properties of smooth muscle
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the material needed for a thorough answer. Here it is:
Properties of Smooth Muscle
1. Structural / Histological Properties
Smooth muscle cells are long, spindle-shaped (fusiform) cells with a single, centrally placed, elongated nucleus. They lack striations because, unlike skeletal and cardiac muscle, the contractile filaments are not organized into sarcomeres - thick (myosin) and thin (actin) filaments are present but arranged obliquely across the cell, not in neat parallel registers. - Costanzo Physiology 7th Edition, p. 48
-
Cell length ranges from ~20 µm (small blood vessels) to ~500 µm (pregnant uterus); diameter at the widest point is 5-10 µm.
-
Adjacent cells are packed in a "tail-to-head" arrangement so that cross-sections show profiles of varying diameter, with only the largest profiles containing nuclei.
-
The cell surface shows numerous small plasmalemmal invaginations called caveolae, which are enriched in ion channels and act as functional substitutes for the T-tubule system of striated muscle.
-
There are no T-tubules; this is unnecessary because the smaller cell diameter allows Ca²⁺ diffusion across the whole cell without them.
-
The sarcoplasmic reticulum (SR) is rudimentary - a peripheral SR close to the sarcolemma handles local Ca²⁺ release for membrane excitability, and a deeper central SR delivers Ca²⁺ to the contractile apparatus.
-
Junqueira's Basic Histology 17e, pp. 527-529
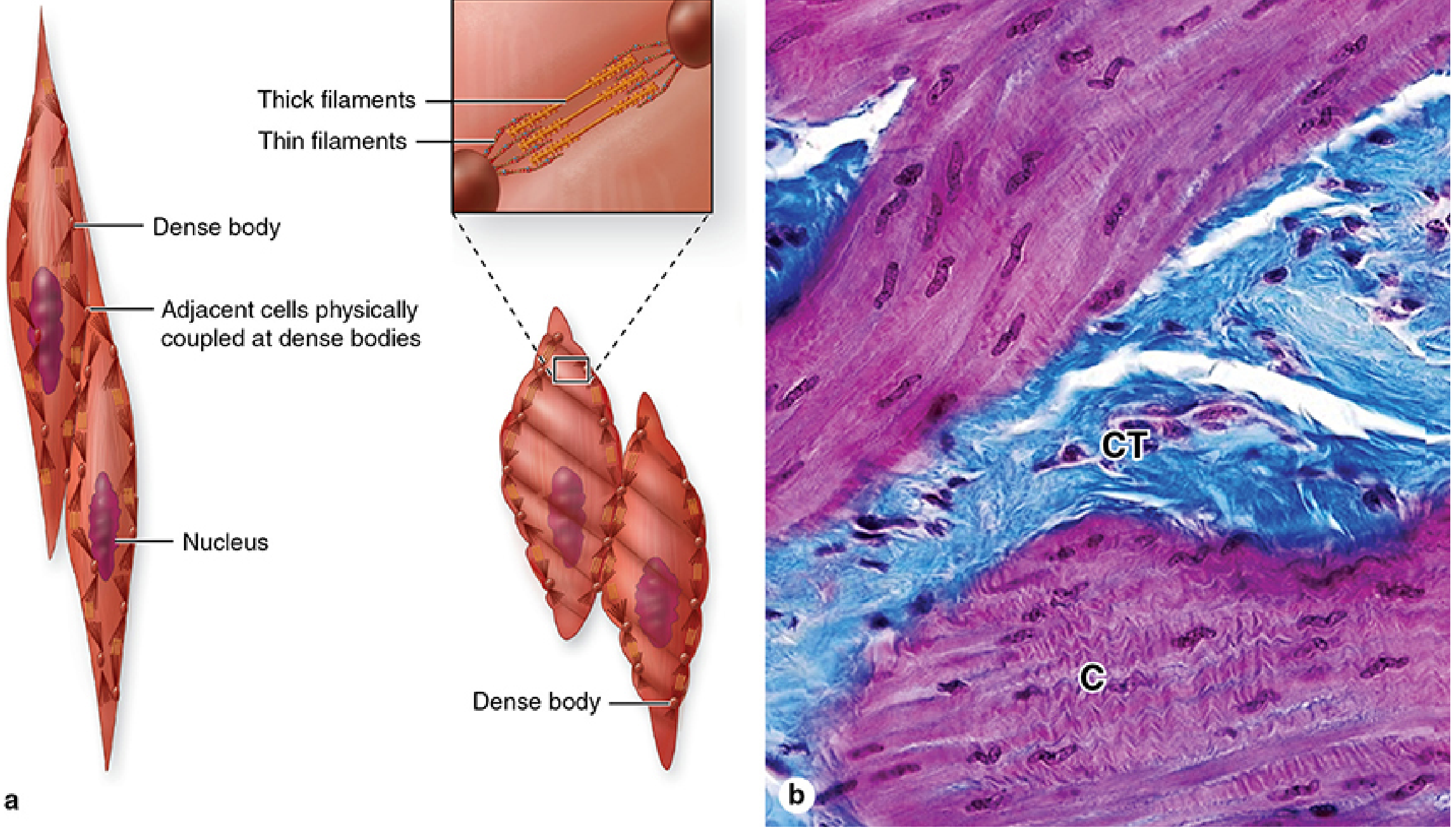
Dense bodies (containing α-actinin) serve as the functional analog of Z-discs: thin actin filaments and intermediate filaments (desmin) insert into them. Dense bodies are also present on the cell membrane and are coupled to adjacent cells via cadherins, so contractile force is transmitted cell-to-cell. During contraction the cells shorten AND twist, giving contracted nuclei a corkscrew appearance. - Junqueira's Basic Histology 17e, p. 529-530
2. Types of Smooth Muscle
| Feature | Unitary (Single-Unit) | Multiunit |
|---|---|---|
| Gap junctions | Abundant | Few/absent |
| Electrical coupling | Yes - cells contract as one unit | No - each cell acts independently |
| Location | GI tract, bladder, uterus, ureter | Iris, ciliary muscle, vas deferens |
| Pacemaker activity | Yes - spontaneous slow waves | No |
| Innervation | Sparse; mainly modulates tone | Dense postganglionic autonomic fibers |
| Response to stretch | Contracts when stretched | Does not |
Costanzo Physiology 7th Edition, p. 48-49
Vascular smooth muscle is a hybrid - it combines features of both types.
3. Excitation-Contraction (E-C) Coupling
The critical difference from skeletal muscle: smooth muscle has no troponin. Contraction is controlled via the Ca²⁺-calmodulin-myosin light chain kinase (MLCK) pathway:
-
A stimulus (depolarization, hormone, neurotransmitter) raises intracellular [Ca²⁺] through three routes:
- Voltage-gated Ca²⁺ channels (open with membrane depolarization - unlike skeletal muscle, even sub-threshold depolarization can open these)
- Ligand-gated Ca²⁺ channels (activated by hormones/neurotransmitters via G-proteins)
- IP₃-gated SR channels (hormones → PLC → IP₃ → Ca²⁺ release from SR)
- Additional amplification via Ca²⁺-induced Ca²⁺ release (CICR) through ryanodine receptors (RYR2 isoform) on the SR
-
Ca²⁺ binds calmodulin (4 Ca²⁺ ions cooperatively). The Ca²⁺-calmodulin complex activates MLCK.
-
MLCK phosphorylates the myosin light chain at serine-19 → increases myosin ATPase activity → myosin head binds actin → cross-bridge cycling → tension.
-
Calponin and caldesmon (thin filament proteins) also participate: at low [Ca²⁺], they inhibit myosin ATPase; rising Ca²⁺-calmodulin phosphorylates them, releasing their inhibition.
-
Relaxation occurs when [Ca²⁺] falls via: closing of voltage-gated channels (hyperpolarization), cAMP/cGMP-mediated channel inhibition, decreased IP₃ production, increased SR-Ca²⁺-ATPase activity, or activation of myosin light chain phosphatase (dephosphorylates myosin).
- Costanzo Physiology 7th Edition, pp. 49-50; Ganong's Review of Medical Physiology 26e, p. 127-128
4. Electrical Properties
- Resting membrane potential is typically -50 to -60 mV (less negative than skeletal muscle's ~-90 mV).
- Action potentials in smooth muscle have a slower time course, with a plateau phase mediated primarily by L-type Ca²⁺ channels (rather than Na⁺ channels as in skeletal muscle).
- Slow waves (pacemaker potentials) arise from spontaneous oscillations in membrane potential in unitary smooth muscle. When slow waves reach threshold, bursts of action potentials are superimposed, each followed by a contraction.
- Unlike skeletal and cardiac muscle, smooth muscle can be activated to contract by subthreshold depolarization alone - full action potentials are not required.
5. Autonomic Innervation and Pharmacology
Smooth muscle is innervated by the autonomic nervous system (both sympathetic and parasympathetic). Unlike skeletal muscle, there are no motor end plates - neurotransmitter is released en passant from varicosities along the nerve terminal and diffuses to the muscle.
- Acetylcholine (muscarinic receptors, via PLC/IP₃): depolarizes unitary smooth muscle, increases spike frequency, increases tone and contractility. - Ganong's 26e, p. 128
- Norepinephrine/epinephrine: typically hyperpolarizes intestinal smooth muscle (relaxation) by opening K⁺ channels (β₂ receptors), but contracts vascular smooth muscle (α₁ receptors).
- Unitary smooth muscle also shows 2 key autonomous properties: (1) spontaneous activity without nervous stimulation, and (2) contraction in response to stretch (myogenic response). Stretch → depolarization → increased spike frequency → increased tone. This is the physiological basis of Bayliss' myogenic response in blood vessels. - Ganong's 26e, p. 128
Relaxation pharmacology:
-
NO (nitric oxide) from endothelium → activates soluble guanylyl cyclase → ↑cGMP → protein kinase G activation → Ca²⁺ channel inhibition/enhanced Ca²⁺ removal → relaxation.
-
Phosphodiesterase V inhibitors (sildenafil, tadalafil) block cGMP breakdown → prolonged smooth muscle relaxation in corpus cavernosum and pulmonary vasculature.
-
β₂-agonists (albuterol) → ↑cAMP → relaxation of airway smooth muscle (used in asthma).
-
Ganong's 26e, p. 129
6. Mechanical Properties
- Smooth muscle contracts and relaxes slowly (cross-bridge cycling rate is ~100× slower than fast skeletal muscle).
- The latch-bridge mechanism allows sustained contraction with very little ATP expenditure: after MLCK activity declines and [Ca²⁺] falls, myosin cross-bridges remain attached to actin for prolonged periods in a high-force, low-energy state. This is especially important in vascular smooth muscle maintaining resting vessel tone. - Ganong's 26e, p. 127
- Smooth muscle can sustain prolonged contraction without fatigue.
- It can shorten to a much greater fraction of its resting length than skeletal muscle (up to 70-80%), allowing hollow organs like the bladder and uterus to change volume enormously.
- Plasticity: smooth muscle can adjust its resting length over a wide range and still generate near-maximal force - this is critical for organs like the bladder that fill and empty repeatedly.
7. Location and Functions
Smooth muscle is found in:
- GI tract - peristalsis and segmentation (two layers: inner circular, outer longitudinal)
- Vasculature - control of vessel caliber and blood pressure
- Bladder, ureter, uterus - propulsion and voiding
- Bronchioles - airway resistance regulation
- Iris and ciliary body - pupil diameter and lens accommodation
- Vas deferens, seminal vesicles
Its primary functions are: (1) producing motility/propulsion (e.g., chyme along the gut, urine along the ureter), and (2) maintaining sustained tension (e.g., vascular tone). - Costanzo Physiology 7th Edition, p. 48
Summary comparison with other muscle types:
| Property | Smooth | Cardiac | Skeletal |
|---|---|---|---|
| Striations | No | Yes | Yes |
| Sarcomeres | No | Yes | Yes |
| Troponin | No | Yes | Yes |
| Ca²⁺ regulator | Calmodulin/MLCK | Troponin C | Troponin C |
| Ca²⁺ source | ECF + SR (both) | ECF + SR (CICR) | SR only |
| T-tubules | No (caveolae instead) | Yes | Yes |
| Pacemaker | Some types | Yes (SA node) | No |
| Autonomic control | Yes | Yes | No |
| Speed of contraction | Slowest | Intermediate | Fastest |
| Fatigue resistance | Very high | Very high | Variable |
| Nuclear number | 1 (single) | 1-2 | Multiple (peripheral) |
Gut brain axis
Reading File
Finding Sources
Finding Sources
Searching PubMed
"gut-brain axis"[MeSH Terms] AND microbiota
Reading File
Reading File
Reading File
Searching PubMed
"gut-brain axis" AND microbiome
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have a thorough set of content from multiple authoritative sources. Let me compile the comprehensive answer.
The Gut-Brain Axis
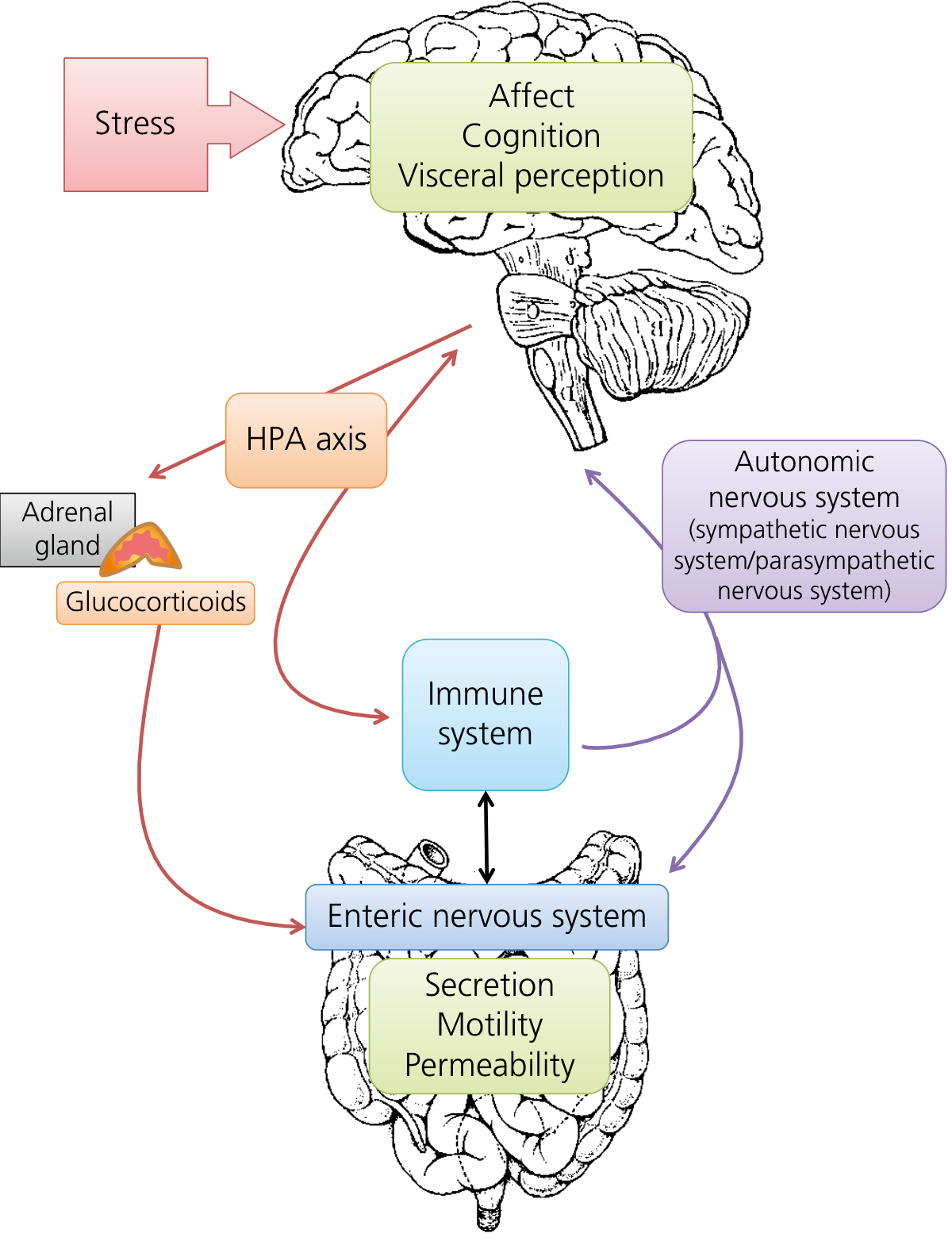
The gut-brain axis (GBA) is the bidirectional communication network linking the central nervous system (CNS), the enteric nervous system (ENS), the autonomic nervous system (ANS), the hypothalamic-pituitary-adrenal (HPA) axis, the immune system, and the intestinal microbiota. It integrates psychological, neuroendocrine, immune, and microbial signals to regulate GI function - and conversely, gut-derived signals shape brain function, mood, behavior, and disease. - Sleisenger & Fordtran's GI and Liver Disease
1. Structural Anatomy of the Axis
The Enteric Nervous System - "The Second Brain"
The ENS is the anatomical foundation of the gut-brain axis. It contains ~500 million neurons organized into two main plexuses:
- Myenteric (Auerbach's) plexus - between the longitudinal and circular muscle layers; primarily controls motility
- Submucosal (Meissner's) plexus - in the submucosa; controls secretion and local blood flow
The ENS possesses marked independence: it can regulate peristalsis, secretion, and blood flow even after complete dissection from the brain and spinal cord. Yet it receives modulatory input from the CNS via the vagus nerve (parasympathetic) and sympathetic fibers from prevertebral ganglia. - Yamada's Textbook of Gastroenterology 7e
The Vagus Nerve - The Highway
The vagus nerve is the principal communication route between gut and brain:
-
Afferent (gut → brain): ~80% of vagal fibers are sensory, carrying information from chemoreceptors, osmoreceptors, and mechanoreceptors in the gut mucosa to autonomic centers in the medulla. These form vagovagal reflexes - loops that integrate gut sensory input at the brainstem and send efferent motor output back to the ENS.
-
Efferent (brain → gut): Preganglionic parasympathetic fibers from the dorsal motor nucleus of the vagus synapse on ENS neurons. Parasympathetic stimulation (overall) increases secretion and motility.
-
The vagus nerve innervates the gut from the pharynx to the distal colon; the remaining distal colon and rectum receive parasympathetic innervation from pelvic nerves (S2-S4).
-
Medical Physiology (Boron & Boulpaep), p. 1279-1280
Sympathetic Innervation
Preganglionic sympathetic fibers synapse in prevertebral ganglia (celiac, superior/inferior mesenteric), releasing ACh. Postganglionic fibers synapse either in the ENS or directly on effector cells (gut smooth muscle, secretory cells, blood vessels). Sympathetic activation generally inhibits GI motility and secretion and reduces blood flow to the gut (e.g., fight-or-flight response). - Medical Physiology (Boron & Boulpaep)
Hierarchical Reflex Loops
The ANS operates in hierarchical levels:
- ENS (lowest level) - independent reflexes
- Autonomic ganglia - control ENS and other organs
- Spinal cord - integrates across levels
- Brainstem - coordinates all visceral control
- Forebrain (hypothalamus, limbic system, cortex) - top-down modulation of all lower centers
2. Communication Pathways
A. Neural Pathways
| Direction | Route | Key Signals |
|---|---|---|
| Bottom-up (gut → brain) | Vagal afferents, spinal afferents | Mechanosensory, chemosensory, nociceptive, hormonal |
| Top-down (brain → gut) | Vagal efferents, sympathetic efferents | ACh, norepinephrine, neuropeptides |
B. Neuroendocrine / HPA Axis Pathway
The HPA axis is the primary neuroendocrine limb of the stress response:
- Stress → hypothalamus releases corticotropin-releasing factor (CRF)
- CRF → anterior pituitary releases ACTH
- ACTH → adrenal cortex releases cortisol
- Cortisol feeds back to hypothalamus/pituitary (negative feedback) AND acts directly on gut:
- Increases colonic motility
- Increases visceral sensitivity
- Promotes mast cell degranulation
- Increases intestinal permeability
- Modulates the local gut immune response
CRF also acts as a neurotransmitter, directly activating the ANS and modulating ENS function independently of cortisol. - Yamada's Textbook of Gastroenterology 7e, p. 1459
C. Immune Pathway
The intestinal immune system communicates bidirectionally with the nervous system:
- Activated mast cells and mucosal immune cells release cytokines (IL-1β, IL-6, TNF-α) that activate afferent sensory neurons
- The vagus nerve has anti-inflammatory properties: vagal efferent activity suppresses peripheral cytokine release via the cholinergic anti-inflammatory pathway (ACh acting on α7-nicotinic receptors on macrophages)
- Post-infectious IBS is associated with persistently increased gut lymphocytes, enterochromaffin cells, and IL-1β expression, linking prior immune activation to chronic gut-brain dysregulation - Yamada's 7e, p. 1461
D. Enteroendocrine / Humoral Signaling
Enteroendocrine cells (EECs), which constitute the largest endocrine organ in the body, release hormones that act on the ENS, vagal afferents, and the brain:
| Hormone | Cell type | Key action |
|---|---|---|
| Serotonin (5-HT) | Enterochromaffin (EC) cells | ~90% of body's 5-HT; stimulates vagal afferents → brain; regulates motility via 5-HT3/5-HT4 receptors on ENS |
| Cholecystokinin (CCK) | I cells (duodenum/jejunum) | Vagal afferent activation → satiety signaling in brain |
| Ghrelin | Gastric X/A cells | Hunger signal; crosses blood-brain barrier |
| GLP-1, PYY | L cells (ileum/colon) | Satiety, insulin secretion, gut motility |
Serotonin deserves special emphasis: EC cells sense luminal contents (pressure, pH, nutrients) and release 5-HT, which activates 5-HT3 receptors on vagal afferent nerve terminals. These carry signals to the brainstem (nodose ganglia → NTS). Within the gut, 5-HT coordinates peristalsis via both ascending excitatory and descending inhibitory interneurons of the ENS. - Sleisenger & Fordtran's, p. 67
3. The Microbiota-Gut-Brain Axis
The gut microbiome (trillions of microorganisms) adds a critical third dimension to the gut-brain axis, creating the microbiota-gut-brain (MGB) axis. Communication is bidirectional:
Top-down (Brain → Microbiota)
- Stress, psychological states, and experiences alter intestinal microbiota composition in animal models
- Mechanism: ANS-mediated changes in gut motility, secretion, mucus, and permeability change the gut environment, which selects for different microbial populations
- Norepinephrine released under stress can directly stimulate bacterial growth
Bottom-up (Microbiota → Brain)
Gut microbes influence the brain through at least four routes:
-
ENS activation - Microbes alter ENS function; ENS signals are relayed to CNS via the vagus nerve. Ingestion of Lactobacillus rhamnosus changed GABA receptor expression in limbic brain regions and reduced anxiety/depression - an effect blocked by vagotomy, proving vagal dependence. - Harrison's Principles of Internal Medicine 22e, p. 3442
-
HPA axis programming - Microbial metabolites (especially SCFAs) target areas not protected by the blood-brain barrier (BBB), including the hypothalamus. Neonatal microbiota program HPA axis stress reactivity across the lifespan - germ-free animals show exaggerated HPA responses that are normalized by microbial colonization. - Sleisenger & Fordtran's
-
Bloodborne microbial metabolites crossing the BBB
- Short-chain fatty acids (SCFAs) - butyrate, propionate, acetate; produced by bacterial fermentation of dietary fiber; regulate BDNF production, microglial development, and epigenetic changes in brain cells
- Tryptophan metabolites - serotonin precursors and kynurenine pathway products; influence serotonergic signaling
- Secondary bile acids - affect neuroinflammation via TGR5 and FXR receptors
- Bacterial neurotransmitters - gut bacteria produce GABA, serotonin, dopamine precursors, and neuroactive peptides
-
Immune modulation - Microbiota are required for normal development and function of brain microglia (CNS-resident immune cells); dysbiosis → immune dysregulation → neuroinflammation
- Harrison's Principles 22e; Sleisenger & Fordtran's GI and Liver Disease
4. Stress and the Gut-Brain Axis
The gut-brain axis is the neuroanatomic substrate of the biopsychosocial model of GI disease. Stress has well-documented effects on GI function:
- Cannon (1915): Observed cessation of bowel activity in cats exposed to a growling dog
- Pavlov: Demonstrated that psychic stimuli alter gastric acid secretion via the vagus
- Beaumont & Wolf: Observed direct mucosal changes (hyperemia, altered motility/secretion) in response to emotions (anger, anxiety)
Stress effects on the gut:
-
Increased colonic motility (CRF-mediated)
-
Increased visceral sensitivity (central and peripheral sensitization)
-
Increased intestinal permeability ("leaky gut") - allowing translocation of bacterial products and antigens
-
Mast cell degranulation → histamine and cytokine release → sensitization of afferent neurons
-
Altered microbiota composition
-
Sleisenger & Fordtran's, pp. 350-351; Yamada's 7e, pp. 1459-1461
5. Clinical Relevance - Disorders of Gut-Brain Interaction (DGBIs)
The gut-brain axis is central to the pathophysiology of functional GI disorders, now renamed DGBIs (Rome IV classification):
Irritable Bowel Syndrome (IBS)
IBS is the prototype DGBI. Key gut-brain mechanisms:
- Visceral hypersensitivity - lowered pain thresholds in the gut, partly from central sensitization (altered pain processing in brain) and peripheral sensitization (sensitized mucosal afferents)
- Altered motility - exaggerated motility response to stress
- HPA dysregulation - chronic stress is the strongest predictor of IBS symptom intensity over time
- Post-infectious IBS - acute gut infection → persistent immune activation → altered ENS → IBS; predicted by psychological stress and anxiety at time of infection
- Dysbiosis - altered microbiome composition contributes to both gut and central symptoms
Treatment: Central neuromodulators - TCAs (e.g., amitriptyline 10-25 mg at bedtime) and SSRIs act on the gut-brain axis to reduce visceral hypersensitivity, not just mood; 5-HT3 antagonists (e.g., alosetron) reduce diarrhea; 5-HT4 agonists (e.g., prucalopride) treat constipation. - Goldman-Cecil Medicine, p. 1419
Neurodegenerative Diseases
A striking recent insight is the gut-to-brain propagation of pathological proteins:
In Parkinson's disease (PD), the Braak staging hypothesis proposes that α-synuclein aggregates originate in the ENS (and olfactory bulb), then propagate retrogradely via the vagus nerve to the brainstem, substantia nigra, limbic system, and cortex. This matches the clinical sequence: constipation and anosmia (nonmotor symptoms, years before diagnosis) → anxiety/depression → parkinsonism → dementia. - Harrison's Principles 22e, p. 3536
Other neurological diseases with gut-brain connections:
-
Autism Spectrum Disorder (ASD) - children with ASD have documented dysbiosis; severity of dysbiosis correlates with autism severity; murine models show microbiome manipulation can ameliorate ASD behaviors (IL-17 implicated)
-
Multiple sclerosis - A. muciniphila peptides may drive cross-reactive immune responses via molecular mimicry (HLA-related)
-
Alzheimer's disease - gut dysbiosis → neuroinflammation → amyloid processing (active research area)
-
Guillain-Barré syndrome - Campylobacter jejuni molecular mimicry of GM1 ganglioside
-
Hepatic encephalopathy - gut bacterial metabolites (ammonia, etc.) directly worsen brain function; treated with rifaximin/lactulose
-
Harrison's Principles of Internal Medicine 22e
Psychiatric Disorders
- Depression and anxiety - gut dysbiosis and altered 5-HT production are implicated; gut microbiota influence BDNF levels, GABA receptor expression, and HPA reactivity
- Anorexia nervosa / eating disorders - gut hormones (ghrelin, CCK, GLP-1) modulate satiety circuits
- Germ-free mice display reduced anxiety, less stress reactivity, more exploratory behavior, and impaired memory - all reversible with microbial colonization
6. Microbiome as a Therapeutic Target
| Target | Approach |
|---|---|
| Dysbiosis | Probiotics, prebiotics, fecal microbiota transplant (FMT) |
| Visceral hypersensitivity | Central neuromodulators (TCAs, SSRIs, SNRIs) |
| Airway smooth muscle (asthma) | β₂ agonists (albuterol) |
| Gut motility | 5-HT3 antagonists, 5-HT4 agonists |
| Hepatic encephalopathy | Rifaximin, lactulose (reduce gut-derived toxins) |
| Depression/anxiety | Psychobiotics (probiotic strains targeting mood) |
| Obesity | Microbiome manipulation (FMT from lean donors improves insulin sensitivity) |
Summary
BRAIN (affect, cognition, visceral perception)
↕ (vagal afferents/efferents)
HPA AXIS (CRF → ACTH → cortisol)
↕
AUTONOMIC NERVOUS SYSTEM (sympathetic + parasympathetic)
↕
ENTERIC NERVOUS SYSTEM (myenteric + submucosal plexus)
↕ (immune system)
GUT EPITHELIUM & MICROBIOTA
(serotonin, SCFAs, bile acids, neurotransmitters, cytokines)
The axis is not simply a "gut-to-brain" or "brain-to-gut" pathway - it is a genuinely bidirectional, multi-channel system where disruption at any level (dysbiosis, mucosal inflammation, psychological trauma, altered ENS wiring) propagates throughout the entire network.
Recent literature: Reviews in 2023-2025 continue to expand this field - the diet-microbiota-gut-brain axis (Schneider et al., Nature Metabolism 2024, PMID 39174768) and the gut microbiota-immune-brain axis with therapeutic implications (O'Riordan et al., Cell Reports Medicine 2025, PMID 40054458) are particularly relevant for clinical translation.
Mechanism of intestinal secretion at MBBS level
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
All content needed is gathered. Now let me compile the comprehensive MBBS-level answer.
Mechanism of Intestinal Secretion
Overview: The Fluid Budget of the GI Tract
The intestine is simultaneously the body's largest secretory AND absorptive organ. Each day:
| Source | Volume |
|---|---|
| Saliva | ~1.5 L |
| Gastric juice | ~2.0 L |
| Bile | ~0.5 L |
| Pancreatic juice | ~1.5 L |
| Small intestinal secretion | ~1.8 L |
| Total entering small intestine | ~7-9 L/day |
| Absorbed by small intestine | ~6.5-7.5 L |
| Reaching colon | ~1 L |
| Stool loss | ~0.2 L |
The intestine secretes fluid primarily to create a watery vehicle that keeps luminal contents in solution, facilitating digestion and absorption. - Guyton & Hall Medical Physiology; Harrison's Principles 22e
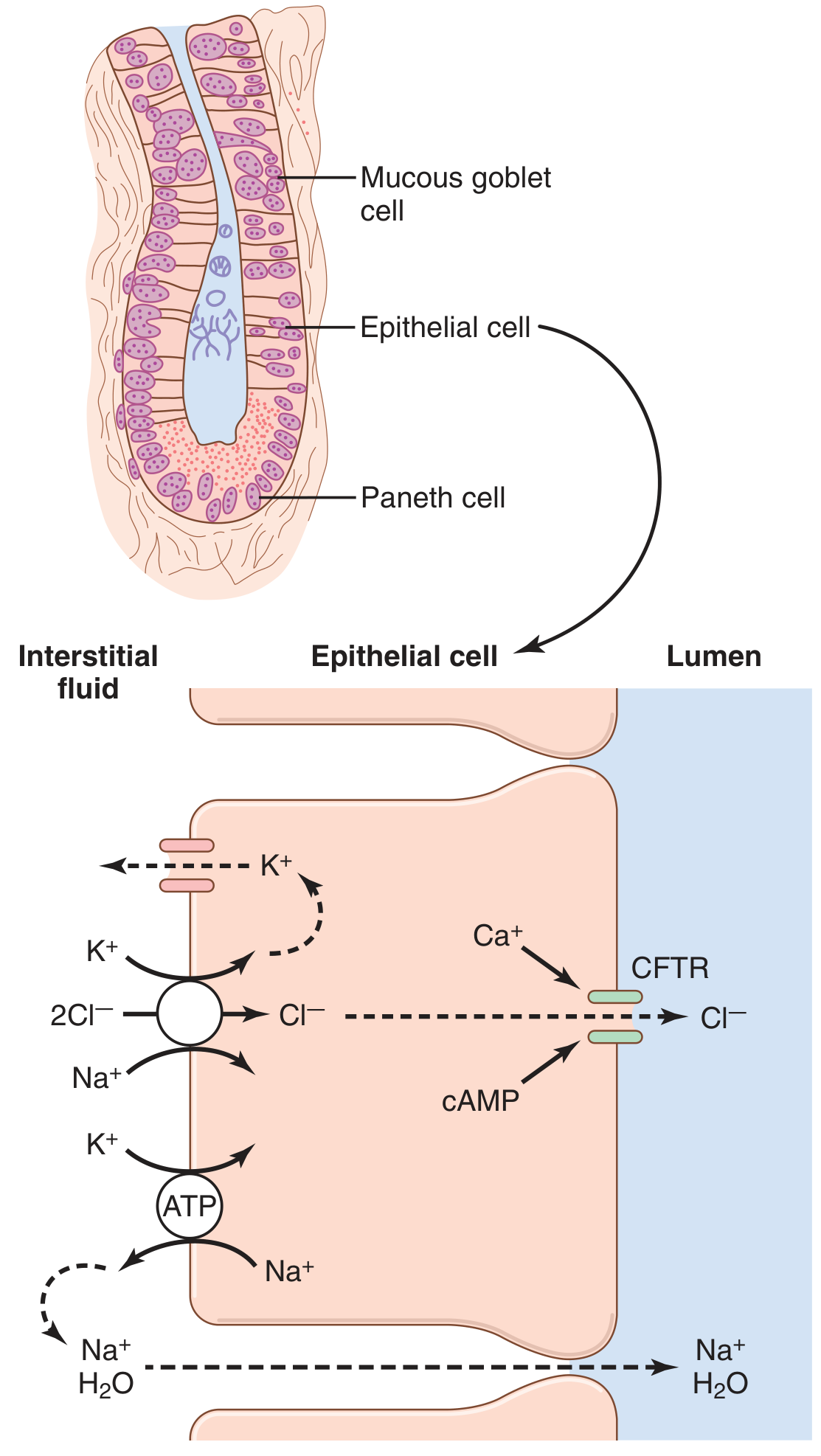
1. Anatomical Basis: The Crypt-Villus Unit
The small intestinal epithelium is organized into a functional absorptive-secretory unit:
- Villi (finger-like projections): covered by enterocytes that absorb fluid, electrolytes, and nutrients
- Crypts of Lieberkühn (pits between villi): lined by epithelial cells (enterocytes + goblet cells + Paneth cells) that secrete fluid and electrolytes
This creates a "crypt-to-villus" fluid circulation: crypts pour out ~1800 mL/day of alkaline, nearly enzyme-free fluid (pH 7.5-8.0), which flows up over the villi, where it is then reabsorbed along with digested nutrients. The net result is a washing, solubilizing flow that keeps the luminal surface in a fluid-rich environment for absorption. - Guyton & Hall Medical Physiology, p. 811
2. Core Cellular Mechanism: Cl⁻-Driven Secretion
The driving force for intestinal fluid secretion is active Cl⁻ secretion from crypt enterocytes. Na⁺ and water follow passively. Here are the steps:
Step-by-Step (Crypt Cell)
Step 1 - Energy generation by basolateral Na⁺-K⁺-ATPase
- The Na⁺-K⁺-ATPase pump on the basolateral membrane continuously pumps 3 Na⁺ out and 2 K⁺ in, using ATP.
- This maintains a low intracellular Na⁺ concentration and a negative intracellular electrical potential - the driving force for the next step.
Step 2 - Cl⁻ entry via the NKCC1 cotransporter (basolateral)
- The low intracellular Na⁺ drives the Na⁺-K⁺-2Cl⁻ (NKCC1) cotransporter on the basolateral membrane.
- This brings Na⁺, K⁺, and 2Cl⁻ into the cell together from the interstitial fluid.
- Result: intracellular [Cl⁻] rises above its electrochemical equilibrium.
Step 3 - K⁺ recycling (basolateral)
- The K⁺ brought in by NKCC1 exits back across the basolateral membrane through basolateral K⁺ channels (KCNQ1, etc.).
- This keeps intracellular [K⁺] in check and maintains the negative membrane potential.
Step 4 - Cl⁻ exits apically through CFTR channels
- Cl⁻, which has accumulated inside the cell, now moves down its electrochemical gradient out through CFTR (Cystic Fibrosis Transmembrane conductance Regulator) Cl⁻ channels in the apical membrane into the intestinal lumen.
- CFTR channels are normally closed at rest - they must be opened by intracellular signals (see below).
- Other apical Cl⁻ channels (Ca²⁺-activated CaCC channels) also contribute.
Step 5 - Na⁺ follows paracellularly
- Cl⁻ secretion into the lumen creates a negative lumenal charge.
- Na⁺ is dragged through the paracellular pathway (tight junctions) by this electrochemical gradient.
Step 6 - Water follows osmotically
-
The accumulation of NaCl in the lumen creates an osmotic gradient.
-
Water moves osmotically from the cell and interstitium into the lumen.
-
Net result: secretion of isotonic NaCl solution into the lumen.
-
Costanzo Physiology 7th Edition, p. 391-392; Guyton & Hall, p. 811
3. Regulation: What Opens the Cl⁻ Channels?
CFTR channels are the key regulated step. They are normally closed; their opening is controlled by second messenger systems activated by neurotransmitters, hormones, and bacterial toxins:
A. cAMP Pathway (most important)
Secretagogue (VIP, ACh, PGE₂, cholera toxin)
↓
Gs protein → Adenylyl cyclase activated
↓
ATP → cAMP ↑
↓
Protein Kinase A (PKA) activated
↓
PKA phosphorylates CFTR → CFTR Cl⁻ channel OPENS
↓
Cl⁻ secretion → Na⁺ + H₂O follow → Net fluid secretion
Key secretagogues acting via cAMP:
- VIP (Vasoactive Intestinal Peptide) - the most potent endogenous secretagogue
- Prostaglandins (PGE₂, PGI₂) - released during inflammation; explain secretory diarrhea in enteritis
- Secretin - from S cells of duodenum; stimulates pancreatic and intestinal secretion
- Cholera toxin (see below)
B. Ca²⁺ Pathway
Secretagogue (ACh via muscarinic M3, 5-HT, substance P)
↓
Gq protein → Phospholipase C activated
↓
PIP₂ → IP₃ + DAG
↓
IP₃ → Ca²⁺ release from ER; DAG → PKC
↓
↑ intracellular Ca²⁺ → Ca²⁺-activated CaCC channels open
↓
Cl⁻ secretion → fluid secretion
- Acetylcholine (from ENS neurons): major neural secretagogue - acts via M3 receptors → ↑Ca²⁺
- Serotonin (5-HT): released by enterochromaffin cells in response to luminal stimuli → activates ENS neurons → Cl⁻ secretion
- Substance P, neurotensin: neuropeptides released by ENS
C. cGMP Pathway
-
Heat-stable E. coli enterotoxin (STa): binds guanylyl cyclase C (GCC) receptor on apical membrane → ↑cGMP → activates PKG → phosphorylates CFTR
-
Guanylin and uroguanylin: endogenous peptides that physiologically activate GCC → regulate fluid balance
-
Linaclotide, plecanatide: drugs for constipation that mimic guanylin → activate GCC → ↑ intestinal secretion/motility
-
Medical Physiology (Boron & Boulpaep), p. 2084-2087
Summary Table: Secretagogues and Their Mechanisms
| Secretagogue | Source | Receptor | 2nd Messenger | Clinical Relevance |
|---|---|---|---|---|
| VIP | ENS neurons | VPAC1/2 (Gs) | ↑ cAMP | Verner-Morrison syndrome (VIPoma) |
| Cholera toxin | V. cholerae | ADP-ribosylates Gs | ↑↑↑ cAMP (irreversible) | Cholera - "rice water" diarrhea |
| E. coli STa | ETEC | GCC receptor | ↑ cGMP | Traveler's diarrhea |
| ACh | ENS, vagus | M3 (Gq) | ↑ Ca²⁺ | Normal secretory regulation |
| Serotonin (5-HT) | Enterochromaffin | 5-HT3/4 | ↑ Ca²⁺ / cAMP | Carcinoid syndrome |
| PGE₂ | Immune cells, epithelium | EP2/EP4 (Gs) | ↑ cAMP | Inflammatory diarrhea |
| Linaclotide | Drug | GCC | ↑ cGMP | Treatment of IBS-C |
4. Neural Regulation
The most important physiological regulator of intestinal secretion is the enteric nervous system (ENS). Local neural reflexes dominate:
- Tactile/chemical stimulation of mucosal mechanoreceptors and chemoreceptors (e.g., by chyme) → activate submucosal plexus neurons
- These release VIP and ACh onto crypt cells → Cl⁻ secretion
- Parasympathetic stimulation (vagus nerve, pelvic nerves) → increases secretion via ENS
- Sympathetic stimulation → generally inhibits secretion (α₂ adrenergic receptors → ↓cAMP; also α-adrenergic stimulation increases NaCl absorption)
"By far the most important means for regulating small intestine secretion are local enteric nervous reflexes, especially reflexes initiated by tactile or irritative stimuli from the chyme in the intestines." - Guyton & Hall Medical Physiology, p. 811
5. Composition of Intestinal Secretion
| Component | Details |
|---|---|
| Volume | ~1800 mL/day from small intestine |
| pH | 7.5-8.0 (slightly alkaline due to HCO₃⁻) |
| Electrolytes | Na⁺, Cl⁻, HCO₃⁻, K⁺ (isotonic with plasma) |
| Enzymes | None in the secreted fluid itself |
| Mucus | From goblet cells - lubricates and protects |
| Paneth cell secretions | Defensins (antimicrobial peptides), lysozyme - into crypt lumen |
Note: Brush border enzymes (sucrase, maltase, lactase, peptidases) are membrane-bound on villus enterocyte apical surface - they are not secreted into the lumen. - Guyton & Hall, p. 811
6. Large Intestine Secretion
The large intestine has no villi and no digestive enzymes. Its crypts of Lieberkühn secrete:
- Mucus only (from abundant goblet cells) - the dominant secretion
- Small amount of NaHCO₃ - neutralizes acid from bacterial fermentation
- Volume: much smaller than small intestine (~few hundred mL/day at most)
Regulation:
- Direct tactile stimulation of epithelium → reflex mucus secretion
- Parasympathetic stimulation (pelvic nerves, S2-S4) → marked increase in mucus secretion + peristalsis
- Extreme parasympathetic activation (emotional disturbance) → copious ropy mucus without feces
Function of colonic mucus:
- Protects wall from mechanical excoriation
- Holds fecal matter together
- Shields epithelium from bacterial activity and their metabolic acids
- The alkaline (pH 8.0) HCO₃⁻-rich mucus neutralizes acidic fermentation products
- Guyton & Hall Medical Physiology, p. 812
7. Clinical Application: Secretory Diarrhea
Understanding the secretion mechanism directly explains the pathophysiology of secretory diarrhea:
Cholera (prototype)
- Vibrio cholerae colonizes small intestine → releases cholera toxin (CT)
- CT B subunit binds GM1 ganglioside on apical membrane → A subunit enters cell
- A subunit catalyzes ADP-ribosylation of Gsα → Gsα locked in active (GTP-bound) state
- Adenylyl cyclase permanently activated → cAMP remains maximally elevated
- CFTR channels stay permanently open → massive Cl⁻ secretion
- Na⁺ and H₂O follow → up to 20 L/day of "rice-water stool"
- Electrolyte losses: HCO₃⁻ loss → metabolic acidosis; K⁺ loss → hypokalemia
Oral Rehydration Solution (ORS) - Exploiting Normal Absorption
The key insight: cholera toxin increases cAMP and opens CFTR, but it does NOT affect the Na⁺-glucose cotransporter (SGLT1) on villus cells. Therefore:
- ORS (glucose + Na⁺ + Cl⁻ + HCO₃⁻ + K⁺) → SGLT1 absorbs Na⁺ with glucose → water follows
- This absorption mechanism works normally even in cholera
- This is the basis of WHO Oral Rehydration Therapy - arguably one of the greatest public health achievements
Types of Diarrhea (MBBS)
| Type | Mechanism | Example | Key Feature |
|---|---|---|---|
| Secretory | Excess Cl⁻ secretion via cAMP/cGMP/Ca²⁺ | Cholera, ETEC, VIPoma | Persists with fasting; large volume; isotonic |
| Osmotic | Non-absorbed solutes retain water in lumen | Lactase deficiency, lactulose | Stops with fasting; osmotic gap in stool |
| Exudative/Inflammatory | Mucosal damage → protein/blood/mucus loss | IBD, invasive bacteria | Blood/mucus in stool |
| Motility | Rapid transit → reduced absorption time | IBS-D, hyperthyroidism | Small volume, urgency |
- Costanzo Physiology 7th Edition, p. 392-393
Quick Revision Summary (MBBS)
CRYPT CELL SECRETION (active Cl⁻ secretion)
Basolateral:
Na⁺-K⁺-ATPase → lowers intracellular Na⁺ (uses ATP)
NKCC1 cotransporter → Na⁺ + K⁺ + 2Cl⁻ enter cell (driven by low intracellular Na⁺)
K⁺ channels → K⁺ recycles back out
Apical:
CFTR Cl⁻ channels (normally CLOSED)
Opened by: cAMP (via VIP, cholera toxin) or Ca²⁺ (via ACh, 5-HT) or cGMP (via STa, guanylin)
Cl⁻ exits into lumen
Na⁺ follows paracellularly (electrochemical drag)
H₂O follows osmotically
→ Isotonic NaCl fluid secreted into lumen
→ Absorbed by villus cells further up (net absorption normally)
→ If secretion overwhelms absorption → DIARRHEA
Create a diagram poster comparing cAMP vs Ca²⁺ pathways of intestinal secretion
Generating Image
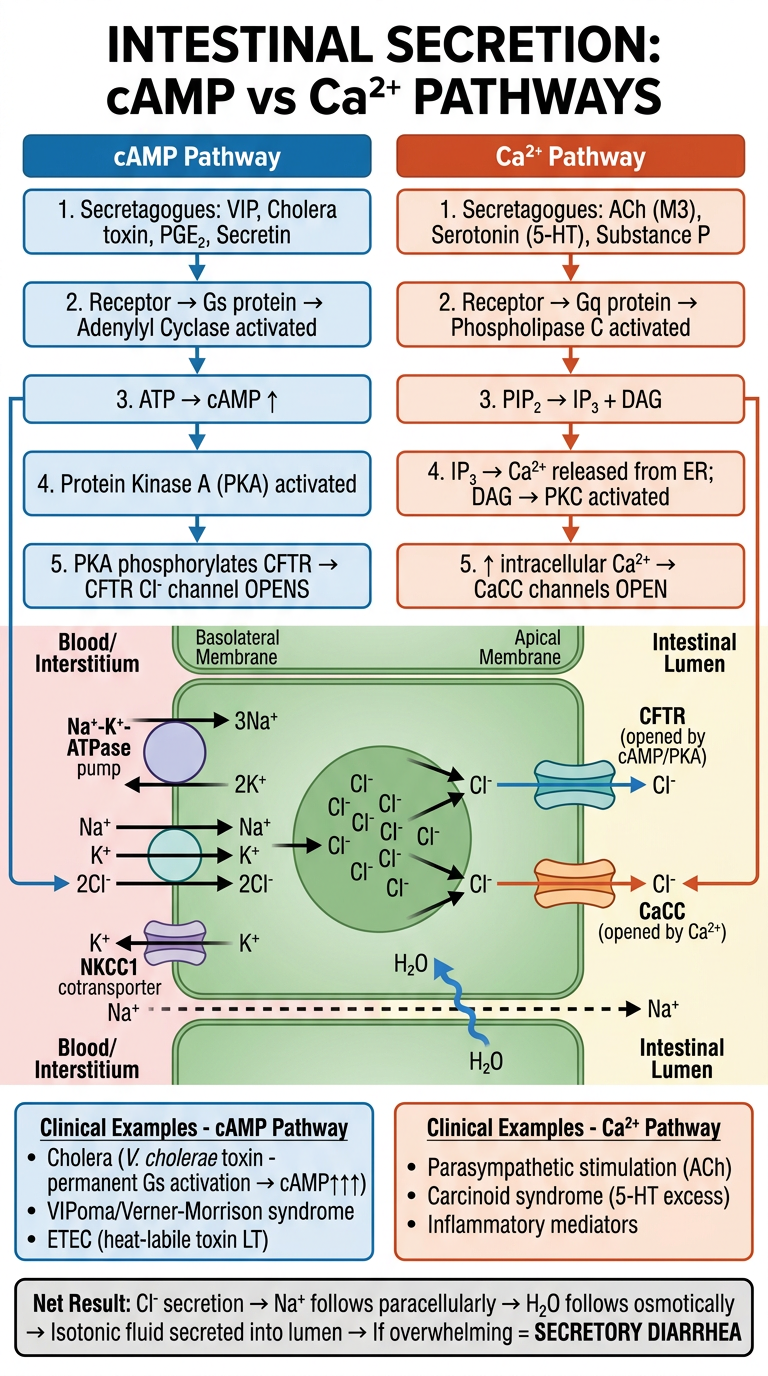
Here's your poster comparing the two major signaling pathways driving intestinal Cl⁻ secretion. Key points illustrated:
cAMP Pathway (blue):
- Triggered by VIP, cholera toxin, PGE₂, secretin
- Gs → adenylyl cyclase → cAMP → PKA → CFTR phosphorylation and opening
- Cholera toxin irreversibly ADP-ribosylates Gsα → permanently elevated cAMP → massive fluid loss
Ca²⁺ Pathway (orange):
- Triggered by ACh (M3), serotonin (5-HT), substance P
- Gq → PLC → IP₃ + DAG → Ca²⁺ release from ER → CaCC channels open
- Also activates PKC, which can synergize with cAMP
Common final pathway (center cell):
Both pathways converge on opening apical Cl⁻ channels. Cl⁻ exits into the lumen, Na⁺ follows paracellularly by electrochemical drag, and water follows osmotically - producing isotonic fluid secretion.
This is a shared conversation. Sign in to Orris to start your own chat.