Tell me the Management approach to a patient of hypotension for a MBBS graduate general practitioner working in emergency
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypotension" AND "emergency management" AND "fluid resuscitation"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive, authoritative content from Rosen's Emergency Medicine. I have everything needed to write an excellent, structured management guide for a GP in the emergency setting. Let me compile this into a comprehensive response.
Management of Hypotension in the Emergency Setting
For an MBBS Graduate General Practitioner
(Based primarily on Rosen's Emergency Medicine, 9th Edition, Chapter 3 - Shock)
1. Definitions & Key Concepts
Hypotension = Systolic BP < 90 mmHg, or MAP < 65 mmHg, or a drop of >40 mmHg from baseline.
Critical distinction: Shock ≠ Hypotension. Shock is inadequate tissue perfusion. A patient can be in shock with a normal BP (compensated), and not all hypotensive patients are in shock. Your job is to manage the underlying state, not just the number.
Shock diagnostic criteria (any 2 of these = presumptive shock):
- Arterial base deficit < -4 mEq/L
- Serum lactate > 4 mmol/L
- Urine output < 0.5 mL/kg/h
- Sustained arterial hypotension > 30 minutes
2. The ABCDE Stabilization (Do This Immediately, in Parallel)
| Step | Action |
|---|---|
| A - Airway | Ensure patent airway; prepare for intubation if GCS < 8 or respiratory failure |
| B - Breathing | Apply high-flow O₂ (15 L/min via non-rebreather mask); target SpO₂ > 94% |
| C - Circulation | Two large-bore IV lines (16G or larger) in antecubital fossa; send bloods simultaneously |
| D - Disability | Assess GCS, blood glucose (rule out hypoglycemia as a cause/contributor) |
| E - Exposure | Full body examination; look for bleeding sources, rashes, distended abdomen |
3. Immediate Investigations (Order All Simultaneously)
- CBC - hemoglobin (hemorrhage/anemia), WBC (infection/sepsis), platelets
- Serum electrolytes, BUN, creatinine - renal perfusion
- Blood glucose - hypoglycemia
- Arterial Blood Gas (ABG) - base deficit, lactate, PaO₂/FiO₂
- Serum lactate - key perfusion marker; > 4 mmol/L = shock
- LFTs, coagulation profile (PT/INR/aPTT)
- ECG - ischemia, arrhythmia, right heart strain (PE)
- Urinalysis + Foley catheter insertion - monitor urine output
- CXR - pulmonary edema, pneumothorax, widened mediastinum
- Bedside ultrasound (POCUS/FAST) if available - cardiac tamponade, hemoperitoneum, LV function, IVC collapsibility
4. Diagnose the TYPE of Shock (This Drives All Management)
Use the clinical flowchart approach from Rosen's EM (see diagram below):
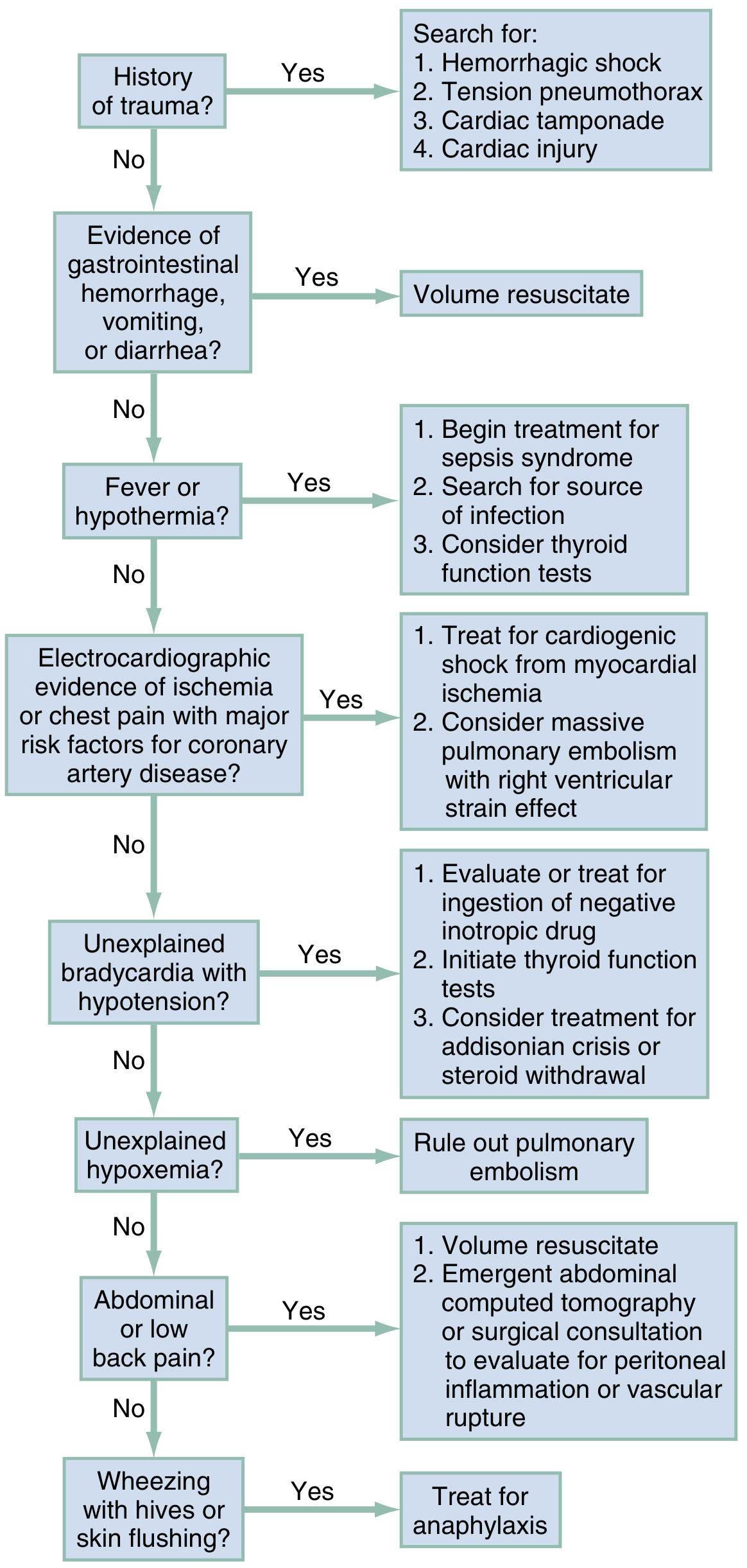
The 4 (+1) Types of Shock:
| Type | Mechanism | Classic Signs | Common Causes |
|---|---|---|---|
| Hypovolemic | Low preload (volume loss) | Tachycardia, dry mucosa, flat neck veins, cold extremities | Hemorrhage, dehydration, burns, GI losses |
| Distributive | Loss of vascular tone / maldistribution | Warm flushed skin, bounding pulse early; then cold in late stages | Sepsis, anaphylaxis, neurogenic, adrenal crisis |
| Cardiogenic | Pump failure | JVD, pulmonary edema, S3 gallop, cold clammy extremities | MI, arrhythmia, myocarditis, tension pneumothorax (obstructive) |
| Obstructive | Outflow obstruction | JVD, hypoxia, unilateral absent breath sounds or muffled heart sounds | Cardiac tamponade, massive PE, tension pneumothorax |
| Neurogenic | Sympathetic loss | Bradycardia with hypotension (no reflex tachycardia) | Spinal cord injury |
5. Type-Specific Management (from Rosen's EM, Box 3.5)
A. Hypovolemic / Hemorrhagic Shock
- Control hemorrhage: direct pressure, tourniquet, splint long-bone fractures
- IV fluids: 10-20 mL/kg isotonic crystalloid (Normal Saline or Ringer's Lactate) as initial bolus; reassess
- If massive hemorrhage suspected (trauma): skip crystalloid; go directly to packed RBCs (5-10 mL/kg) in a balanced ratio with fresh frozen plasma (FFP) and platelets (1:1:1)
- Transfuse PRBCs if hemoglobin < 7 g/dL (or < 10 g/dL if active cardiac ischemia)
- Urgent surgical/gastroenterology referral for uncontrolled internal bleeding
B. Septic Shock (Distributive)
- Fluids: 30 mL/kg crystalloid IV within the first hour; reassess after each 500 mL bolus for response vs. fluid overload
- Vasopressors (if volume fails to restore MAP > 65): Norepinephrine is the first-line agent, starting at 0.5 mcg/min IV infusion (titrate to MAP > 65)
- Antibiotics: Broad-spectrum IV antibiotics within 1 hour of recognition (e.g., Piperacillin-Tazobactam + Vancomycin empirically, pending cultures)
- Blood cultures x2 (aerobic + anaerobic) BEFORE antibiotics if possible, but do NOT delay antibiotics > 1 hour
- Source control: drain abscess, remove infected catheter
- PRBCs if Hb < 7 g/dL
- Consider hydrocortisone 200 mg/day IV if vasopressor-refractory septic shock
C. Cardiogenic Shock
- Oxygen + CPAP/NIPPV for pulmonary edema (reduce work of breathing)
- Do NOT give large fluid boluses (will worsen pulmonary edema)
- Vasopressors/inotropes: Norepinephrine 0.5 mcg/min IV + Dobutamine 5 mcg/kg/min IV (combined vasopressor and inotrope approach)
- Treat the underlying cause:
- STEMI → Aspirin + Heparin + emergent PCI (or thrombolysis if PCI unavailable)
- Arrhythmia → Cardioversion or rate control
- Acute MR/VSD → surgical referral
- Avoid negative inotropes (beta-blockers, CCBs)
- Urgent cardiology/higher center referral
D. Obstructive Shock
- Cardiac tamponade: Immediate pericardiocentesis (life-saving procedure)
- Tension pneumothorax: Immediate needle decompression (2nd intercostal space, midclavicular line) → chest tube insertion
- Massive PE: Systemic thrombolysis (Alteplase 100 mg IV over 2h) if hemodynamically unstable; anticoagulation with heparin
E. Anaphylactic Shock (Distributive - special case)
- IM Epinephrine 0.3-0.5 mg (1:1000) immediately - this is the single most important step
- IV fluids (1-2L crystalloid bolus)
- IV antihistamines (chlorpheniramine), IV corticosteroids (hydrocortisone 200 mg)
- Nebulized bronchodilators for bronchospasm
- Keep supine with legs elevated
F. Neurogenic Shock (Spinal cord injury)
- Bradycardia with hypotension: IV fluids first, then Norepinephrine or Phenylephrine
- Do NOT use epinephrine (worsens bradycardia via reflex)
- Atropine if heart rate < 50 and symptomatic
- Urgent neurosurgical referral
6. Vasopressor Quick Reference
| Drug | Starting Dose | Indication |
|---|---|---|
| Norepinephrine | 0.5-2 mcg/min IV (up to 30 mcg/min) | First-line for septic, cardiogenic, and most distributive shock |
| Epinephrine | 0.3-0.5 mg IM (anaphylaxis); 0.1-1 mcg/min IV infusion | Anaphylaxis; refractory shock |
| Dopamine | 5-20 mcg/kg/min IV | Second-line (more arrhythmogenic than NE) |
| Dobutamine | 2.5-10 mcg/kg/min IV | Cardiogenic shock (inotrope, not vasopressor) |
| Vasopressin | 0.03-0.04 units/min IV | Adjunct in septic shock refractory to NE |
All vasopressors should ideally be given via central line. In an emergency, a proximal peripheral or IO (intraosseous) line is acceptable short-term.
7. Monitoring Response to Treatment
A patient is responding adequately if you see:
- HR decreasing toward normal (< 100)
- SBP > 90 or MAP > 65 mmHg
- Urine output improving to > 0.5 mL/kg/h (target 1 mL/kg/h)
- Serum lactate trending down (clear within 2-4h)
- Base deficit improving (less negative)
- Improving mental status
Signs of worsening / need for escalation:
- Rising lactate despite resuscitation
- Refractory hypotension despite 3+ L fluids
- Worsening base deficit
- New or worsening organ dysfunction (oliguria, confusion, rising creatinine)
8. When to Refer / Transfer to a Higher Center
As a GP in an emergency, refer/transfer when:
- STEMI or cardiogenic shock (PCI center needed)
- Surgical emergency (hemorrhage, bowel perforation, AAA)
- Refractory shock not responding to initial management
- Requirement for ICU-level vasopressor infusions
- Massive PE needing thrombectomy or ECMO
- Cardiac tamponade needing surgical drainage
9. Common Pitfalls to Avoid
| Pitfall | Correction |
|---|---|
| Treating the BP number without finding the cause | Always identify the type of shock |
| Giving large fluids to cardiogenic shock | Small bolus (250 mL), reassess with lung exam |
| Delaying antibiotics in sepsis "waiting for cultures" | Cultures first, but antibiotics within 1 hour no matter what |
| Missing anaphylaxis (not giving epinephrine first) | Epinephrine IM is the most important drug in anaphylaxis |
| Missing tension pneumothorax (waiting for CXR) | This is a clinical diagnosis - needle decompress if suspected |
| Normal BP = no shock | Check lactate; compensated shock can exist with normal BP |
Sources: Rosen's Emergency Medicine: Concepts and Clinical Practice, 9th Ed., Chapter 3 (Shock) - Puskarich & Jones; Sabiston Textbook of Surgery, 21st Ed.; Goldman-Cecil Medicine, International Ed.
This is a shared conversation. Sign in to Orris to start your own chat.