Hydrocele
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive content to construct a thorough answer on hydrocele. Here's a complete overview:
Hydrocele
Definition
A hydrocele is a fluid collection that resides in the tunica vaginalis in the scrotum or in the processus vaginalis in the inguinal canal. — Mulholland and Greenfield's Surgery, 7e
Embryology & Pathophysiology
During fetal development, the testicle descends from the retroperitoneum to the scrotum in the third trimester. A peritoneal extension — the processus vaginalis — accompanies it. As the testis settles in the scrotum, the processus vaginalis normally forms the tunica vaginalis (a serous covering around the testis) and then obliterates, closing the communication between the peritoneal cavity and the inguinal canal.
Failure of obliteration leads to a spectrum of conditions:
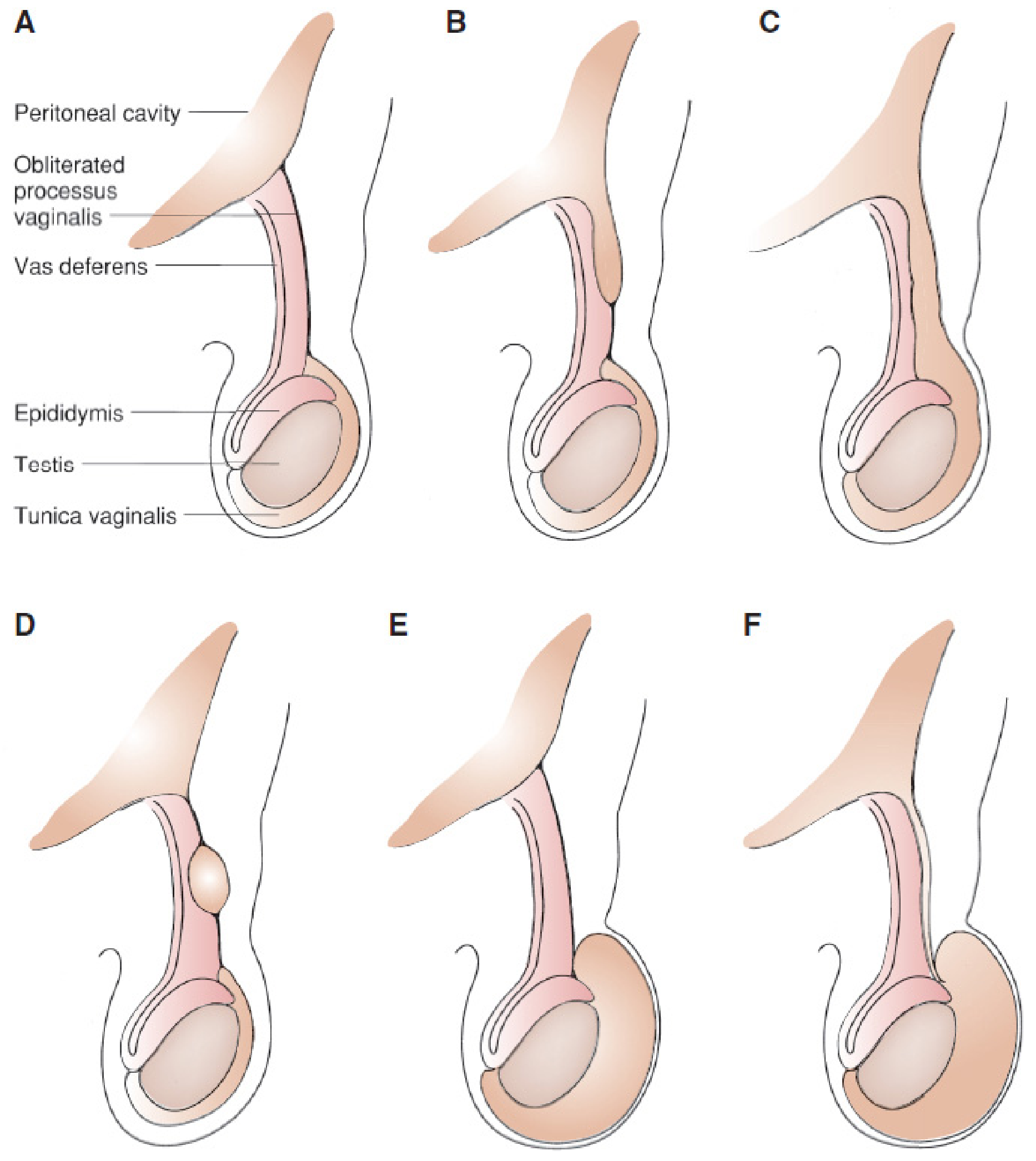
Figure: Anatomic variations with different degrees of obliteration of the processus vaginalis. (A) Normal. (B) Proximal hernia sac; distal obliterated. (C) Hernia sac extending into scrotum. (D) Hydrocele of the cord. (E) Scrotal hydrocele, obliterated processus. (F) Patent processus — communicating hydrocele. — Mulholland and Greenfield's Surgery, 7e
The incidence of patent processus vaginalis is 80–94% in newborns and decreases to 20–30% in adults, indicating ongoing obliteration with age.
Classification
| Type | Description |
|---|---|
| Communicating hydrocele | Patent processus vaginalis maintains direct communication with the peritoneal cavity; fluid volume fluctuates (enlarges with activity/crying, reduces when supine). Synonymous with patent processus vaginalis. |
| Non-communicating hydrocele | Isolated fluid collection in the tunica vaginalis; no peritoneal communication. Typically asymptomatic and self-resolving. |
| Hydrocele of the cord | Fluid trapped in the processus vaginalis separate from the tunica vaginalis (males). |
| Hydrocele of the canal of Nuck | Equivalent in females — fluid trapped in the processus vaginalis. |
| Abdominoscrotal hydrocele | Uncommon (~1.25% of all hydroceles); a tense, noncommunicating scrotal mass that extends into the abdomen; bilateral in ~30% of cases. |
Clinical Features
- Presentation: Painless scrotal swelling, usually unilateral. A history of fluctuating size (larger after activity, smaller in the morning) strongly suggests a communicating hydrocele.
- Transillumination: A hydrocele transilluminates brightly with a handheld light — key examination finding distinguishing it from a solid scrotal mass.
- Acute hydrocele: May arise suddenly secondary to incarcerated hernia, torsion of the appendix testis, or reactive inflammation. With acute non-communicating hydrocele, normal cord structures can be palpated above the mass and bowel obstruction symptoms are absent (helpful in differentiating from incarcerated hernia).
- Abdominoscrotal hydrocele: Palpable abdominal mass + tense scrotal swelling; ultrasound helps delineate the proximal extent.
Diagnosis
- Clinical (history + physical examination) is usually sufficient.
- Transillumination confirms fluid-filled nature.
- Scrotal ultrasound: Used when diagnosis is uncertain, to rule out testicular pathology, or to define extent in abdominoscrotal hydroceles.
Management
Conservative
- Non-communicating hydrocele in infants: Observation is appropriate — the majority resolve spontaneously before 12 months of age.
Surgical Indications
Operative management is indicated for:
- Non-communicating hydrocele persisting beyond 12 months of age
- Acute enlargement of the hydrocele
- Any question of communication with the peritoneal cavity (communicating hydrocele = patent processus vaginalis → always repaired electively)
- Abdominoscrotal hydrocele
Surgical Approach
- The communicating hydrocele is treated operatively in the same fashion as an indirect inguinal hernia — high ligation of the processus vaginalis via an inguinal approach.
- In adults, surgical options include Lord's procedure (plication), Jaboulay's procedure (eversion of the tunica vaginalis), or excision of the sac.
Post-Varicocelectomy Hydrocele
A specific secondary type: hydrocele formation is the most common complication after non-microscopic varicocelectomy (incidence 3–33%, average ~7%). It results from lymphatic obstruction during cord dissection. Using magnification (operating microscope) to identify and preserve lymphatics almost eliminates this risk. At least half of post-varicocelectomy hydroceles grow large enough to warrant surgical excision. — Campbell-Walsh-Wein Urology
Key Points
- Transillumination is the hallmark physical sign.
- Communicating hydrocele = patent processus vaginalis → always treat surgically.
- Non-communicating hydrocele in infants → observe until 12 months; most resolve.
- Fluctuating size = communicating hydrocele (diagnostic).
- Must differentiate from incarcerated hernia (no bowel obstruction symptoms, transilluminates, cord palpable above mass) and from testicular tumors (solid, does not transilluminate).
This is a shared conversation. Sign in to Orris to start your own chat.