chest pain with normal troponin but positive d-dimer what's the differential?
chest pain normal troponin elevated D-dimer differential diagnosis
Why this combination matters
Priority Diagnoses (must rule out urgently)
1. Pulmonary Embolism (PE) - the top concern
- Key features: pleuritic pain, dyspnea, tachycardia, hypoxia, low-grade fever, leg swelling/DVT
- Next step: apply Wells or Geneva score, PERC rule; proceed to CT pulmonary angiography if indicated
- Harrison's 22e, Chap. 290; Tintinalli's EM; Rosen's EM
2. Acute Aortic Dissection
- Key features: tearing/ripping pain radiating to the back, pulse/BP differential between arms, wide mediastinum on CXR, hypertension history, Marfan features
- The ADD-RS (Aortic Dissection Detection Risk Score) + D-dimer strategy: ADD-RS of 0 + negative D-dimer = 99.7% sensitivity. A positive D-dimer with any ADD-RS points mandates CT aortography.
- Rosen's EM, p. 1161; Fuster and Hurst's The Heart, 15th ed.
Important Secondary Diagnoses (D-dimer elevated but less immediately life-threatening)
3. Pericarditis
4. Pneumonia / Pleuritis
5. Pneumothorax
6. Esophageal Rupture (Boerhaave Syndrome)
Non-life-threatening causes of elevated D-dimer with chest pain
| Cause | Why D-dimer rises |
|---|---|
| Active malignancy | Chronic hypercoagulability, occult VTE |
| Recent surgery / trauma | Systemic coagulation activation |
| Pregnancy (2nd/3rd trimester) | Physiologic fibrin turnover - D-dimer unreliable |
| Sepsis | Disseminated intravascular coagulation (DIC) pathway activation |
| Atrial fibrillation | Intra-atrial thrombus and fibrin turnover |
| Heart failure | Low-flow state + chronic activation |
| COVID-19 | Marked endothelial/coagulation activation, elevated D-dimer independently associated with mortality |
| Advanced age (>70) | Age-adjusted cutoff applies: age x 10 ng/mL |
| Liver disease | Impaired fibrin clearance |
| Inflammatory conditions (SLE, vasculitis) | Active inflammation |
| Musculoskeletal / costochondritis | D-dimer itself is nonspecific here - likely coincidental or minor elevation |
Clinical Approach Summary
Chest pain + Normal Troponin + Positive D-dimer
|
v
Apply clinical probability scores
(Wells for PE, ADD-RS for dissection)
|
Low probability PE + PERC-negative? --> No further workup needed
Low-intermediate probability PE? --> D-dimer effectively rules out
High probability PE? --> CT pulmonary angiography (D-dimer is not enough)
Any suspicion for dissection? --> CT aortography (do NOT anticoagulate first)
ECG: diffuse ST-elev + PR dep? --> Pericarditis workup
CXR: infiltrate/effusion? --> Pneumonia, effusion, esophageal rupture
Create a quick reference card for D-dimer interpretation
A clean, professional medical quick reference card titled "D-Dimer Interpretation" for emergency medicine clinicians. Dark navy blue header with white title text. Organized into clearly labeled sections with colored boxes: Section 1 - "What is D-Dimer?" with a brief description: fibrin degradation product, reflects active clot formation and lysis. Sensitivity >95% for PE/DVT, specificity ~50%. Section 2 - "Normal Cutoffs" with a table: Standard cutoff: <500 ng/mL (or <0.5 mg/L FEU). Age-adjusted (age >50): Age × 10 ng/mL (e.g., 70yo = <700 ng/mL). YEARS algorithm: <1000 ng/mL if no YEARS criteria met. Section 3 - "Positive D-Dimer: Key Diagnoses" with colored icons and two columns: LIFE-THREATENING (red): Pulmonary Embolism, Aortic Dissection, DIC, Massive DVT; OTHER CAUSES (orange): Pneumonia/sepsis, Malignancy, Post-surgery/trauma, Pregnancy, Atrial fibrillation, Heart failure, COVID-19, Liver disease, Inflammatory conditions, Advanced age. Section 4 - "Rule-Out Algorithm" flowchart: Low pretest probability (Wells <2 or Geneva low) → D-dimer → Negative = PE excluded. Positive = CT-PA. High pretest probability → Skip D-dimer → CT-PA directly. Aortic dissection: ADD-RS 0 + Negative D-dimer = 99.7% sensitivity. Section 5 - "Key Pitfalls" in a yellow warning box: Only ~30% of positive D-dimers have PE. Never use as rule-IN test. Do NOT anticoagulate before ruling out dissection. D-dimer unreliable in late pregnancy and post-op patients. Normal troponin does NOT rule out dissection. Section 6 - small footer: "Sources: Harrison's 22e, Rosen's EM, Tintinalli's EM" Clean white background, color-coded sections, medical sans-serif font, compact card format suitable for a pocket reference or laminated card.
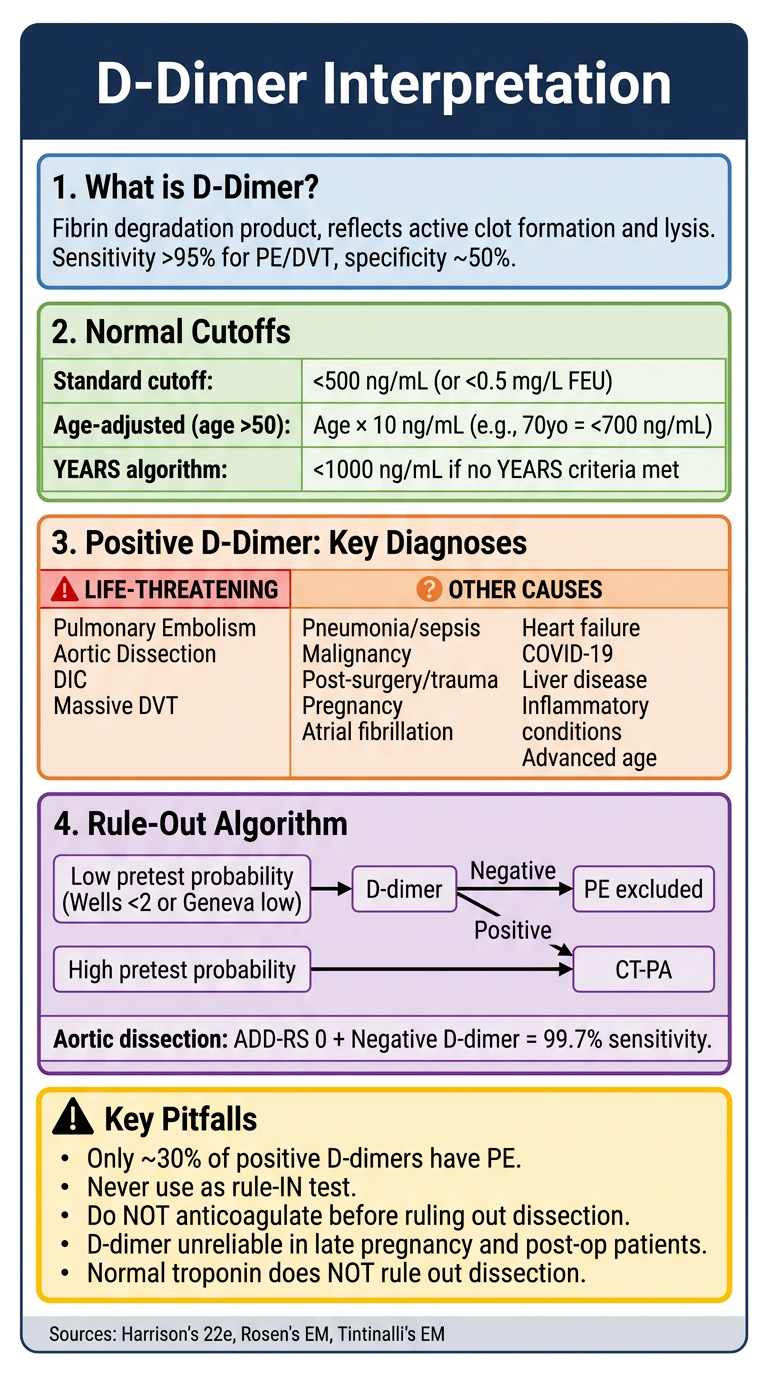
- Normal cutoffs including the age-adjusted formula (age x 10 ng/mL) and the YEARS algorithm threshold
- Life-threatening vs. other causes of a positive result, color-coded for fast scanning
- Rule-out algorithm for PE and aortic dissection with decision branch logic
- Key pitfalls in a warning box - the ones that cause real harm if missed
Search for latest 2024-2026 guidelines on PE risk stratification
"pulmonary embolism" AND "risk stratification"
pulmonary embolism risk stratification guidelines 2024 2025 ESC AHA update
PMID: 41712677
PMID: 40200307
https://www.pharmacytimes.com/view/aha-acc-guidelines-introd…
https://emcrit.org/pulmcrit/peguidelines
"pulmonary embolism" AND "YEARS algorithm" AND "D-dimer"
2026 AHA/ACC PE Guidelines: What's New
- Full guideline in Circulation [PMID: 41712677]
The Biggest Change: A New 5-Category Risk Classification
| Category | Description | Rough Old Equivalent |
|---|---|---|
| A | Subclinical / incidentally found PE (on CT done for another reason, no symptoms) | - |
| B | Symptomatic, low severity - PESI ≤85, sPESI <1, Hestia <1 | Low-risk |
| C | Symptomatic, higher severity by validated score + RV dysfunction | Intermediate (submassive) |
| D | Pre-cardiopulmonary failure - normotensive shock, possible need for ventilatory support | Intermediate-high |
| E | Cardiopulmonary failure - persistent/recurrent hypotension, cardiogenic shock, cardiac arrest | Massive / high-risk |
Key Recommendation Changes
Diagnosis & D-Dimer
- D-dimer remains central to ruling out PE in low-pretest probability patients, balancing "potential harms of testing with the risk of missed diagnosis"
- Age-adjusted D-dimer (age × 10 ng/mL for >50 years) and the YEARS algorithm (D-dimer threshold 1000 ng/mL if no YEARS criteria met) both endorsed
- New: Every patient must have a CT-PA to enter Categories B-E subgroups - which has been criticized as removing the option of ruling in PE via limb ultrasound alone
Biomarkers for Risk Stratification
- Strong recommendation (LOE B-NR): Measure at least 1 cardiac biomarker (troponin or BNP) in Category C patients (symptomatic, no shock) to assess short-term risk
- Strong recommendation (LOE B-NR): Measure lactate in Categories C-E patients at an acute care facility to further stratify mortality risk - this is a new emphasis
Treatment Setting
- More aggressive push for outpatient management of Category B (low-risk) PE when social/clinical criteria are met (Hestia criteria endorsed)
- Category A (incidental PE): individualized anticoagulation decision - not automatic treatment
Anticoagulation
- DOACs over VKAs (warfarin) for eligible patients: strong recommendation
- Apixaban and rivaroxaban are the preferred DOACs (most evidence)
PERT (PE Response Teams)
- New strong recommendation to implement PERTs at acute care facilities when resources permit
- PERTs shown to reduce hospital length of stay and improve decision-making for advanced therapies (catheter-directed thrombolysis, mechanical thrombectomy)
Score Comparison: What the Evidence Now Says
| Score | Rule-out (LR-) | Verdict |
|---|---|---|
| 3-tier Revised Geneva | 0.39 | Best overall - objective, no subjective "PE most likely" item |
| 3-tier Wells | 0.34 | Similar rule-out, slightly worse for imaging triage |
| 2-tier Wells | 0.56 | Significantly underperforms - should not be used |
| PERC | 0.36 | Reliable rule-out when applied correctly, but wide CIs - more evidence needed |
Expert Criticism of the 2026 Guidelines (EMCrit/PulmCrit analysis)
-
PESI blind spot not patched: The ESC 2019 guidelines required low-risk patients to have both a low sPESI and no RV dilation. The 2026 AHA/ACC guidelines omit this requirement, risking misclassification of genuinely sick patients into Category B (undertreated)
-
Troponin vs. BNP conflated: The guideline treats them as equivalent "biomarkers," but troponin is more specific for adverse outcomes. Patients with chronic heart failure (elevated BNP, normal troponin) may be falsely triaged to a higher-risk category
-
Three competing severity scores allowed: The guideline endorses PESI, sPESI, or Bova to define Category C - using different scores in practice will produce contradictory classifications between providers
-
CT-PA required for all: Requiring CT-PA even in Category B subcategorization removes the option of diagnosing PE via compression ultrasound alone (the ESC 2019 approach), leading to more contrast and radiation exposure in otherwise low-risk patients
How This Compares to ESC 2019 (still in use in Europe)
| Feature | ESC 2019 | AHA/ACC 2026 |
|---|---|---|
| Risk tiers | 3 (low / intermediate / high) | 5 (A-E) |
| Low-risk criteria | sPESI=0 + no RV dilation | sPESI <1 alone (Category B) |
| Biomarkers | Troponin + BNP separately weighted | Grouped as "biomarkers" |
| PERT | Mentioned | Strong recommendation |
| Outpatient PE | Endorsed with Hestia | More explicitly endorsed |
| Score preference | Wells or Geneva (no preference) | PESI/sPESI/Bova (no preference) |
Bottom Line for Practice
- The 2026 AHA/ACC guideline is the current US standard for acute PE management
- The new A-E categories add nuance at both ends (incidental PE and refractory shock) but the intermediate categories remain contested
- Use 3-tier Revised Geneva or 3-tier Wells for pretest probability (per the 2025 meta-analysis)
- DOACs first, measure troponin + lactate in intermediate/high-risk patients
- Push for outpatient treatment in Category B when Hestia criteria are met
- If your institution doesn't have a PERT yet, the 2026 guideline makes it a formal quality benchmark
give me a proper treatment plan