Types of asthma atopic asthma vs no atopic asthma and how to diagnose them. Guide with proper management lines according to international protocols
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive, evidence-based guide on asthma types and management.
Asthma: Types, Diagnosis, and Management
1. Overview and Classification
The asthma syndrome is characterized by marked heterogeneity in clinical expression, environmental triggers, and immunopathologic mechanisms. Traditionally, only two forms were recognized — atopic and non-atopic — but this is an oversimplification. Multiple underlying pathobiologic mechanisms (endotypes) underlie the classic signs and symptoms. — Goldman-Cecil Medicine
2. Atopic (Allergic / Extrinsic) Asthma
Definition & Epidemiology
- The most common and most studied subtype
- Characterized by IgE-mediated sensitization to environmental allergens
- Found in nearly all school-aged children with asthma and ~50% of adult asthmatics
Pathophysiology
| Component | Role |
|---|---|
| TH2 cells | Produce IL-4, IL-5, IL-13; drive IgE production and eosinophil recruitment |
| IL-4 | Induces B-cell proliferation and IgE class switching |
| IL-13 | Airway hyperresponsiveness, goblet cell metaplasia, mucus hypersecretion |
| IL-5 | Eosinophil formation, maturation, recruitment, and survival |
| Mast cells | Activated by allergen–IgE binding; release histamine, leukotrienes, prostaglandins → bronchoconstriction |
| Eosinophils | Accumulate after allergen exposure; key biomarker predicting ICS response |
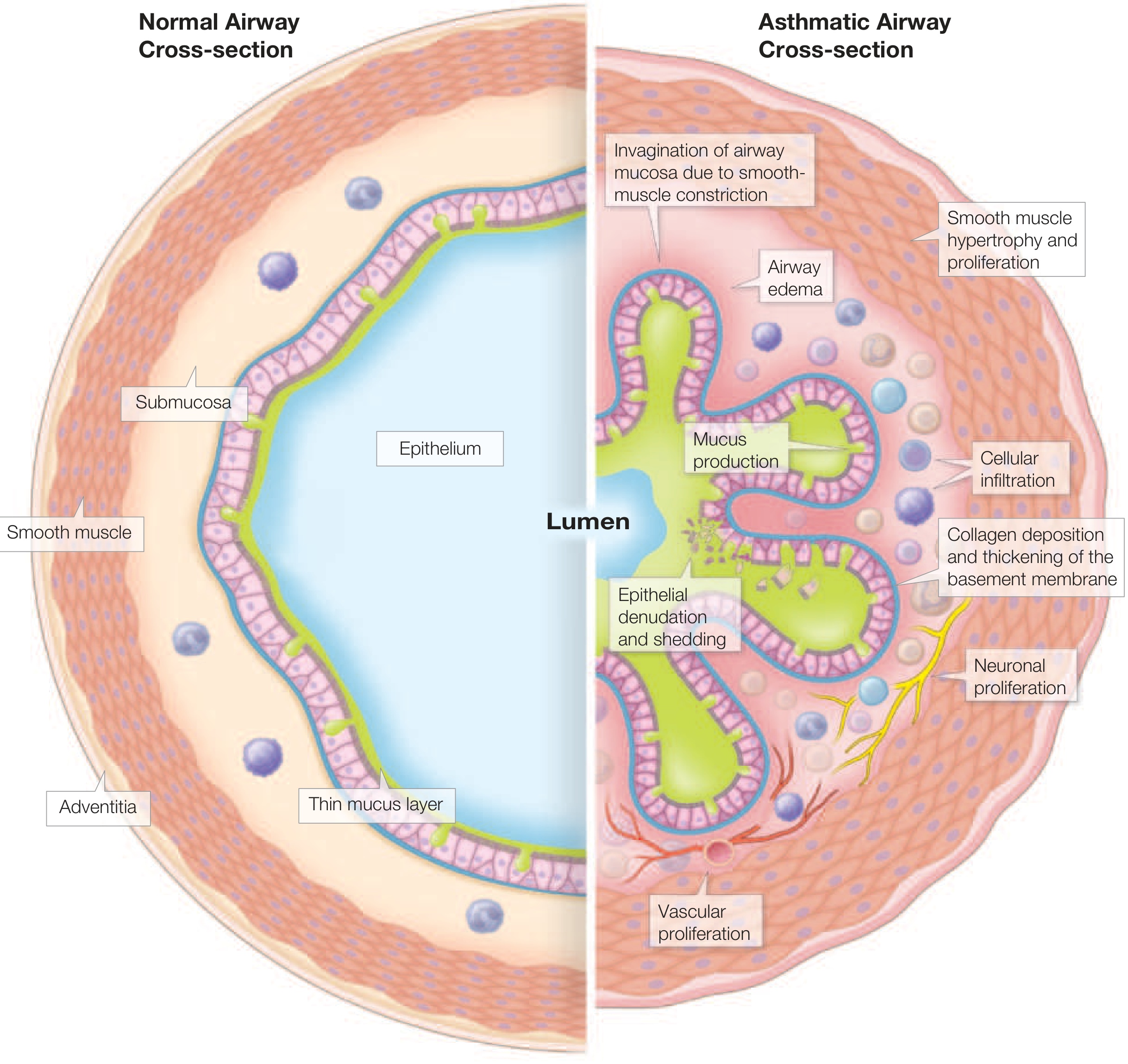
Structural/Remodeling Changes
- Epithelial fragility, mucosal edema and hyperemia
- Subepithelial reticular basement membrane thickening (collagen types III and IV)
- In chronic/severe disease: smooth muscle hyperplasia, mucus gland hypertrophy, subepithelial angiogenesis
Triggers
Allergens (house dust mite, animal dander, cockroach, pollen, mold), viral infections, exercise, cold/dry air, irritants, pollutants, ASA/NSAIDs, β-blockers, occupational exposures, hormonal changes
3. Non-Atopic (Intrinsic) Asthma
Definition
- No demonstrable IgE-mediated sensitization to environmental allergens
- Also called "intrinsic" asthma (historically also "cryptogenic")
- Often adult-onset, can be more severe and persistent
- Both atopic and intrinsic asthma are classified as "Type-2-high" phenotypes — meaning eosinophilic inflammation driven by type-2 cytokines is still present, but without the IgE allergic mechanism
Key Differences from Atopic Asthma
| Feature | Atopic | Non-Atopic (Intrinsic) |
|---|---|---|
| Onset | Often childhood | Often adult onset |
| Skin prick test | Positive | Negative |
| Serum total/specific IgE | Elevated | Normal |
| Blood eosinophilia | Common | May still be present |
| Triggers | Allergens + others | Non-allergen triggers (infections, exercise, cold air, aspirin) |
| Family history of atopy | Often present | Less common |
| Response to allergen avoidance | Yes | No |
| Response to ICS | Good | Good (if eosinophilic) |
Cluster analyses of large adult asthma cohorts have identified at least three subtypes that are not well described by the atopic/non-atopic binary. — Goldman-Cecil Medicine
4. Additional Recognized Phenotypes / Endotypes
- Eosinophilic asthma (Type-2-high): responds well to ICS and anti-IL-5/anti-IL-4Rα biologics; can be atopic or non-atopic
- Neutrophilic asthma (Type-2-low): more severe, steroid-resistant; associated with obesity, smoking, occupational exposures
- Mixed eosinophilic/neutrophilic: most severe phenotype
- Exercise-induced bronchoconstriction
- Aspirin-exacerbated respiratory disease (AERD)
- Occupational asthma
5. Diagnosis
Diagnosis is based on compatible symptoms + objective evidence of variable airflow obstruction.
Clinical Features
- Episodic wheeze, dyspnea, chest tightness, cough (especially nocturnal)
- Symptoms vary over time and in intensity
- Triggered by allergens, exercise, viral infections, irritants
Spirometry (Essential)
- FEV1/FVC <0.7 (or below lower limit of normal) = obstruction
- Bronchodilator reversibility: ≥12% AND ≥200 mL increase in FEV1 after SABA → strongly supports asthma
- If spirometry is normal between attacks, further testing is needed
Bronchoprovocation Testing
Used when spirometry is normal or near-normal:
- PC20 (methacholine or histamine provocative concentration causing 20% fall in FEV1)
- PC20 ≤0.125 mg/mL = severe hyperresponsiveness (score 3)
- PC20 8–>0.5 mg/mL = mild hyperresponsiveness
- Exercise challenge or mannitol challenge can also be used
Peak Expiratory Flow (PEF)
- Serial PEF monitoring demonstrates variability >20% (diurnal or day-to-day)
- Useful for both diagnosis and monitoring control
Biomarkers Distinguishing Atopic from Non-Atopic / Endotyping
| Test | Atopic Asthma | Non-Atopic | Eosinophilic (either) |
|---|---|---|---|
| Skin prick test (SPT) | Positive | Negative | Variable |
| Serum total IgE | Elevated | Normal | Normal/elevated |
| Specific IgE (RAST) | Positive | Negative | Variable |
| Blood eosinophils | Elevated | May be elevated | Elevated (≥300/µL) |
| FeNO | Elevated (>35–40 ppb if untreated) | Variable | Elevated if IL-13 driven |
| Induced sputum eosinophils | Elevated | May be elevated | Elevated |
FeNO (Fraction of exhaled NO):
-
35–40 ppb in untreated patients = Type-2 (eosinophilic) inflammation
-
20–25 ppb despite moderate-to-high ICS = poor adherence or persistent Type-2 inflammation
- Easily suppressed by ICS, useful for adherence monitoring
Severity Classification (GINA-based)
| Severity | Symptom Frequency | Nighttime Symptoms | FEV1 (% predicted) | SABA Use |
|---|---|---|---|---|
| Intermittent | ≤2 days/week | ≤2×/month | ≥80% | ≤2 days/week |
| Mild persistent | >2 days/week but not daily | 3–4×/month | ≥80% | >2 days/week |
| Moderate persistent | Daily | >1×/week | 60–79% | Daily |
| Severe persistent | Continuous | Frequent | <60% | Continuous |
6. Management: International Protocol (GINA Stepwise Approach)
Goals of Therapy
- Symptom frequency ≤2 times/week
- Nighttime awakenings ≤2 times/month
- Reliever use ≤2 times/week (except before exercise)
- No more than 1 exacerbation/year
- Optimized lung function
- Normal daily activities
- Minimal treatment side effects
— Harrison's Principles of Internal Medicine, 22E
Non-Pharmacological Measures (All Types)
- Allergen mitigation (atopic): dust-mite impermeable covers as part of comprehensive strategy; pet removal if clearly symptomatic; pest control for cockroach-sensitized patients
- Remove or reduce occupational triggers
- Avoid secondhand smoke and cannabis combustion products
- Vaccination: annual influenza, pneumococcal (all adults regardless of age), COVID-19, RSV vaccines
- Allergen immunotherapy (subcutaneous): suitable only in mild-to-moderate controlled atopic asthma; variable evidence; risk of anaphylaxis
- Sublingual immunotherapy: evidence base not yet substantial for asthma
Pharmacological Agents
Reliever Medications (Rescue / Bronchodilators)
| Drug Class | Agent | Onset | Duration | Notes |
|---|---|---|---|---|
| SABA | Albuterol (salbutamol) | 3–5 min | 4–6 h | First-line reliever; MDI or nebulizer |
| LABA | Salmeterol, Formoterol | Salmeterol: slow; Formoterol: fast (~like SABA) | ~12 h | NOT monotherapy in asthma; always with ICS; formoterol used in MART strategy |
| SAMA | Ipratropium | 15–30 min | 4–6 h | Adjunct in severe acute exacerbations |
| LAMA | Tiotropium | Hours | 24 h | Add-on in Step 4–5 for uncontrolled asthma |
Frequent SABA use (without ICS) is associated with increased asthma mortality. — Harrison's 22E
Controller Medications
Inhaled Corticosteroids (ICS) — Cornerstone of therapy for all persistent asthma
| Agent | Low Dose | High Dose | Delivery |
|---|---|---|---|
| Beclomethasone | 1–2 puffs bid (low strength) | 5–6 puffs bid (high strength) | MDI/DPI |
| Budesonide | 1–2 puffs bid (100 µg) | 1–2 puffs bid (400 µg) | DPI/nebulizer |
| Ciclesonide | 1 puff (80 µg) bid | Max dose (400 µg DPI) | MDI |
| Fluticasone propionate | 1–2 puffs bid (50 µg) | 2 puffs bid (highest strength) | MDI/DPI |
| Fluticasone furoate | 1 puff daily (50 µg) | 1 puff daily (200 µg) | DPI |
| Mometasone | 1 puff daily (100 µg) | 2 puffs bid (200 µg) | MDI/DPI |
— Goldman-Cecil Medicine
Additional Controllers
| Drug | Mechanism | Use |
|---|---|---|
| Leukotriene receptor antagonists (LTRAs) — Montelukast, Zafirlukast | Block cysteinyl LT1 receptors | Step 2 alternative; aspirin-sensitive asthma; allergic rhinitis comorbidity |
| Theophylline | Bronchodilator (phosphodiesterase inhibitor) + mild anti-inflammatory | Step 3–4 add-on; narrow therapeutic window; falling out of use |
| Anti-IgE — Omalizumab | Binds free IgE → prevents mast cell/basophil activation | Step 5: moderate-to-severe atopic asthma with elevated IgE |
| Anti-IL-5 — Mepolizumab, Reslizumab | Reduce severe eosinophilic inflammation | Step 5: severe eosinophilic asthma |
| Anti-IL-4Rα — Dupilumab | Blocks IL-4/IL-13 signaling | Step 5: severe type-2 asthma (atopic or non-atopic eosinophilic) |
| Anti-TSLP — Tezepelumab | Blocks upstream alarmin | Step 5: broad severe asthma regardless of phenotype |
GINA Stepwise Treatment
STEP 1 — Intermittent Asthma
• PRN low-dose ICS-formoterol (preferred) OR
• PRN SABA alone (if truly infrequent, low risk)
STEP 2 — Mild Persistent
• Low-dose ICS (daily) + PRN SABA
• Alternative: LTRA daily + PRN SABA
STEP 3 — Moderate Persistent
• Low-dose ICS + LABA + PRN SABA or ICS-formoterol (MART)
• Alternative: Medium-dose ICS + PRN SABA
STEP 4 — Severe (Step-up)
• Medium/high-dose ICS + LABA + PRN ICS-formoterol (MART)
• Consider adding LAMA (tiotropium)
• Add LTRA or theophylline
• Consider specialist referral
STEP 5 — Severe Uncontrolled
• High-dose ICS + LABA
• Add LAMA
• Biologics based on phenotype:
– Elevated IgE + atopic → Omalizumab (anti-IgE)
– Eosinophilia (≥300/µL) → Mepolizumab or Reslizumab (anti-IL-5)
– Type-2 inflammation → Dupilumab (anti-IL-4Rα)
– Regardless of phenotype → Tezepelumab (anti-TSLP)
• Consider oral corticosteroids (lowest effective dose)
Specific Considerations by Asthma Type
| Consideration | Atopic | Non-Atopic |
|---|---|---|
| Allergen avoidance | Central | Not relevant |
| Allergen immunotherapy | Yes (mild–moderate, controlled) | No |
| Anti-IgE (Omalizumab) | Yes (if elevated IgE) | No |
| Anti-IL-5 biologics | Yes (if eosinophilic) | Yes (if eosinophilic) |
| Dupilumab | Yes | Yes (if Type-2 high) |
| Tezepelumab | Yes | Yes (broader applicability) |
| ICS | Yes | Yes |
Management of Acute Exacerbations
- Oxygen to maintain SpO2 94–98%
- Repeated SABA (albuterol) via MDI+spacer or nebulizer q20 min × 3 in first hour
- Ipratropium added in moderate-severe exacerbations
- Systemic corticosteroids — oral prednisolone 40–50 mg/day × 5–7 days (IV methylprednisolone if unable to take orally)
- Magnesium sulfate IV (2 g over 20 min) — severe exacerbations not responding to initial therapy
- Heliox, IV bronchodilators, or ICU intubation for life-threatening cases
Assessment of Asthma Control (Goals Achieved)
| Parameter | Controlled |
|---|---|
| Daytime symptoms | ≤2 days/week |
| Night awakenings | ≤2/month |
| SABA use | ≤2/week |
| Activity limitation | None |
| Exacerbations | ≤1/year |
If poorly controlled despite Step 4–5 therapy → evaluate for: poor inhaler technique, non-adherence, sinusitis, GERD, vocal cord dysfunction, obesity, obstructive sleep apnea, bronchiectasis, or α1-antitrypsin deficiency.
Sources:
- Harrison's Principles of Internal Medicine, 22E — Chapter 298: Asthma
- Goldman-Cecil Medicine, International Edition — Chapter 75: Asthma
- Murray & Nadel's Textbook of Respiratory Medicine — Chapter 35
- Goodman & Gilman's Pharmacological Basis of Therapeutics — Asthma and COPD Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.