I'm a second year mbbs student. Explain me the topic of ANEURYSM AND DISSECTION including: 1. Pathogenesis 2. Microscopic features 3. Clinical features The explanation should include the following conditions: 1. Aneurysm(types, Pathogenesis, Microscopic, Clinical features) 2. Abdominal aorta dissection 3. Thoracic aorta dissection 4. Article dissection The explanation should be based on ROBBINS AND COTRANS PATHOGENESIS OF DISEASES MBBS 2ND YEAR
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content I need from Robbins and Cotran. Let me compile the comprehensive response for the student.
Aneurysm and Dissection
Based on Robbins & Kumar Basic Pathology and Robbins, Cotran & Kumar Pathologic Basis of Disease
Overview and Definitions
An aneurysm is a localized abnormal dilation of a blood vessel or the heart - it may be congenital or acquired.
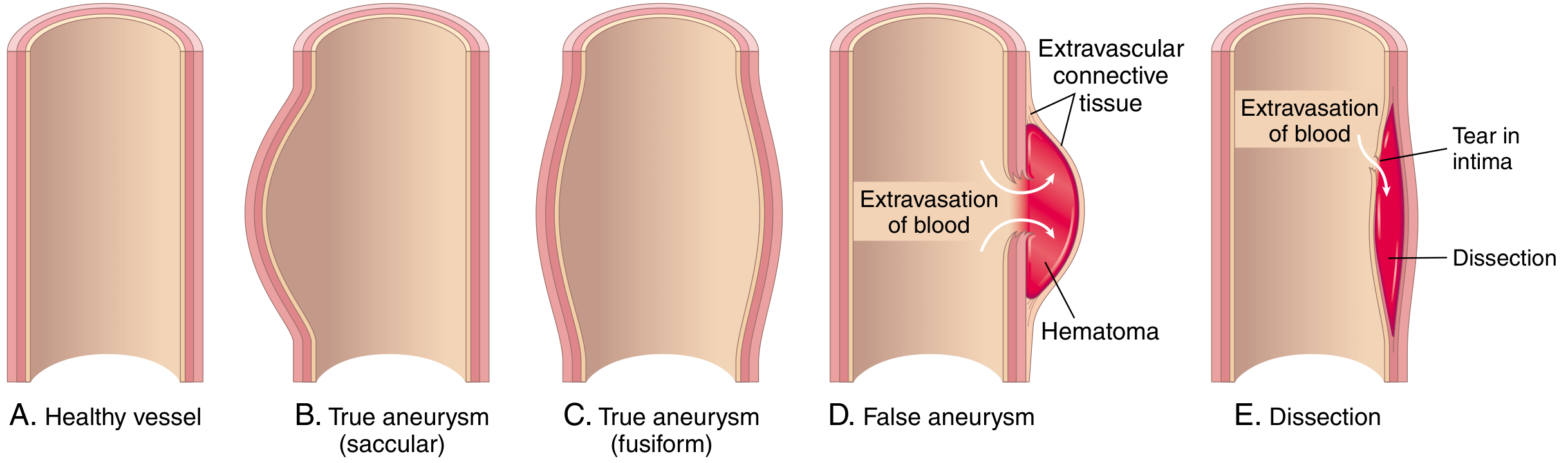
TYPES OF ANEURYSMS
1. True Aneurysm
The aneurysm involves all three layers of the intact (but attenuated) arterial wall - intima, media, and adventitia. The wall bulges outward but remains intact. Examples include:
- Atherosclerotic aneurysms
- Congenital vascular aneurysms
- Ventricular aneurysms following transmural MI
2. False Aneurysm (Pseudoaneurysm)
A defect in the vascular wall leads to an extravascular hematoma that freely communicates with the intravascular space - also called a "pulsating hematoma." The wall itself is ruptured. Examples:
- Ventricular rupture after MI contained by a pericardial adhesion
- Leak at a vascular graft-artery anastomosis
3. By Morphological Shape
| Type | Description | Size in Aorta |
|---|---|---|
| Saccular | Spherical outpouching involving only a portion of the vessel wall | 5-10 cm diameter, often contains thrombus |
| Fusiform | Diffuse, circumferential dilation of a long vascular segment | 5-10 cm diameter; can involve aortic arch, abdominal aorta, iliacs |
PATHOGENESIS OF ANEURYSMS
Core concept: Aneurysms occur when the structural or functional integrity of connective tissue within the vascular wall is compromised. The arterial wall normally undergoes constant remodeling - synthesizing, degrading, and repairing ECM. When this balance is disrupted, the wall weakens and dilates.
The Two Most Important Causes:
- Atherosclerosis - greater factor in abdominal aortic aneurysms (AAA)
- Hypertension - most common etiology in ascending aortic aneurysms
Specific Mechanisms of Wall Weakening:
1. MMP-mediated ECM degradation (Inflammation)
Inflammatory cells (macrophages) associated with atherosclerosis or aortitis produce increased Matrix Metalloproteinases (MMPs) - especially elastolytic MMPs driven by Th2 cytokines (IL-4, IL-13). These degrade elastin, collagens, proteoglycans, laminin, and fibronectin throughout all layers. Simultaneously, decreased expression of TIMPs (tissue inhibitors of metalloproteinases) amplifies ECM breakdown. Result: loss of elastic fibers needed for diastolic recoil.
2. Defective Collagen Synthesis - Genetic Disorders
- Ehlers-Danlos syndrome (vascular type): Defective type III collagen synthesis creates inherently weak vessel walls.
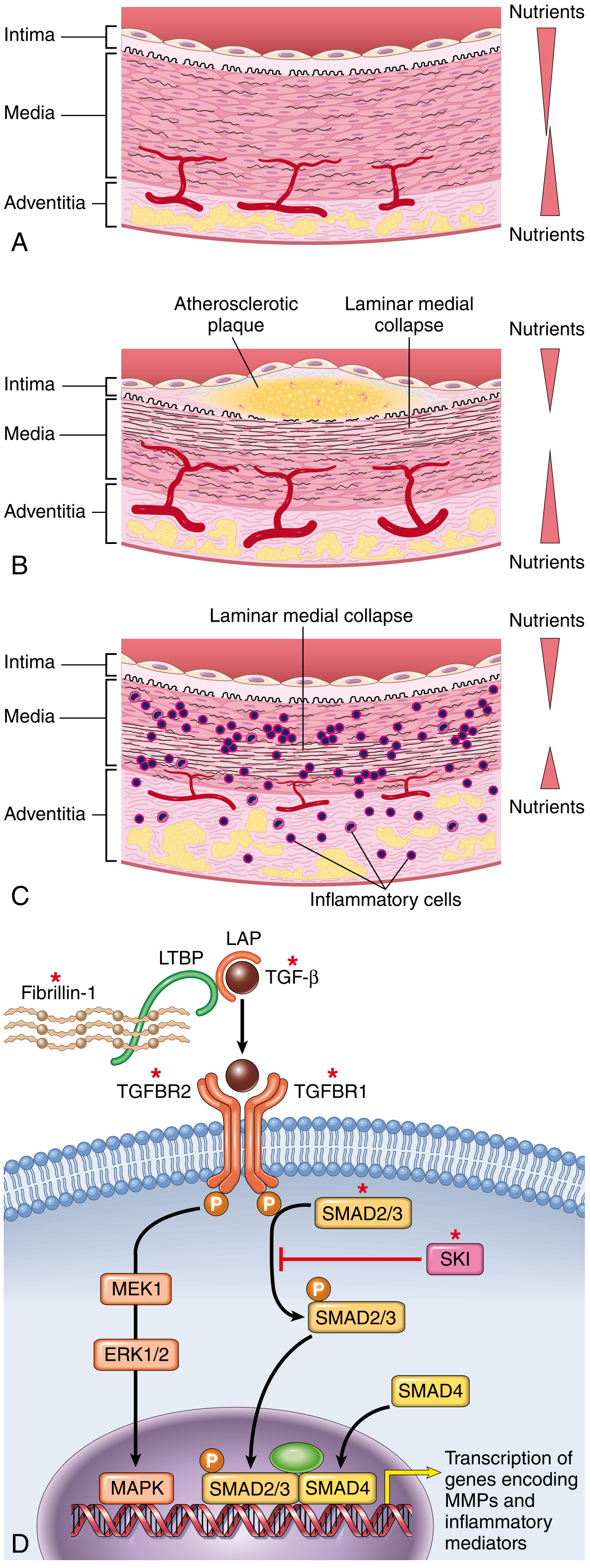
3. Abnormal TGF-β Signaling
- Marfan Syndrome: Mutation in fibrillin-1 gene. Fibrillin-1 normally sequesters TGF-β bound to ECM. Without fibrillin, TGF-β is released excessively, driving MMP transcription and disrupting ECM. Primarily affects the ascending aorta.
- Loeys-Dietz Syndrome: Mutations in TGF-β receptors (TGFBR1/2), SMAD3, or TGF-β3 itself cause overactive TGF-β signaling. Aneurysms can rupture at small sizes.
4. Ischemia of the Inner Media
- Atherosclerotic thickening of the intima increases the diffusion distance for O₂ and nutrients to reach medial SMCs → inner medial ischemia → SMC loss.
- Hypertension narrows arterioles of the vasa vasorum → outer medial ischemia.
- Syphilis (tertiary): Obliterative endarteritis of vasa vasorum of the thoracic aorta → medial ischemia → SMC loss, elastic fiber loss → inadequate ECM synthesis.
5. Mycotic Aneurysms (Infection)
Caused by: (1) septic emboli from infective endocarditis; (2) extension from adjacent suppurative infection; (3) direct hematogenous seeding of the arterial wall.
Final Common Pathway: All these processes lead to histologic changes called medial degeneration - a nonspecific finding common to all forms of aortic disease.
MICROSCOPIC FEATURES (Medial Degeneration)
The histologic hallmark is cystic medial degeneration (CMD) / medial degeneration, which includes:
- Loss and fragmentation of elastic fibers in the tunica media
- Loss of smooth muscle cells (SMCs) - laminar medial collapse
- Accumulation of proteoglycans/mucoid material in the spaces vacated by SMCs and elastic tissue (gives a "cystic" appearance)
- Fibrosis of the media
- In atherosclerotic AAA: severe complicated atherosclerotic changes with destruction and thinning of the underlying aortic media
- In inflammatory AAA: adventitial and periaortic lymphoplasmacytic infiltrate (may suggest IgG4-related disease)
- Mural thrombus formation in the lumen of the aneurysm
1. ABDOMINAL AORTIC ANEURYSM (AAA)
Pathogenesis
- Atherosclerosis is the primary cause - destroys and thins the underlying aortic media
- Smoking is a major independent risk factor
- Other contributors: aging, male sex, genetic predisposition (MMP/TIMP polymorphisms), inflammatory mediators (Th2 cytokines shifting macrophages toward elastolytic MMP production)
- Rarely develops before age 50; occurs more frequently in males and smokers
Microscopic Features (Morphology)
- Located between the renal arteries and the aortic bifurcation
- Severe complicated atherosclerosis with destruction and thinning of the underlying aortic media
- Frequently contains bland, poorly organized mural thrombus
- Size: >3 cm, often >5.5 cm in diameter; up to 25 cm in length
- Can be saccular or fusiform
Clinical Features
- Most AAAs are asymptomatic for years - discovered incidentally on imaging
- Rupture is the most feared complication - presents as sudden-onset severe abdominal/back pain with hypotension (surgical emergency with high mortality)
- Pulsatile abdominal mass - palpable in thin patients
- Compression of adjacent structures can cause ureteral obstruction, venous compression
- Atheroembolism - thrombus/atherosclerotic debris can embolize to distal vessels (legs)
- Thrombosis of the aneurysm with occlusion
- Risk of rupture correlates with size: >5.5 cm warrants surgical repair
2. THORACIC AORTIC ANEURYSM (TAA)
Pathogenesis
- Hypertension is the most common cause of ascending aortic aneurysms
- Marfan syndrome / Loeys-Dietz syndrome - TGF-β signaling dysregulation (see above)
- Tertiary syphilis - classically causes ascending thoracic aneurysms via obliterative endarteritis of the vasa vasorum
- Aortitis (e.g., giant cell arteritis, Takayasu arteritis)
- The ascending thoracic aorta is particularly vulnerable to medial degeneration because it bears the highest pulsatile hemodynamic stress
Microscopic Features
- Same underlying medial degeneration:
- Loss of elastic laminae
- SMC drop-out / laminar medial collapse
- Mucoid/proteoglycan accumulation in the media
- In syphilitic aortitis: obliterative endarteritis of vasa vasorum → adventitial/medial lymphoplasmacytic infiltration → elastic fiber destruction
- In Marfan syndrome: the medial changes are diffuse with the above features
Clinical Features
- Can cause aortic root dilation → aortic valve incompetence/regurgitation (wide pulse pressure, diastolic murmur)
- Compression of mediastinal structures:
- Trachea/bronchi → cough, dyspnea, stridor
- Esophagus → dysphagia
- Recurrent laryngeal nerve → hoarseness
- Superior vena cava → SVC syndrome (facial plethora, arm swelling)
- Chest/back pain - deep, boring pain
- Syphilitic aneurysms typically involve the ascending aorta and arch - can produce a "tree-bark" appearance of the intima (wrinkled, pearly-white)
- Rupture into the pleural space or pericardium
3. AORTIC DISSECTION (Thoracic and Abdominal)
Definition
An arterial dissection arises when blood enters a defect in the arterial wall and tunnels through medial or medial-adventitial planes, creating a false lumen within the wall itself. Dissections mostly (but not always) occur at an aneurysmal site.
Key distinction from pseudoaneurysm: in dissection, blood travels within the wall; in pseudoaneurysm, blood collects outside the wall.
Pathogenesis
The fundamental requirement is a weakened media (medial degeneration). Blood enters through:
- A tear in the intima (most common) allowing blood to track between the media layers
- OR rupture of the vasa vasorum within the media, causing a medial hematoma that then dissects the layers
Predisposing conditions:
- Hypertension (most common systemic risk factor) - present in >90% of cases; causes ischemia of inner media via intimal thickening and ischemia of outer media via vasa vasorum damage
- Marfan syndrome / Loeys-Dietz syndrome - fibrillin/TGF-β pathway defects
- Iatrogenic - cardiac catheterization, intra-aortic balloon pump insertion
- Pregnancy - increased hemodynamic stress (especially in 3rd trimester)
- Bicuspid aortic valve - associated with underlying medial degeneration
- Cocaine use - severe hypertensive surges
Stanford Classification (Clinically important):
| Type | Involvement | Treatment |
|---|---|---|
| Type A | Involves ascending aorta (regardless of origin) | Emergency surgery |
| Type B | Descends from distal to left subclavian artery | Medical management (unless complications) |
DeBakey Classification:
- Type I: Originates in ascending, extends to arch and beyond
- Type II: Confined to ascending aorta
- Type III: Originates in descending thoracic aorta
Microscopic Features
- Medial degeneration is the histological precondition: loss of elastic laminae, SMC dropout, mucoid change
- The dissection plane runs through the outer media or at the media-adventitia junction - this is the plane of cleavage
- Separation of the elastic lamellar units by blood - creating a false lumen
- No true inflammatory reaction in the acute phase
- The false lumen may contain organized thrombus in older dissections
- The intimal tear is typically a transverse laceration (5-6 cm above the aortic valve in Type A)
Clinical Features
Thoracic Aortic Dissection:
- Classic presentation: Sudden onset of severe, tearing or ripping chest pain that radiates to the back/interscapular region - described as the "worst pain of my life"
- Pain may migrate distally as the dissection propagates
- Hypertension is typically present at presentation
- Pulse deficits: unequal blood pressure in arms (>20 mmHg difference); weak or absent pulses in branches of the aorta as they are compromised
- Aortic regurgitation (Type A) - diastolic murmur, wide pulse pressure - due to aortic root involvement
- Neurological signs - stroke, paraplegia (spinal cord ischemia from intercostal/spinal artery compromise)
- Cardiac tamponade - if dissection extends retrograde into the pericardium (Type A) → Beck's triad (hypotension, muffled heart sounds, raised JVP)
- MI - if dissection involves coronary ostia (right coronary more often)
- Chest X-ray findings: widened mediastinum, pleural effusion (hemothorax)
Abdominal Aortic Dissection:
- Less common than thoracic; usually an extension of a Type B dissection
- Abdominal/back pain - severe, tearing character
- Mesenteric ischemia if superior mesenteric artery or celiac trunk orifices are compromised → abdominal pain, bloody diarrhea
- Renal ischemia - if renal arteries are involved → oliguria, acute kidney injury, new-onset hypertension
- Lower limb ischemia - if iliac arteries compromised → pulseless, cold legs
- Without treatment: death from external rupture (hemorrhage into pleural cavity, peritoneum, or mediastinum)
4. ARTERIAL DISSECTION (General Concept)
As described above, the defining feature is:
- Blood entering a defect in the vessel wall
- Tunneling through medial or medial-adventitial planes
- Creating a false lumen alongside the true lumen
The aortic dissection can re-enter the true lumen distally (creating a "double-barreled aorta"), or rupture externally. The outer wall of the false channel is formed by the outer layers of the media + adventitia alone - these are thin and prone to rupture.
Natural history without treatment:
- ~80% mortality within 2 weeks for untreated Type A dissection
- Rupture through the adventitia causes massive hemorrhage
Summary Table
| Feature | AAA | Thoracic Aneurysm | Aortic Dissection |
|---|---|---|---|
| Primary cause | Atherosclerosis | Hypertension / Marfan | Hypertension / Medial degeneration |
| Location | Below renal arteries | Ascending/arch | Any; Type A above, Type B below left subclavian |
| Key microscopy | Atherosclerosis + medial thinning + mural thrombus | Medial degeneration + cystic change | Dissection plane through outer media; no inflammation |
| Classic symptom | Pulsatile abdominal mass / rupture | Compression symptoms / aortic regurgitation | Sudden tearing chest/back pain |
| Deadly complication | Rupture | Rupture | Rupture, tamponade, stroke, MI |
Sources: Robbins & Kumar Basic Pathology (10th Ed.), p. 288-292; Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 458/475-484
This is a shared conversation. Sign in to Orris to start your own chat.