Are T-inversions benign also?
Reading File
Finding Sources
Searching PubMed
T wave inversion ECG clinical significance
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
No - T-wave inversions are not always benign. Their significance depends entirely on the lead location, morphology, depth, clinical context, and associated symptoms. Here is a structured breakdown:
T-Wave Inversions: Benign vs. Pathological
When T-Wave Inversions ARE Normal (Benign)
| Situation | Detail |
|---|---|
| Lead aVR | T inversion is normal in aVR in virtually everyone |
| Lead V1 | Isolated T inversion in V1 is normal |
| Lead III | T inversion in lead III alone is usually a normal variant |
| Neonates/infants | Flat or inverted T waves in right precordial leads (V1-V3) are normal in the first years of life and may persist into adolescence |
| Children | T-wave changes are common in infants and children and rarely reflect ischemia |
As Tintinalli's Emergency Medicine notes: "T-wave inversion in the right pre-cordial leads is common in the first years of life and may persist into adolescence or revert in early childhood to the typical upright pattern seen in adults. T-wave changes are common in infants and children and rarely reflect ischemia."
When T-Wave Inversions Are PATHOLOGICAL
1. Acute Coronary Syndrome (UA/NSTEMI)
T-wave inversion ≥0.1 mV in 2 contiguous leads with a prominent R wave or R/S ratio >1 is a diagnostic criterion for UA/NSTEMI. This is one of the most common and important pathological causes.
2. Wellens' Syndrome (Critical LAD Stenosis)
This is one of the most dangerous patterns - deep, symmetric T-wave inversions in V2-V3 (75% of cases) or biphasic T waves (25%) occurring when a patient is pain-free after an anginal episode. The criteria include:
- History of episodic chest pain consistent with unstable angina
- During pain, ECG may not display abnormal T waves
- When pain-free: deep symmetric T-wave inversion most prominent in V2 and V3, often in V1 and V3, occasionally V3-V6
- No pathologic Q waves or loss of R waves
- Normal or minimally elevated cardiac biomarkers
This pattern indicates critical proximal LAD stenosis and is a pre-infarction warning - the patient is at high risk of massive anterior STEMI if not treated urgently.
3. Pulmonary Embolism
T-wave inversion in V1 through V4 is a classic ECG sign of acute pulmonary hypertension from PE. It is part of the PE ECG severity scoring system - T inversion in V1-V4 scores 4 points and isolated V1 inversion >2 mm scores 2 points (Tintinalli's Emergency Medicine, PE chapter).
4. Right Ventricular Strain
Cor pulmonale, pulmonary hypertension, or acute RV overload can produce T inversions across the right precordial leads.
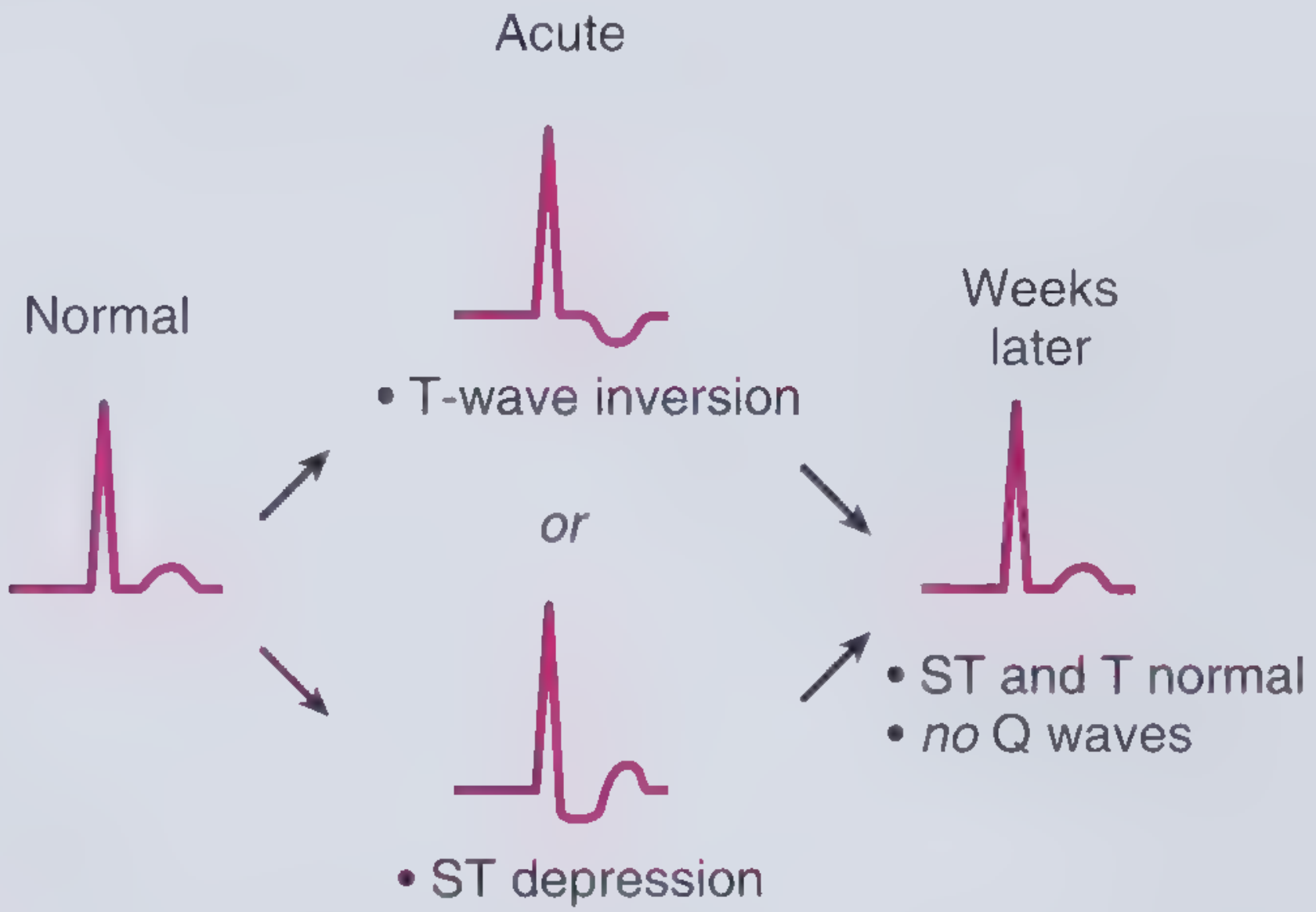
5. Post-STEMI
After ST-elevation resolves following reperfusion, T-wave inversions (sometimes deep and symmetric, similar to Wellens') may follow. These can become permanent in some patients.
6. Structural / Other Causes
- Hypertrophic cardiomyopathy - often dramatic T inversions in lateral leads
- Left bundle branch block and ventricular paced rhythms - discordant T inversions (expected, but mask ischemia assessment)
- Takotsubo (stress) cardiomyopathy - can mimic STEMI/Wellens'
- Hypokalemia - T wave flattening or inversion with prominent U waves
- Digoxin effect - scooped ST/T changes
- Subarachnoid hemorrhage - "cerebral T waves," deeply inverted, widespread, in the context of neurological presentation
Key Clinical Rule
The same morphology means very different things depending on:
-
Which leads: V1 alone = benign; V1-V4 in a dyspneic patient = think PE; V2-V3 deep symmetric in chest pain = Wellens'
-
Symptoms: Asymptomatic isolated findings vs. chest pain/dyspnea dramatically changes the significance
-
Depth and symmetry: Deep, symmetric inversions are more concerning than flat, asymmetric ones
-
Acuity: New inversions on a serial ECG are never benign until proven otherwise
-
Frameworks for Internal Medicine, ACS chapter
-
Tintinalli's Emergency Medicine, Chapters 49 (ACS) and 56 (PE)
Can panic attacks produce T inversions
Finding Sources
Searching PubMed
panic attack T wave inversion ECG changes
Finding Sources
Finding Sources
Finding Sources
Searching the Web
panic attack T wave inversion ECG changes mechanism
Reading File
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC4325305
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
This gives a thorough picture. Here is the complete answer:
Can Panic Attacks Produce T-Wave Inversions?
Yes, they can - through several mechanisms, ranging from transient nonspecific changes to a more serious stress-induced syndrome that genuinely mimics ACS.
Mechanism 1: Nonspecific T-Wave Changes from Sympathetic Surge
During a panic attack, there is a marked surge in noradrenergic discharge from the locus coeruleus and elevated circulating catecholamines. This autonomic activation can produce nonspecific ST-segment and T-wave changes, including T-wave flattening or mild inversions. These are generally transient, reversible, and not associated with structural cardiac disease.
Key point from the web literature: anxiety-related T-wave changes tend to be less pronounced than depression-associated inversions, and there is limited evidence that anxiety alone meaningfully changes T-wave amplitude or QTc. Most changes are non-specific and rate-related (tachycardia alters repolarization).
Mechanism 2: Hyperventilation
Panic attacks almost always involve hyperventilation. Hypocapnia from hyperventilation causes:
- Coronary vasospasm
- Alkalosis-driven shifts in electrolytes (particularly calcium and potassium)
- Altered myocardial repolarization
These can produce ST-segment depression and T-wave changes on ECG that mimic ischemia and resolve when breathing normalizes.
Mechanism 3: Takotsubo (Stress) Cardiomyopathy - The Important One
This is the most clinically significant pathway. Takotsubo syndrome (TS) - also called stress cardiomyopathy or "broken heart syndrome" - is triggered by intense emotional or physical stress through a catecholamine storm mechanism. Key facts from Rosen's Emergency Medicine:
- Serum catecholamines in TS are more than twice as high as in myocardial infarction
- Anxiety is explicitly listed as a risk factor for TS
- Emotional stress is one of the recognized triggers
- ECG shows ST-segment elevations or deep T-wave inversions - indistinguishable from ACS
- Serum troponin is mildly elevated
- BNP is elevated in up to 80% of patients
- 85% of US cases occur in women over age 60
- In the ED, TS is usually not distinguishable from AMI and must be treated accordingly
So a severe panic attack in a susceptible individual (older woman, anxiety history, cardiovascular risk factors) can trigger genuine Takotsubo syndrome with real, deep T-wave inversions, not just artifact.
The Clinical Problem: Panic Disorder Mimics ACS (and vice versa)
Harrison's 22nd edition notes a striking statistic: panic disorder was the primary diagnosis in 43% of patients with chest pain who had normal coronary angiograms, and was present in 9% of all outpatients referred for cardiac evaluation. This cuts both ways:
- Panic attacks produce chest pain, palpitations, dyspnea - identical to ACS symptoms
- They can produce ECG changes including T-wave inversions
- But ACS can also present with anxiety and panic-like symptoms
This means you cannot diagnose a panic attack based on T-wave inversions alone - cardiac causes must be ruled out first, especially in first presentations.
Bottom Line
| Mechanism | T Inversions? | Severity |
|---|---|---|
| Sympathetic/catecholamine surge | Mild, nonspecific | Benign, transient |
| Hyperventilation/hypocapnia | Mild ST-T changes | Benign, reversible |
| Takotsubo syndrome triggered by panic | Deep, significant | Serious - mimics STEMI |
The safest approach: treat T-wave inversions in a patient presenting with chest pain and panic-like symptoms as cardiac until proven otherwise, get serial ECGs and troponins, and consider Takotsubo in the differential - particularly in older women after severe emotional stress.
- Rosen's Emergency Medicine, Takotsubo Syndrome chapter
- Harrison's Principles of Internal Medicine 22E, Panic Disorder chapter
- PMC review: Cardiac and non-cardiac causes of T-wave inversion
This is a shared conversation. Sign in to Orris to start your own chat.