Liss and mipo in Orthopedic plating what are there what's there principle how are they different usage disadvantages complications with appropriate illustrative diagrams and images
Reading File
Finding Sources
Finding Sources
Searching the Web
LISS vs MIPO orthopedic plating principles differences complications
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Reading Web Page
https://ota.org/sites/files/2021-06/General%20A6%20MIPO%20Te…
Loading Image
Loading Image
I now have all the content needed for a comprehensive, well-illustrated answer. Let me compile it.
LISS and MIPO in Orthopedic Plating
Understanding the Relationship First
LISS (Less Invasive Stabilization System) and MIPO (Minimally Invasive Plate Osteosynthesis) are not the same thing, though they are closely related and often confused:
- MIPO is a surgical technique/approach - a philosophy of how you insert and apply a plate
- LISS is a specific implant system - the first widely adopted device designed to be used with MIPO principles
Think of it this way: MIPO is the method; LISS is one tool for executing that method.
PART 1: MIPO - Minimally Invasive Plate Osteosynthesis
Principle
MIPO was developed as a response to the high rates of nonunion (29-38%) and infection (7-20%) seen with traditional open plating, which required wide dissection that damaged the periosteal blood supply and fracture hematoma.
The core philosophy rests on biological fixation rather than anatomic mechanical fixation:
- Preserve the fracture biology - the fracture zone is left undisturbed ("zone of injury untouched")
- Indirect reduction - length, alignment, and rotation are restored without directly visualizing the fracture
- Bridge the fracture - the plate spans the comminuted zone, providing relative stability (not absolute rigidity)
- Submuscular tunnel insertion - the plate is slid under muscles through small proximal and distal incisions only
- Secondary bone healing - the relative-stability construct allows micromotion, promoting callus formation
The key departure from conventional ORIF is: do not strip the soft tissues around the fracture. Do not compress the plate to bone. Do not achieve rigid anatomic reduction of all fragments.
"The principles of fixation with the application of a bridging construct while preserving the fracture biology are similar to those for open plating. MIPO technique allows preservation of the blood supply to the fracture fragments, in turn improving secondary bone healing."
- Rockwood and Green's Fractures in Adults, 10th ed.
How MIPO is Performed (General Steps)
- Two or three small incisions (3-5 cm each) are made proximal and distal to the fracture
- An extraperiosteal submuscular tunnel is created manually along the bone surface
- The plate is slid through the tunnel without exposing the fracture site
- Fracture reduction is achieved indirectly using traction, distractor frames, or external fixators
- Screws are placed percutaneously through stab incisions guided by the targeting arm or fluoroscopy
Where MIPO is Used
| Region | Approach |
|---|---|
| Distal femur | Lateral submuscular via lateral condyle incision |
| Proximal tibia | Anterolateral submuscular tunnel |
| Distal tibia | Anteromedial or anterolateral |
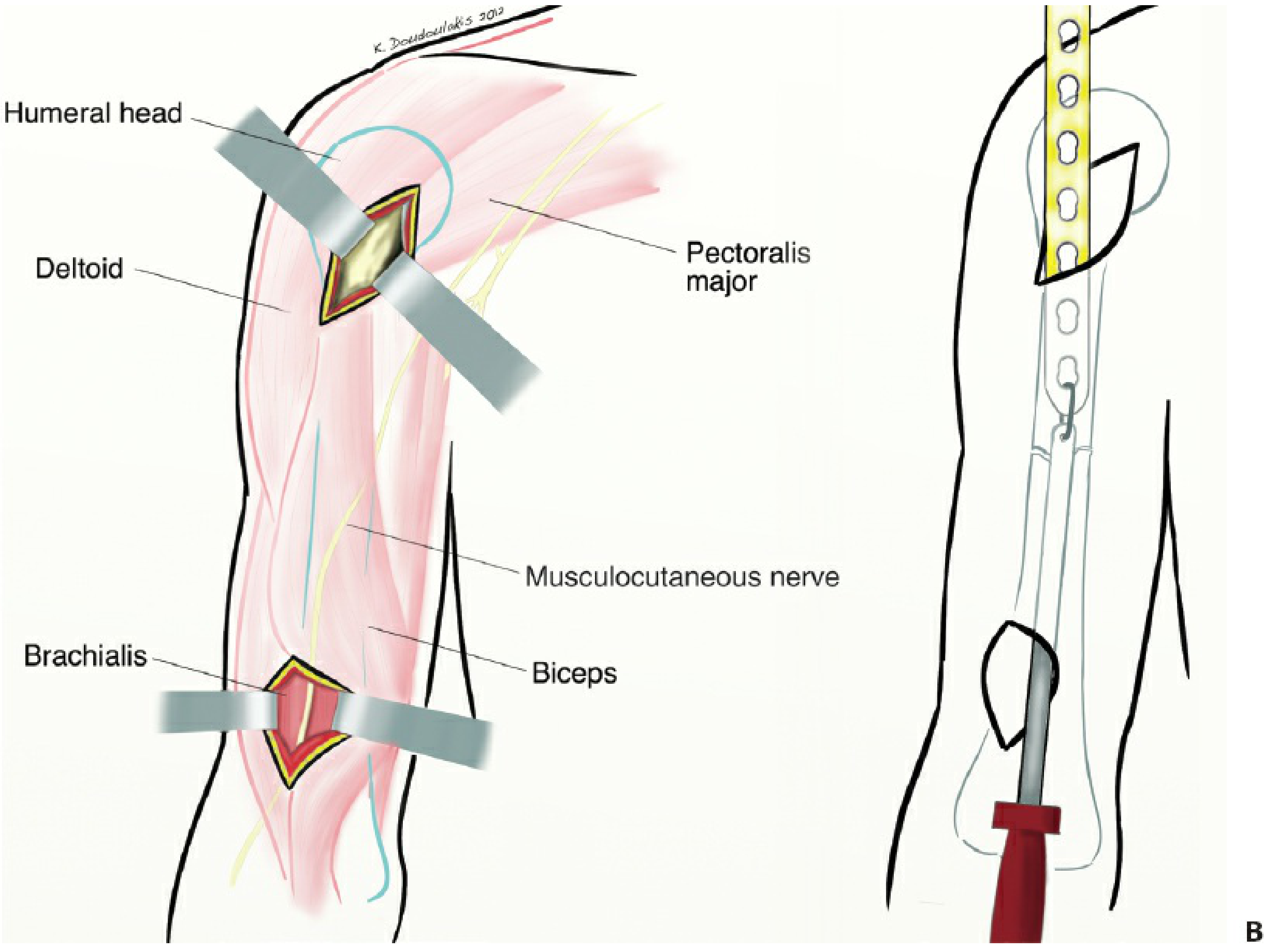
| Humeral shaft | Anterior, lateral, or posterior approaches |
| Femoral shaft | Lateral submuscular |
Advantages of MIPO
- Preserves periosteal vascularity - lower nonunion and infection rates
- Less blood loss intraoperatively
- Smaller incisions - better cosmesis, less wound complications
- Shorter operative time in experienced hands
- Reduced need for bone grafting in comminuted fractures
- Early mobilization possible due to construct stability
PART 2: LISS - Less Invasive Stabilization System
What is LISS?
The LISS plate (originally by Synthes, Paoli, PA; now Johnson & Johnson Medtech) was the first implant system specifically engineered to be used via MIPO technique. It is described in Campbell's Operative Orthopaedics (15th ed, 2026) as:
"An internal-external fixator made of titanium and, therefore, has a different modulus of elasticity than other plating systems."
Distinguishing Design Principles of LISS
-
Fixed-angle locking screws - screw threads engage the plate holes (threaded screw holes), creating a fixed-angle construct. The screw cannot toggle in the plate, so it behaves like an internal fixator - not unlike an external fixator placed under the skin.
-
Unicortical self-drilling, self-tapping locking screws - because the locking mechanism provides angular stability, bicortical purchase is not mandatory (though bicortical is preferred in osteoporotic bone for better pullout resistance).
-
No plate-to-bone compression required - unlike conventional plating where friction between plate and bone provides stability, LISS relies entirely on the locked screw-plate construct. The plate does not need to be contoured exactly to the bone surface and is not pressed against periosteum, preserving blood supply.
-
Radiolucent targeting/insertion arm - the plate is attached to a radiolucent guide arm ("handle") that allows insertion through a submuscular tunnel and guides percutaneous screw placement without direct visualization.
-
Titanium material - lower modulus of elasticity than stainless steel, allowing slight elastic deformation and stress-sharing with bone.
-
Pre-contoured anatomic design - designed specifically for distal femur (femoral LISS) or proximal tibia (tibial LISS), with fixed hole geometry matching the condylar anatomy.
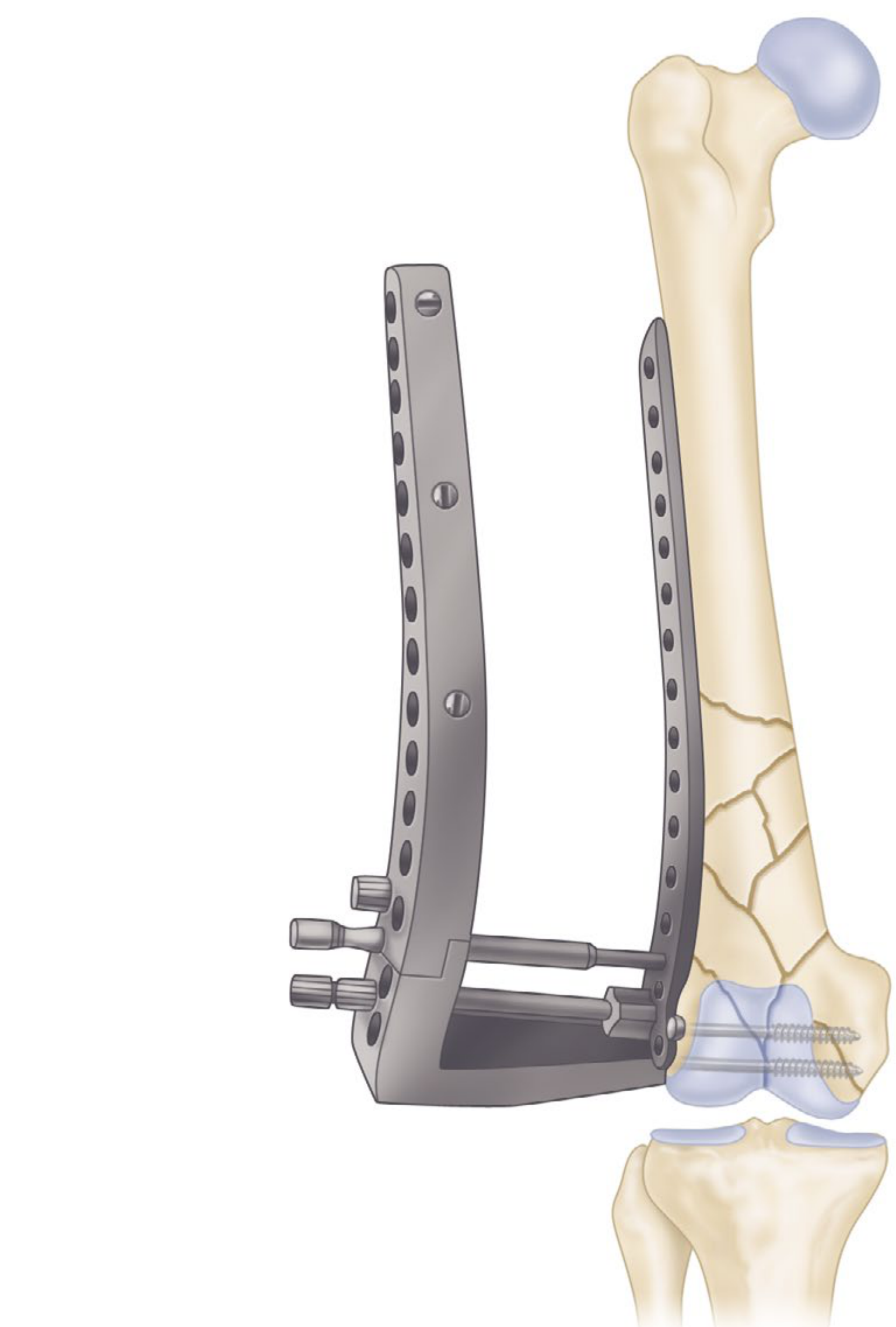
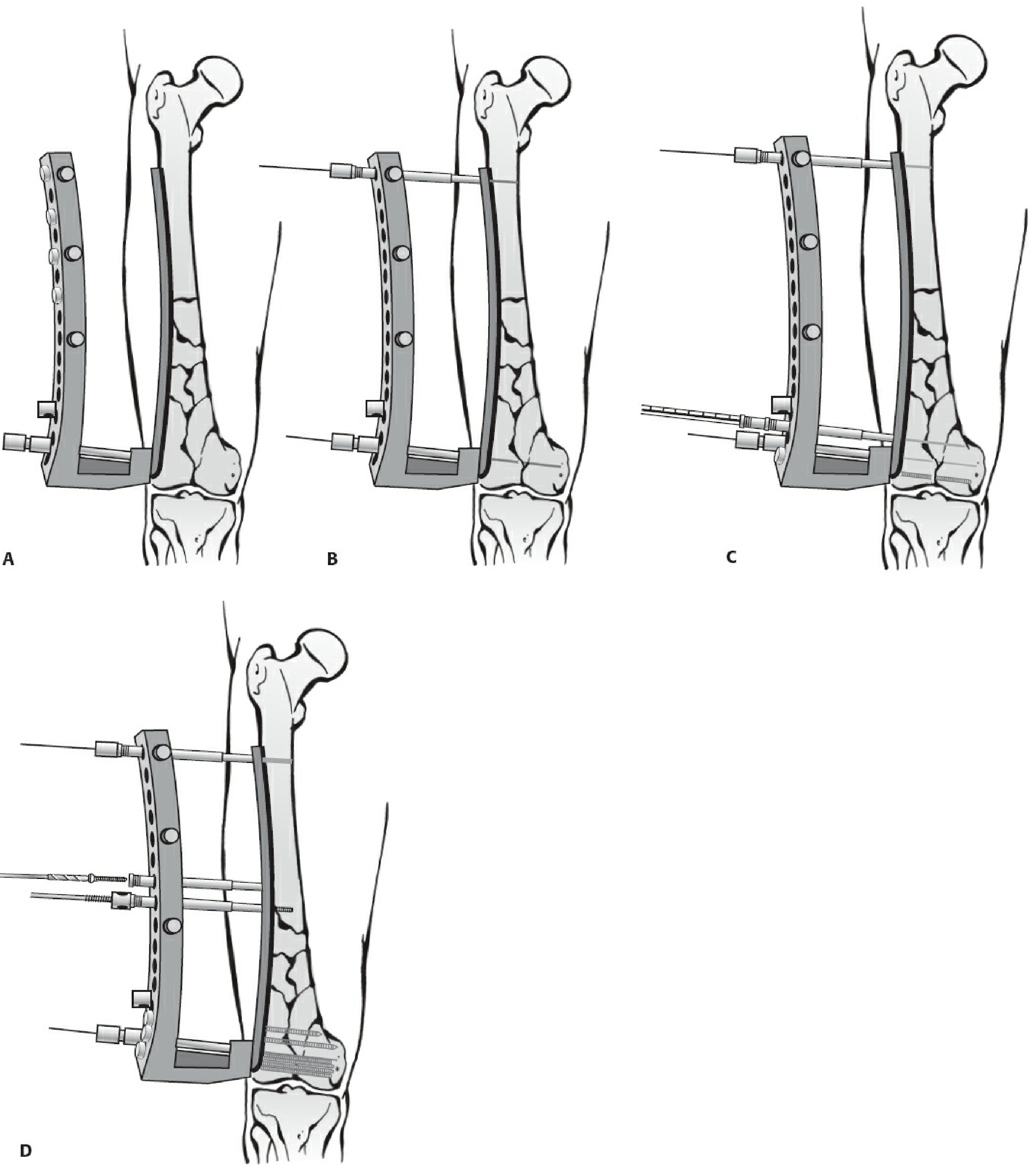
LISS Insertion Technique (Distal Femur Example)
The step-by-step technique is elegantly illustrated by Rockwood and Green's:
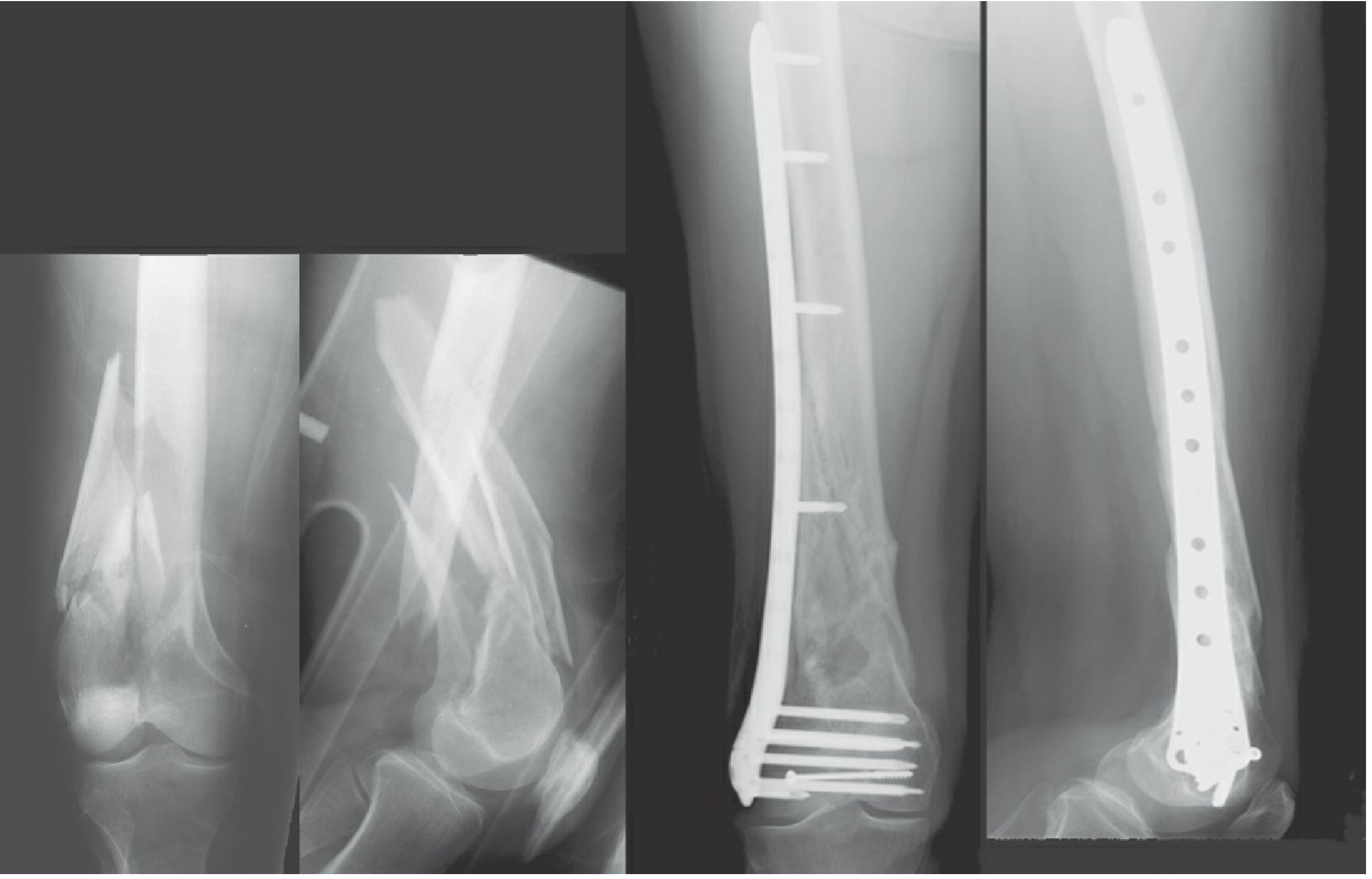
Clinical Application and X-Ray Appearance
PART 3: Key Differences - LISS vs MIPO
| Feature | MIPO | LISS |
|---|---|---|
| Nature | Surgical technique/approach | Specific implant system |
| Scope | Applicable with many plate types | One specific product (distal femur / proximal tibia) |
| Plate type | Any plate used minimally invasively (LCP, LISS, conventional) | Dedicated fixed-angle locking plate only |
| Screw-plate interface | Depends on plate used (locking or non-locking) | Always locked, fixed-angle |
| Targeting | Fluoroscopy-guided or freehand percutaneous | Proprietary radiolucent targeting guide arm |
| Bone contact | Plate may or may not contact bone depending on design | Designed for minimal bone contact |
| Flexibility of use | Any long bone - femur, tibia, humerus, etc. | Anatomically specific (distal femur, proximal tibia) |
| Evolution | Ongoing - all modern minimally invasive plates use MIPO | LISS was first-generation; succeeded by LCP and newer anatomic locking systems |
Conceptual summary: LISS IS a MIPO system, but MIPO does not require LISS. Modern MIPO is most often performed using Locking Compression Plates (LCP), anatomically pre-contoured plates, or variable-angle locking systems - all inserted using MIPO principles. LISS was the pioneering implant that proved the concept.
Evolution of Condylar Fixation Designs

PART 4: Bridge Plating - The Mechanical Foundation
Both LISS and MIPO rely on bridge plating for comminuted fractures:
"Bridge plating is most commonly utilized to span comminuted metaphyseal and diaphyseal fractures. Rather than striving for anatomic reduction and compression of individual fracture fragments, the comminuted region is simply bridged. The resultant construct provides relative rather than absolute stability."
- Rockwood and Green's, 10th ed.
Key mechanical principles:
- Long working length (distance between the most proximal and distal screws) - reduces construct stiffness, allows micromotion, stimulates callus
- Spaced screws - screws clustered near the fracture increase stiffness; spreading them out reduces stiffness appropriately
- Far cortical locking (FCL) screws (newer concept) - near cortex overdrilled so screw engages only far cortex, creating elastic cantilever bending and balanced callus formation
"Rule of toos" for malalignment prevention: The plate must not be applied too distal, too anterior/posterior, or too rotated - any of these will impart deformity to the fracture.
PART 5: Complications
Complications of MIPO Technique
| Complication | Mechanism | Prevention |
|---|---|---|
| Malrotation/malunion | Indirect reduction without direct visualization - rotational assessment is difficult; reported greater malrotation with MIPO vs. ORIF in humeral fractures | Intraoperative fluoroscopy in two planes; rotational assessment using cortical step; clinical limb comparison |
| Nerve injury | Percutaneous screw placement can injure nearby nerves | Radial nerve in humeral lateral approach; Superficial peroneal nerve with LISS tibial screws in holes 11-13 (at 26-30 cm from top) |
| Vascular injury | In distal femur LISS, the superficial femoral artery averages only 21 mm from screw tips (can be as close as 8 mm) in holes 6-10 | Careful screw length selection; awareness of anatomy |
| Iatrogenic fracture | Excessive tunneling force | Careful technique |
| Radiation exposure | Heavy fluoroscopic dependence | Minimize screening time; experienced surgeon |
Complications of LISS Specifically
| Complication | Detail |
|---|---|
| Nonunion | Despite improvement over open plating, LISS nonunion reported at ~4.7%; Henderson et al. found a 20% nonunion rate with modern locked plating technique; stainless steel (vs titanium) identified as risk factor |
| Malunion/malalignment | Overly stiff construct (too many screws clustered near fracture) prevents secondary bone healing; varus collapse particularly noted with distal femur |
| Hardware failure/plate breakage | Excessive stiffness concentrates stress at the plate-fracture interface leading to fatigue failure; nonunion increases hardware stress progressively |
| Implant removal difficulty | Cold welding of self-drilling locking screws into the plate is a recognized specific LISS problem (Suzuki et al., JOT 2010); screws can become impossible to turn |
| Infection | 3% with LISS vs 2.3% with conventional compression plate MIPO vs 6% with open plating (Kolb et al.) - reduced but not eliminated |
| Screw cutout in osteoporotic bone | Unicortical screws have lower pullout strength; bicortical screws recommended in osteoporotic patients |
| Periprosthetic fracture stress risers | The locked unicortical construct creates stress concentration at the ends of the plate |
Risk Factors for Nonunion (LISS/Locking Plate)
- Open fractures (OR 2.42 for nonunion; OR 3.47 for infection)
- Diabetes mellitus
- Obesity
- Stainless steel implant (vs titanium)
- Overly rigid construct (short plate, clustered screws)
- Excessive construct stiffness impairing callus
PART 6: Indications for MIPO/LISS
Ideal fracture patterns:
- Comminuted metaphyseal and diaphyseal fractures (AO A1-A3)
- Complex intra-articular fractures (AO C1-C3) - articular surface reduced openly, metaphysis bridged with MIPO
- Periprosthetic fractures above stable TKA or below well-fixed THA
- Osteoporotic fractures (poor bone quality)
- Open fractures (reduced infection vs conventional open plating)
- Fractures in patients requiring early mobilization
Relative contraindications:
- Simple transverse fractures amenable to compression plating
- Fractures requiring absolute stability (articular step-offs requiring lag screws)
- Severely contaminated open fractures (external fixator preferred first)
Summary: Conceptual Framework
Historical progression:
Open plating (high infection/nonunion)
↓
Biological principles introduced (Mast et al.) - indirect reduction, biology preservation
↓
Fixed-angle implants (blade plate, DCS) - better stability
↓
LISS (1990s) - first "internal external fixator"; combined locking screws + MIPO approach
↓
Modern MIPO with LCP/variable-angle systems - greater flexibility, better anatomic contouring
Core message:
- LISS proved that minimally invasive insertion of a fixed-angle locking plate dramatically reduces infection and nonunion compared to conventional open plating
- MIPO is the umbrella technique now applied with all modern locking plate systems
- The two are inseparable in history but distinct in definition: one is a method, the other was a pioneering device
Sources: Campbell's Operative Orthopaedics 15th ed. 2026 (Chapter 59); Rockwood and Green's Fractures in Adults 10th ed. 2025 (Chapters 12, 37, 58); OTA Core Curriculum MIPO Technique Module.
This is a shared conversation. Sign in to Orris to start your own chat.