oNH evaluation
optic nerve head ONH evaluation clinical assessment ophthalmology
optic nerve head evaluation cup disc ratio neuroretinal rim
optic nerve head evaluation glaucoma
Optic Nerve Head (ONH) Evaluation
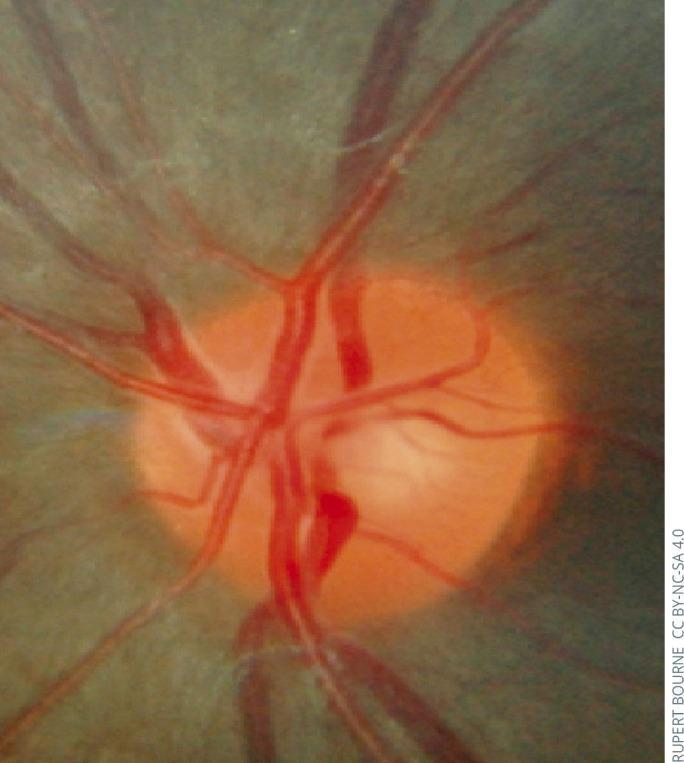
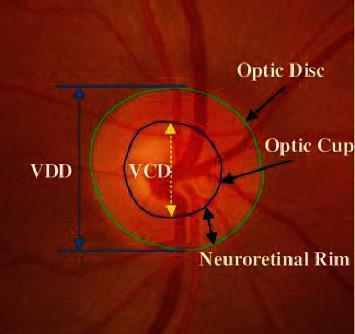
1. Normal ONH Anatomy
| Structure | Description |
|---|---|
| Neuroretinal Rim (NRR) | Orange-pink tissue between the cup edge and disc margin |
| Optic Cup | Central pale depression within the disc |
| Optic Disc | The visible head of the optic nerve |
| Peripapillary Retina | Surrounding tissue that may show atrophic changes |
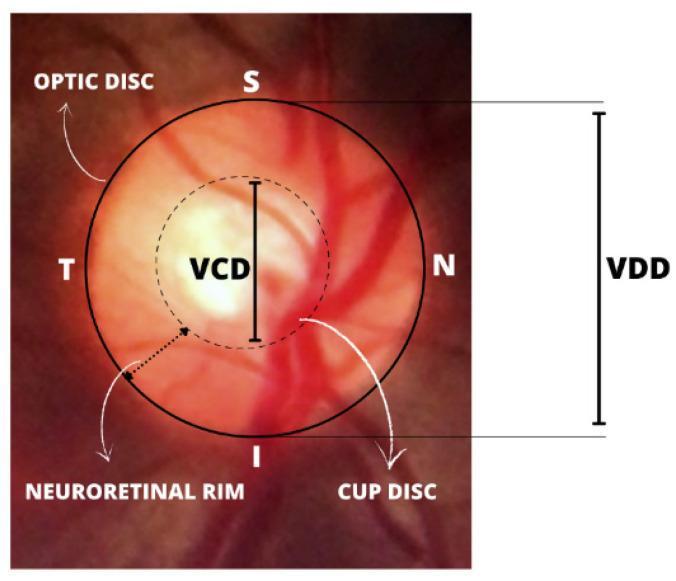
2. The ISNT Rule
Inferior > Superior > Nasal > Temporal
- Sensitivity for glaucoma: 81%, but low specificity (32%)
- Eyes without glaucoma often do not respect this rule
- A 2026 meta-analysis (PMID: 41212675) is the most recent evidence on ISNT rule diagnostic accuracy
3. Cup/Disc (C/D) Ratio
- Vertical C/D ratio is preferred over horizontal
- Only 2% of the population has a C/D ratio >0.7
- Asymmetry ≥0.2 between eyes raises suspicion for glaucoma — but always exclude a genuine difference in disc size first
- Small discs → small cups (may be normal); Large discs → large cups (may also be normal)
💡 Tip: Any cupping in a small disc may be pathological; a large disc with a large cup may be entirely healthy.
4. Optic Disc Size
- Measured by vertical diameter; normal median: 1.5–1.7 mm (white population)
- Large discs may be more susceptible to IOP-induced lamina cribrosa displacement (relevant in normal tension glaucoma, NTG)
- Disc size varies by racial group — largest in those of African descent
- Measured clinically using a slit beam + correction factor (Table 11.3 in Kanski)
5. Glaucomatous Changes at the ONH
Structural signs of glaucomatous damage:
| Sign | Description |
|---|---|
| NRR notching | Focal loss, most often inferior or superior |
| Cup enlargement | Concentric or polar |
| Disc haemorrhage | Risk factor for development and progression; requires magnification to detect |
| Baring of circumlinear vessels | Space between NRR and superficial vessel → early NRR thinning |
| Bayoneting | Double angulation of vessels due to NRR loss |
| Laminar dot sign | Exposed lamina cribrosa fenestrations in advancing glaucoma |
| Sharpened rim/edge | Sharper disc margin angle as NRR recedes |
| Loss of nasal NRR | Sign of moderately advanced damage |
| Collateral vessels | Uncommon; caused by chronic low-grade circulatory obstruction |
Classic glaucomatous subtypes (Fig. 11.9):
- Focal ischaemic — inferior notch
- Myopic — temporal crescent + inferior NRR loss
- Sclerotic — superior shelving, inferior notching
- Concentrically enlarged — deep, uniform cup enlargement
6. Peripapillary Atrophy (PPA)
- Alpha zone (outer): Superficial RPE changes; larger/more common in glaucomatous eyes
- Beta zone (inner): Chorioretinal atrophy; larger, more common in glaucoma; risk factor for progression; its location predicts the orientation of visual field loss
7. Retinal Nerve Fibre Layer (RNFL)
- Arcuate fibres (superotemporal and inferotemporal) are most vulnerable to glaucomatous damage
- Papillomacular bundle fibres are most resistant
- RNFL defects (wedge-shaped or diffuse) precede detectable disc and visual field changes
- Assessed using:
- Red-free (green) light on slit lamp / fundus photography
- OCT (optical coherence tomography)
- Scanning laser polarimetry
⚠️ RNFL defects are not specific to glaucoma — they can occur in neurological disease and in apparently normal individuals.
Key Images
Recent Evidence Update
- PMID 41212675 (Eur J Ophthalmol, 2026): Systematic review/meta-analysis on ISNT rule — most current evidence on its diagnostic accuracy for glaucoma
- PMID 39392516 (Int Ophthalmol, 2024): Comprehensive review of ONH/RNFL imaging modalities in high myopia with glaucoma
Trabecu
trabeculectomy surgical procedure steps indications complications ophthalmology
trabeculectomy outcomes complications glaucoma
trabeculectomy surgical technique scleral flap bleb glaucoma
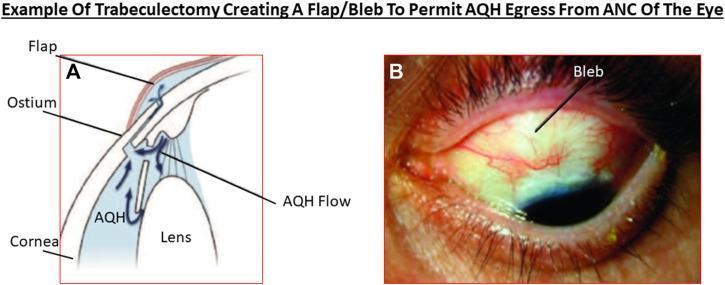
Trabeculectomy
Indications
- Failure of conservative (medical) therapy to achieve adequate IOP control
- Progressive deterioration despite seemingly adequate IOP control (including poor adherence)
- Primary therapy in advanced disease requiring very low target pressure — early surgery may give superior long-term outcomes, particularly in younger patients
- Patient preference — desire to be free of chronic medication
Surgical Technique (Classical Procedure)
| Step | Detail |
|---|---|
| Preoperative | Pupil constricted with pilocarpine 2% |
| Bridle suture | Inserted at superior cornea or superior rectus |
| Conjunctival flap | Limbal or fornix-based flap fashioned superiorly (12 o'clock incision to reduce bleb dysaesthesia) |
| Episcleral prep | Episcleral tissue cleared, major vessels cauterized |
| Scleral trapdoor | Lamellar scleral flap (50% depth) created — rectangular 3×3–4 mm, trapezoidal, or triangular |
| Flap dissection | Dissected anteriorly into clear cornea |
| Paracentesis | Made in temporal peripheral clear cornea |
| AC entry | Along most of the trapdoor base width |
| Sclerectomy | Block of deep sclera excised, usually with a Kelly punch |
| Peripheral iridectomy | Created to prevent blockage of the internal sclerostomy (may be omitted in pseudophakic eyes, with caution) |
| Flap suturing | Posterior corners sutured — releasable or lysable sutures to control postoperative leakage |
| AC reformation | BSS injected through paracentesis to test fistula patency |
| Conjunctival closure | Sutured; irrigation repeated to produce a bleb, checked for leakage |
| Postoperative drops | Atropine 1%; steroids + antibiotics 4×/day for 2 weeks, then steroids alone for 8–12 weeks |

Ex-Press Mini-Shunt
Antimetabolites in Filtration Surgery
Risk Factors for Surgical Failure:
- Previous failed trabeculectomy or MIGS
- Previous conjunctival or cataract surgery
- Secondary glaucoma (inflammatory, neovascular, post-traumatic)
- Black race, age <65 years
- Topical medication >3 years (especially sympathomimetics)
5-Fluorouracil (5-FU)
- Inhibits fibroblast proliferation by retarding DNA synthesis
- Intraoperative: sponge soaked in 50 mg/ml applied under Tenon flap for 5 minutes
- Postoperative: subconjunctival injection of 25–50 mg/ml solution
- Complications: persistent corneal epithelial defects, bleb leakage
Mitomycin C (MMC)
- Alkylating agent — more potent than 5-FU
- Typical: 0.2 mg/ml for 2 minutes intraoperatively; up to 0.4 mg/ml for high-risk patients
- Sponges placed away from the limbus to improve bleb profile
- Risk: cystic thin-walled bleb → chronic hypotony, late bleb leak, endophthalmitis
Bevacizumab (anti-VEGF)
- More effective than placebo, but increases risk of bleb encapsulation
- Not superior to MMC alone; combining with MMC shows no benefit
Complications
1. Shallow Anterior Chamber
| Cause | Management |
|---|---|
| Pupillary block | Mydriatics; Nd:YAG laser iridectomy |
| Overfiltration | Conservative; pressure dressing; AC reformation; suture tightening |
| Malignant glaucoma | Mydriatics + IV mannitol → Nd:YAG anterior hyaloid disruption → pars plana vitrectomy |
2. Failure of Filtration
- Flat, avascular bleb
- Vascularized bleb — episcleral fibrosis
- Encapsulated bleb (Tenon cyst) — localized, dome-shaped, fluid-filled, engorged vessels
- Extrascleral: Subconjunctival/episcleral fibrosis; bleb encapsulation
- Scleral: Over-tight flap suturing; scleral bed scarring
- Intraocular: Sclerostomy blockage (vitreous, blood, uveal tissue, membranes)
3. Bleb-Associated Infection
| Condition | Description |
|---|---|
| Blebitis | Infection without vitreous involvement |
| Endophthalmitis | Infection with vitreous involvement |
- Conjunctival swab (do NOT aspirate from within bleb)
- Topical broad-spectrum antibiotics hourly (e.g. ofloxacin + cephalosporin)
- Oral co-amoxiclav 500/125 mg TDS + ciprofloxacin 750 mg BD for ≥5 days (or azithromycin 500 mg/day)
- Steroids only after definite antibiotic response
4. Late Bleb Leakage
- Positive Seidel test confirms aqueous leak through bleb
- Risks: thin-walled or MMC blebs
- Management: pressure dressing, bandage contact lens, surgical revision, or bleb needling with 5-FU
5. Bleb Dysaesthesia
- Discomfort from a large or anteriorly placed bleb contacting the lid
- Reduced by placing incisions at 12 o'clock
Recent Evidence
- PMID 39394492 (Graefe's, 2025): Meta-analysis — PreserFlo MicroShunt vs. trabeculectomy: comparable IOP reduction with a different complication profile
- PMID 39670502 (Dtsch Arztebl Int, 2025): MIGS vs. trabeculectomy — trabeculectomy remains the gold standard for advanced glaucoma
Techniques of trabeculectomy
trabeculectomy surgical steps scleral flap conjunctival flap iridectomy technique
trabeculectomy surgical technique steps releasable sutures fornix limbal based flap
Technique of Trabeculectomy
Numerous modifications are in use. The classical procedure is described below.
Principle
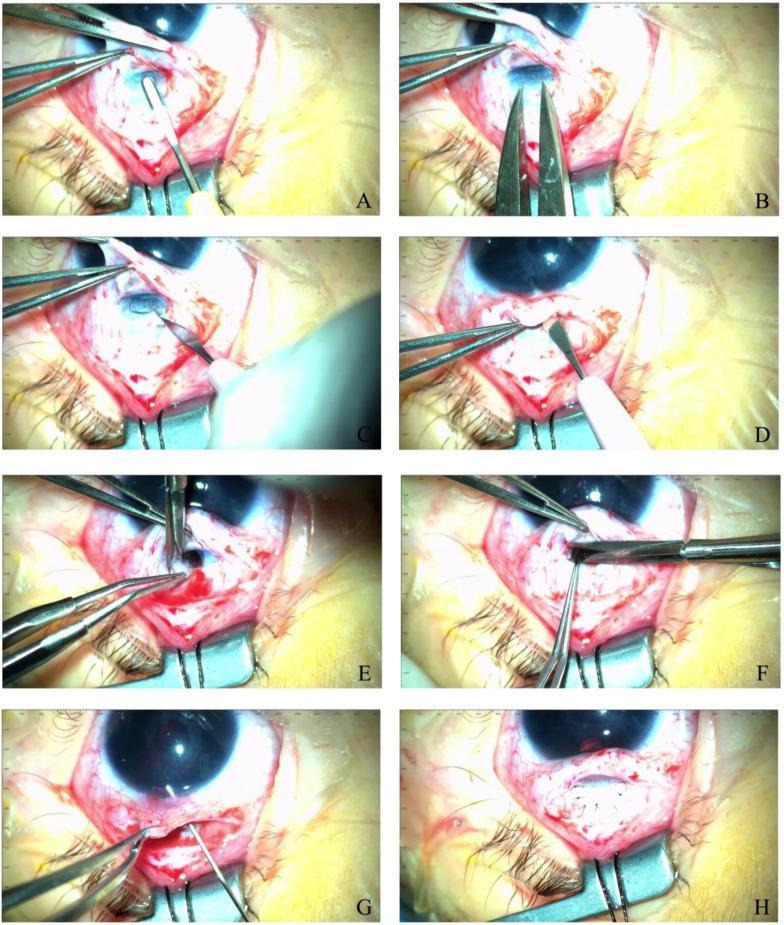
Step-by-Step Surgical Technique
Step 1 — Preoperative Preparation
- Pupil constriction: Pilocarpine 2% instilled preoperatively
- Deepens anterior chamber, protects the lens, and tents the iris away from the sclerostomy
Step 2 — Bridle Suture
- Inserted at superior cornea or superior rectus muscle
- Rotates the eye downward to expose the superior limbus
Step 3 — Conjunctival Flap
| Type | Description | Advantage |
|---|---|---|
| Limbal-based | Base at limbus, opening posteriorly | Better control of bleb position |
| Fornix-based | Base at fornix, opening anteriorly | Easier dissection; may produce a more diffuse bleb |
- Both include the conjunctiva + Tenon capsule
- Fashioned superiorly at 12 o'clock (reduces risk of bleb dysaesthesia compared to off-centre incisions)
Step 4 — Episcleral Preparation
- Episcleral tissue cleared
- Major vessels cauterized to minimize intraoperative bleeding
Step 5 — Lamellar Scleral Flap (Trapdoor)
- Incisions made through ~50% of scleral thickness
- Creates a trapdoor/lamellar flap — shapes available:
- Rectangular 3 × 3–4 mm (most common)
- Trapezoidal
- Triangular
- Flap dissected anteriorly until clear cornea is reached
Step 6 — Paracentesis
- Made in temporal peripheral clear cornea
- Allows AC reformation and IOP testing at any point during surgery
- Also used postoperatively for laser suture lysis or AC reformation if needed
Step 7 — Anterior Chamber Entry & Sclerectomy
- AC entered along most of the width of the trapdoor base
- Block of deep sclera excised — typically using a Kelly punch (creates the internal sclerostomy/fistula)
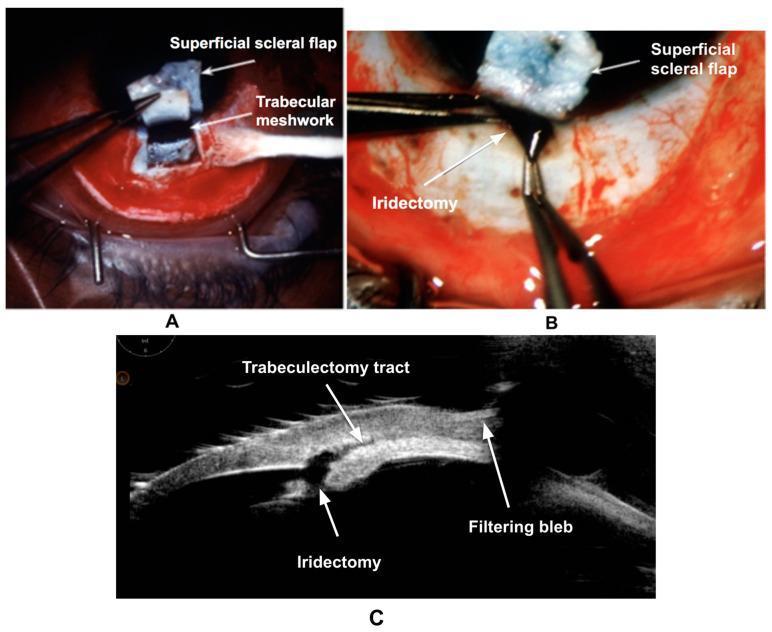
Step 8 — Peripheral Iridectomy
- Created to prevent iris prolapse into / blockage of the internal sclerostomy
- Some surgeons omit this step in pseudophakic eyes — but a small risk of iris prolapse remains if omitted
- Performed with Vannas scissors and fine forceps
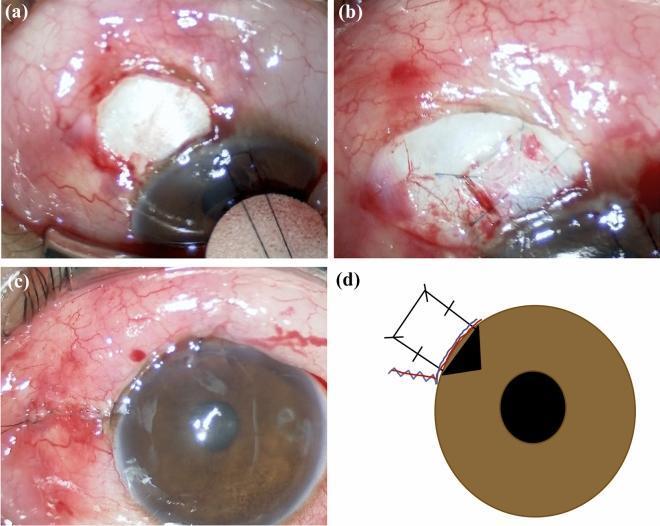
Step 9 — Scleral Flap Suturing
- Posterior corners sutured first
- Suturing strategy determines the key postoperative IOP balance:
| Suture Type | Effect |
|---|---|
| Lightly opposed | Allows early filtration; risk of hypotony |
| Tight closure with releasable sutures | Prevents early leakage; sutures released postoperatively to increase flow |
| Tight closure with lysable sutures | Released non-invasively with Nd:YAG laser postoperatively |
| Radial edge sutures | Some surgeons add these to reduce risk of lateral/side leak |
Releasable and lysable sutures are the modern preferred approach — they allow tight intraoperative closure (safe early phase) with controlled flow titration in the postoperative period.
Step 10 — Fistula Patency Test
- BSS injected through the paracentesis to deepen the AC and confirm the fistula is patent
- IOP is assessed and bleb formation observed
Step 11 — Conjunctival Closure
- Conjunctiva/Tenon capsule flap sutured (10-0 nylon or absorbable suture)
- Paracentesis irrigation repeated to produce a bleb
- Bleb inspected for leakage (Seidel test if needed)
Step 12 — Postoperative Medications
| Drug | Regimen |
|---|---|
| Atropine 1% | 1 drop at end of surgery (cycloplegia → deepens AC) |
| Pilocarpine 2% | Used instead of atropine if no iridectomy was performed |
| Steroid + antibiotic drops | 4× daily for 2 weeks |
| Steroid drops alone | Continue for 8–12 weeks thereafter |
| Steroid + antibiotic injection | Given under inferior conjunctiva at end of surgery |
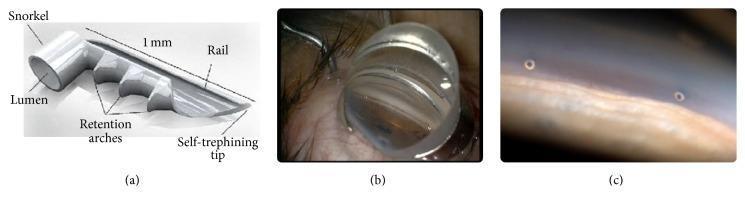
Variant: Ex-Press Mini-Shunt
- Scleral flap created identically to standard technique
- No Kelly punch sclerectomy — instead, a needle is used to enter the AC
- No peripheral iridectomy required
- Lower rates of hypotony and hyphaema compared to standard trabeculectomy
- IOP control is equivalent to standard trabeculectomy
- Not suitable for primary angle-closure glaucoma without concurrent/prior cataract surgery
Summary of Key Technical Decisions
| Decision Point | Options | Consideration |
|---|---|---|
| Conjunctival flap | Limbal vs. fornix-based | Bleb morphology and surgeon preference |
| Scleral flap shape | Rectangular / trapezoidal / triangular | Surgeon preference |
| Sclerostomy method | Kelly punch vs. Ex-Press shunt | Risk of hypotony, patient factors |
| Iridectomy | Performed vs. omitted | Omit only in pseudophakia with caution |
| Flap sutures | Releasable / lysable / loose | Titrate postoperative IOP |
| Antimetabolite | 5-FU / MMC / none | Based on failure risk factors |
Different techniques
Formation of aqueous humour
aqueous humour formation mechanisms ciliary body ophthalmology
aqueous humour formation ciliary body processes mechanisms diagram
aqueous humor formation ciliary epithelium
Formation of Aqueous Humour
Site of Production
Mechanisms of Formation
1. Ultrafiltration (Passive)
- Blood within the fenestrated capillaries of the ciliary processes exerts hydrostatic pressure
- A high-protein filtrate is driven by this pressure gradient out of the capillaries into the stroma of the ciliary processes
- This is a passive, pressure-dependent process — it does not require energy
2. Active Secretion (Primary mechanism)
- From the ciliary stromal filtrate, active transport of solutes (ions) occurs across the dual-layered ciliary epithelium:
- Outer pigmented epithelium (PE) — faces the stroma
- Inner non-pigmented epithelium (NPE) — faces the posterior chamber
- Key transporters involved:
- Na⁺/K⁺-ATPase — pumps sodium into the posterior chamber, driving osmotic water flow
- Carbonic anhydrase — generates bicarbonate ions, contributing to the osmotic gradient
- Aquaporins — water channels facilitating passive water movement
This is the predominant mechanism of aqueous formation and the target of most IOP-lowering drugs.
3. Diffusion (Passive)
- The osmotic gradient established by active ion transport facilitates passive flow of water into the posterior chamber
- Some additional plasma components diffuse across the epithelium along concentration gradients
Summary of Mechanisms
| Mechanism | Type | Driving Force | Contribution |
|---|---|---|---|
| Ultrafiltration | Passive | Hydrostatic pressure gradient | Minor |
| Active secretion | Active (energy-dependent) | Na⁺/K⁺-ATPase, carbonic anhydrase | Major |
| Diffusion | Passive | Osmotic/concentration gradient | Minor |
Neural Regulation
| Receptor | Effect on Aqueous Production |
|---|---|
| Beta-2 adrenoceptors | ↑ Increased secretion |
| Alpha-2 adrenoceptors | ↓ Decreased secretion |
This is the pharmacological basis for:
- Beta-blockers (e.g. timolol) — block β₂ receptors → reduce production
- Alpha-2 agonists (e.g. brimonidine) — stimulate α₂ receptors → reduce production
- Carbonic anhydrase inhibitors (e.g. dorzolamide, acetazolamide) — inhibit enzyme → reduce active secretion
Diurnal Variation
- Aqueous production follows a diurnal pattern — it is lower at night
- This contributes to normal diurnal IOP fluctuation (IOP tends to be higher in the morning)
Flow of Aqueous After Formation
- Posterior chamber (formed here by ciliary processes)
- → Through the pupil
- → Anterior chamber
- → Exits via:
| Route | Proportion | Details |
|---|---|---|
| Trabecular (conventional) | ~90% | Through trabecular meshwork → Schlemm's canal → episcleral veins. Pressure-sensitive. |
| Uveoscleral (unconventional) | ~10% | Across ciliary body face → suprachoroidal space → venous drainage of ciliary body, choroid, and sclera |
| Iris | Small amount | Direct drainage across the iris |
IOP Homeostasis
IOP is determined by the rate of aqueous production versus the resistance to outflow at the trabecular meshwork and episcleral venous pressure.
- Normal upper limit: 21 mmHg (applanation tonometry)
- Production rate: ~2–3 µL/min
Clinical Relevance
| Drug Class | Mechanism | Effect |
|---|---|---|
| Beta-blockers | Block β₂ → ↓ cAMP → ↓ active secretion | ↓ AH production |
| Alpha-2 agonists | Stimulate α₂ → ↓ secretion | ↓ AH production |
| CAIs (topical/systemic) | Inhibit carbonic anhydrase | ↓ AH production |
| Prostaglandin analogues | ↑ Uveoscleral outflow | ↑ AH drainage |
| Pilocarpine | Ciliary muscle contraction → opens TM | ↑ Trabecular outflow |
Minimally invasive glaucoma surgeries
minimally invasive glaucoma surgery MIGS types mechanisms 2024 2025
minimally invasive glaucoma surgery MIGS
minimally invasive glaucoma surgery MIGS stent trabecular iStent Hydrus
Minimally Invasive Glaucoma Surgery (MIGS)
Indications
- Mild to moderate glaucoma with slow visual field loss and modest target IOP (aiming for 15–17 mmHg)
- Combined with phacoemulsification + IOL to reduce dependence on topical medications
- Not suitable for advanced glaucoma requiring very low target pressures
Classification by Mechanism
Group 1 — Schlemm Canal Surgery (No Bleb)
A. Trabecular Excision (Ab Interno)
| Device | Mechanism |
|---|---|
| Trabectome | Electrocautery ablation of the trabecular meshwork; creates a direct AC–Schlemm canal communication |
| Kahook Dual Blade (KDB) | Dual-bladed goniotomy instrument; excises a strip of trabecular meshwork; can be combined with phaco |
B. Trabecular Bypass Stents
| Device | Mechanism |
|---|---|
| iStent inject | Titanium micro-stent inserted ab interno through the trabecular meshwork into Schlemm's canal; bypasses the meshwork |
| Hydrus Microstent | 8 mm nitinol intracanalicular scaffold; dilates and scaffolds Schlemm's canal across 3 clock hours |
C. Canaloplasty
| Device | Mechanism |
|---|---|
| Ab-interno canaloplasty (iTrack) | Viscodilation of Schlemm's canal 360° using a microcatheter + viscoelastic; no bleb formed |
Group 2 — Subconjunctival Drainage (Bleb-Forming)
| Device | Description |
|---|---|
| Xen Gel Stent | 6 mm gelatin stent (softens and swells in situ); ab interno insertion; drains to subconjunctival space |
| PreserFlo MicroShunt | SIBS polymer tube (8.5 mm); ab externo insertion; flow-limiting luminal diameter of 70 µm |
| InnFocus MicroShunt | Similar to PreserFlo |
- Mitomycin C 0.02% (0.1 ml) is usually injected subconjunctivally adjacent to the implant to reduce bleb fibrosis
- Bleb needling is often required postoperatively
- Shares complications with trabeculectomy: overfiltration, bleb-related infection, encapsulation
- Additional risk of stent malposition and erosion
Group 3 — Supraciliary/Uveoscleral Drainage (No Bleb)
| Device | Description |
|---|---|
| MINIject | 5 mm silicone implant made of thousands of interconnected hollow spheres; ab interno insertion; 0.5 mm protrudes into AC |
- No bleb formed
- No antimetabolite required
- Small risk of late corneal endothelial cell loss
Also Related: Non-Penetrating Glaucoma Surgery
| Procedure | Mechanism |
|---|---|
| Deep Sclerectomy | Two lamellar scleral flaps; deep flap excised leaving a thin trabecular/Descemet membrane window; aqueous diffuses out. Collagen implant + postoperative Nd:YAG goniopuncture improves long-term results |
| Viscocanalostomy | Schlemm canal identified and dilated with high-density viscoelastic; no open fistula; superficial flap sutured tightly (no bleb) |
- AC is never entered → avoids hypotony and its sequelae
- IOP reduction generally less than trabeculectomy
- Main indication: POAG (primary open-angle glaucoma)
- Preferred when advanced disease makes hypotony-related visual loss a concern
Complications Summary
| Group | Key Complications |
|---|---|
| Schlemm canal (Group 1) | Implant malposition, haemorrhage, infection, late corneal decompensation |
| Bleb-forming (Group 2) | Trabeculectomy-like complications + stent malposition/erosion |
| Supraciliary (Group 3) | Late corneal endothelial cell loss |
| All MIGS | Late failure → increases bleb fibrosis risk if trabeculectomy is subsequently needed |
Results
| Procedure | Outcome |
|---|---|
| iStent (stand-alone) | ~30% IOP reduction from baseline, sustained up to 5 years |
| Hydrus Microstent (Horizon Study) | Safer, less visual field loss, more effective than phaco alone at 5 years |
| Xen / goniotomy / canaloplasty (stand-alone) | At 2 years, 1 in 4 patients require further surgery |
⚠️ Results of MIGS combined with cataract surgery are biased — phacoemulsification itself independently reduces IOP by ~15%.
Recent Evidence
- PMID 38853535 (Clin Exp Ophthalmol, 2024): Systematic review/meta-analysis — angle-based MIGS in normal tension glaucoma shows meaningful IOP reduction
- PMID 40439165 (Turk J Ophthalmol, 2025): Review of ab interno goniotomy/goniectomy techniques
- PMID 39670502 (Dtsch Arztebl Int, 2025): Meta-analysis confirms trabeculectomy remains gold standard for advanced glaucoma; MIGS has better safety profile for mild-moderate disease