXR, or PPARα ligands
- Neither phenobarbital nor any other inducer works
- This is why genetic testing is important - if an HNF-1α site mutation is found, inducers should not be used and alternative management is required
Broader Pharmacological Treatments in Type II
| Agent | Mechanism |
|---|---|
| Calcium phosphate / orlistat | Bind bilirubin in the gut, reduce enterohepatic recirculation |
| Ursodeoxycholic acid (UDCA) | Choleretic - promotes bile flow and bilirubin excretion |
| Tin-mesoporphyrin / Zinc-protoporphyrin | Heme-oxygenase inhibitors - reduce bilirubin production at the source |
| Phototherapy | Used as backup during illness-related bilirubin spikes |
Practical Bottom Line
Treatment for the acinetobacter baumanni
Acinetobacter baumannii treatment guidelines 2024 carbapenem resistant colistin sulbactam cefiderocol
Treatment of Acinetobacter baumannii Infections
Key Principles
- Treatment difficulty stems from: distinguishing colonization vs true infection, and extensive multidrug resistance
- Empirical therapy should be based on local epidemiology and patient's known colonization status
- Definitive therapy must be guided by antimicrobial susceptibility testing (AST)
- Always obtain Infectious Diseases consultation - proven to reduce mortality
Step 1 - Classify by Resistance Profile
| Category | Definition | Empirical Approach |
|---|---|---|
| Susceptible | Sensitive to most antibiotics | β-lactams (ampicillin-sulbactam preferred) |
| MDR | Resistant to ≥3 antibiotic classes | Carbapenems or high-dose sulbactam combinations |
| CRAB (Carbapenem-resistant) | Resistant to all carbapenems | Sulbactam-durlobactam (preferred) or polymyxin-based combos |
| XDR/PDR | Resistant to almost all/all options | Salvage combinations; ID consult mandatory |
Treatment by Susceptibility
A. Carbapenem-Susceptible Strains
| Drug | Dose | Notes |
|---|---|---|
| Ampicillin-sulbactam (preferred) | 3 g q4h (extended infusion) | Sulbactam has direct antibacterial activity against A. baumannii via PBP2/PBP3 inhibition |
| Meropenem | 2 g q8h over 3h infusion | For susceptible isolates only |
| Imipenem-cilastatin | 500 mg q6h over 3h infusion | For susceptible isolates only |
| Cefepime | 2 g q8h | If susceptible on AST |
B. Carbapenem-Resistant A. baumannii (CRAB) - 2024 IDSA Preferred Regimen
First-Line (Preferred):
| Drug | Dose | Notes |
|---|---|---|
| Sulbactam-durlobactam | 1 g/1 g q6h over 3h | FDA-approved 2023; Durlobactam protects sulbactam from Acinetobacter-derived cephalosporinases (ADC) and OXA-type carbapenemases |
| + Imipenem-cilastatin | 500 mg q6h | Added to the combination for synergy |
Clinical evidence: RCT (n=125 CRAB patients) showed 19% 28-day mortality with sulbactam-durlobactam vs 32% with colistin - lower nephrotoxicity too. - Harrison's 22E, p.1340
Alternative (When sulbactam-durlobactam unavailable):
| Partner Drug | Dose | Preferred For |
|---|---|---|
| Polymyxin B | Per international consensus (Tsuji et al.) | Bloodstream infections (preferred over colistin) |
| Colistin (Polymyxin E) | Per international consensus | Urinary tract infections (preferred) |
| Tigecycline | 200 mg loading → 100 mg q12h | Combination only; high-dose needed; low serum levels |
| Minocycline | 200 mg q12h IV/PO | Good tissue penetration; combination therapy |
| Cefiderocol | 2 g q8h over 3h | Use only in combination; conflicting mortality data (see below) |
High-dose sulbactam rationale: increases binding to PBP2 and PBP3 targets to optimise cell wall synthesis inhibition.
C. Novel Agent: Cefiderocol
| Feature | Detail |
|---|---|
| Class | Siderophore cephalosporin - hijacks bacterial iron-uptake pathways to enter the cell |
| Activity | Active against CRAB, CRPA, ESBL, KPC, OXA-48, MBL (broadest novel β-lactam coverage) |
| Caution | In one RCT of critically ill CRAB patients: 50% mortality in cefiderocol arm vs 18% in best available therapy - use only as part of combination, not monotherapy |
| IDSA guidance | Reserve for treatment failure or when other options exhausted; use in combination only |
Drug Activity Summary vs Resistant Organisms
| Antibiotic | ESBL | KPC | OXA-48 | MBL | CRPA | CRAB |
|---|---|---|---|---|---|---|
| Imipenem/relebactam | ✓ | ✓ | - | - | ✓ | - |
| Ceftolozane/tazobactam | ✓ | - | - | - | ✓ | - |
| Ceftazidime/avibactam | ✓ | ✓ | ✓ | - | ✓ | - |
| Meropenem/vaborbactam | ✓ | ✓ | - | - | - | - |
| Cefiderocol | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Sulbactam-durlobactam | - | - | ✓ | - | - | ✓ |
Special Site Considerations
| Infection Site | Key Points |
|---|---|
| Pneumonia (VAP/HAP) | Most common site; polymyxins achieve poor lung concentrations - consider inhaled colistin as adjunct |
| Bloodstream infections | Polymyxin B preferred over colistin (better PK/PD); remove central line if catheter-related |
| CNS/Meningitis | Requires drugs with adequate CSF penetration; colistin intrathecal/intraventricular may be needed |
| UTI | Colistin preferred over polymyxin B; catheter removal essential |
| Wound/burn | Remove infected devitalized tissue; systemic + topical therapy |
Resistance Mechanisms (Why This Bug Is So Hard to Treat)
- OXA-type carbapenemases (OXA-23, OXA-40, OXA-58) - most common CRAB mechanism
- ADC (Acinetobacter-derived cephalosporinase) - intrinsic AmpC β-lactamase
- ESBL production
- Efflux pumps (AdeABC, AdeFGH)
- Porin loss (OmpA downregulation)
- Biofilm formation on devices
Quick Reference - IDSA 2024 Algorithm
A. baumannii infection confirmed
↓
Susceptibility testing
↓
Carbapenem-susceptible? → YES → Ampicillin-sulbactam ± carbapenem
↓ NO
CRAB
↓
Sulbactam-durlobactam available? → YES → Sulbactam-durlobactam + imipenem
↓ NO
High-dose Amp-Sulbactam + (Polymyxin B or Tigecycline or Minocycline or Cefiderocol)
↓
Reassess 48-72h; adjust per cultures + clinical response