How can master pediatrics in terms of its protocol??
Reading File
Asking for Preferences
Finding Sources
Searching the Web
mastering pediatrics clinical protocols approach guide 2025
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Now I have enough material from authoritative sources to give a thorough, structured answer. Here it is:
Mastering Pediatrics: A Protocol-Based Guide
Pediatrics is unique because children are not simply small adults - their physiology, drug dosing, vital sign norms, and disease presentations change with age. Mastering it requires internalizing a set of protocols organized around assessment, resuscitation, and disease management. Below is a structured breakdown.
1. The Core Mindset: Age-Stratified Thinking
Everything in pediatrics is adjusted by age group:
| Age Group | Category |
|---|---|
| 0-28 days | Neonate |
| 1-12 months | Infant |
| 1-3 years | Toddler |
| 3-12 years | Child |
| 12-18 years | Adolescent |
Vital signs, drug doses, fluid volumes, normal lab ranges, and differential diagnoses all shift across these groups. Anchor every clinical decision to the child's age and weight.
2. The Pediatric Assessment Triangle (PAT) - Your First Protocol
Before touching the patient, use the PAT to form a rapid impression from the doorway. It has three sides:
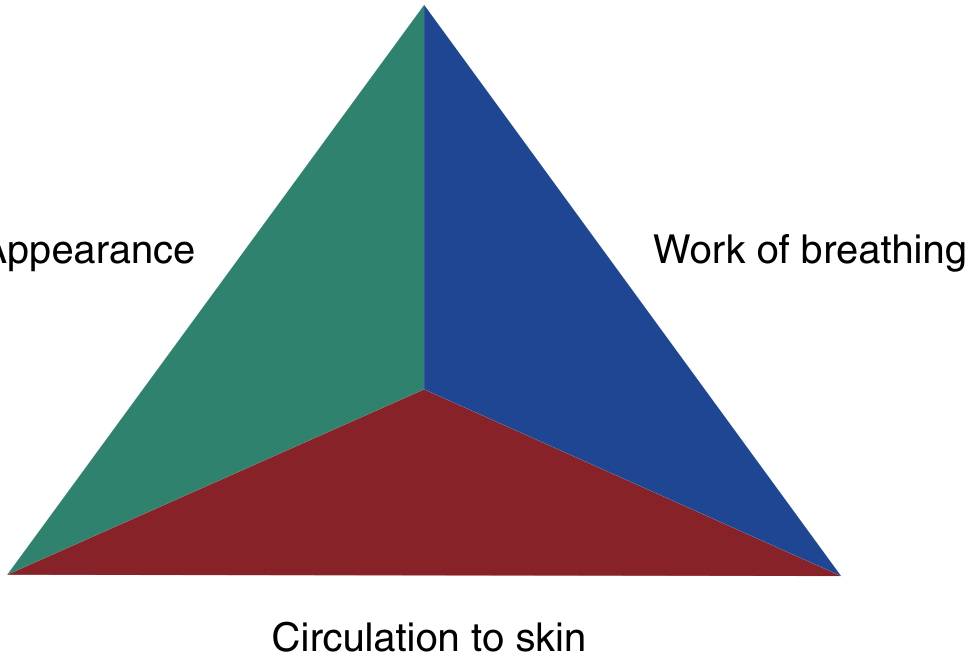
Side 1 - Appearance (TICLS mnemonic):
- Tone - is the child floppy?
- Interactivity - does the child engage with surroundings?
- Consolability - can the parent console the child?
- Look/Gaze - is eye tracking normal?
- Speech/Cry - is the cry weak, high-pitched, or absent?
Side 2 - Work of Breathing:
- Abnormal sounds: stridor, grunting, snoring, wheezing
- Abnormal positioning: sniffing, tripod
- Retractions, nasal flaring, head bobbing
Side 3 - Circulation to the Skin:
- Pallor, mottling, cyanosis
- Capillary refill > 2 seconds
- Petechiae
Interpreting the PAT:
| PAT Findings | Physiologic State |
|---|---|
| Abnormal appearance only | CNS/metabolic problem |
| Abnormal work of breathing only | Respiratory distress |
| Abnormal circulation only | Compensated shock |
| Abnormal appearance + circulation | Decompensated shock |
| All three abnormal | Cardiopulmonary failure |
- ROSEN's Emergency Medicine, Concepts and Clinical Practice
3. Normal Pediatric Vital Signs - Know Your Numbers
Published in Roberts and Hedges' Clinical Procedures in Emergency Medicine:
Heart Rate (beats/min) by Percentile:
| Age | 5th %ile | 50th %ile | 95th %ile |
|---|---|---|---|
| 0-3 months | 113 | 140 | 171 |
| 3-6 months | 108 | 135 | 167 |
| 6-9 months | 104 | 131 | 163 |
| 9-12 months | 101 | 128 | 160 |
| 12-18 months | 97 | 124 | 157 |
Key principle: "Normal" vital signs do NOT rule out serious illness. Children can compensate and maintain near-normal vitals until they suddenly decompensate.
Blood Pressure estimation (quick formula):
- Minimum systolic BP = 70 + (2 x age in years) for children 1-10 years
- Below this threshold = hypotension requiring urgent intervention
Respiratory Rate:
- Neonate: 30-60/min
- Infant: 25-50/min
- Toddler: 20-30/min
- School age: 16-24/min
- Adolescent: 12-20/min
4. Resuscitation Protocols
4a. Neonatal Resuscitation (NRP)
The neonatal resuscitation algorithm follows a stepwise approach at birth:
- Initial assessment - term? good tone? breathing/crying?
- Warm, dry, stimulate - within 30 seconds
- Reassess HR - HR < 100 = begin positive pressure ventilation (PPV)
- PPV with SpO2 monitoring - target SpO2 by minute post-birth (60-65% at 1 min, rising to 85-95% at 10 min)
- HR < 60 after 30 seconds of effective PPV - start chest compressions (3:1 ratio)
- Epinephrine if HR < 60 persists: 0.01-0.03 mg/kg IV/IO
- ROSEN's Emergency Medicine
4b. Pediatric Advanced Life Support (PALS - 2025 AHA Update)
The 2025 AHA PALS guidelines (just updated) emphasize:
Cardiac Arrest:
- High-quality CPR: 100-120 compressions/min, depth at least 1/3 chest AP diameter
- Compression:ventilation ratio - 30:2 (single rescuer) or 15:2 (two rescuers, with advanced airway)
- Defibrillation: 2 J/kg first shock, 4 J/kg subsequent shocks (maximum 10 J/kg or adult dose)
- Epinephrine: 0.01 mg/kg IV/IO every 3-5 minutes
- Amiodarone (pulseless VT/VF): 5 mg/kg IV/IO bolus
Shock Recognition:
- Tachycardia + poor perfusion = shock, regardless of blood pressure
- Compensated shock: normal BP with tachycardia + prolonged capillary refill
- Decompensated shock: hypotension (late sign in children)
5. Sepsis Protocol (Surviving Sepsis 2020 - Pediatric Bundle)
Per the 2020 pediatric Surviving Sepsis Campaign guidelines, a bundled approach within 1 hour reduces mortality (OR = 0.59):
The 1-Hour Sepsis Bundle:
- Obtain blood cultures
- Administer IV/IO fluid bolus - 10-20 mL/kg isotonic crystalloid (reassess after each bolus; avoid large upfront boluses unlike adult protocol)
- Start broad-spectrum antibiotics (within 1 hour of recognition)
- Measure lactate; target < 2 mmol/L within 3-4 hours
- Vasopressors if shock persists after 40-60 mL/kg total fluids - norepinephrine or epinephrine are first-line in pediatric septic shock
Vascular Access: Peripheral IV or intraosseous (IO) device - do NOT delay resuscitation waiting for central access. Vasoactive infusions CAN run through peripheral IVs temporarily.
Corticosteroids: Hydrocortisone 1-2 mg/kg (max 100 mg) for fluid and vasopressor-refractory shock only.
Glucose: Children are prone to hypoglycemia (limited glycogen stores) - check glucose early and correct if low. Target blood glucose 72-180 mg/dL.
- ROSEN's Emergency Medicine
6. Key Disease-Specific Protocols to Master
Febrile Infant Protocol (Age-Based)
- < 28 days: Full septic workup (blood, urine, CSF cultures) + empiric antibiotics regardless of appearance
- 29-60 days: Risk-stratify using clinical criteria (Rochester, Step-by-Step, or PECARN rules) - consider LP
- 61-90 days: Well-appearing + vaccinated - may monitor without LP if low-risk criteria met
- > 3 months: Focus on source; treat based on clinical findings
Febrile Seizure Protocol
- Simple febrile seizure (< 15 min, generalized, single episode): No LP, no EEG, no anti-epileptics
- Complex febrile seizure: Investigate underlying cause
Bronchiolitis (RSV)
- Supportive care only: nasal suctioning + hydration
- No salbutamol, steroids, antibiotics, or epinephrine routinely recommended (AAP guideline)
- Admission criteria: SpO2 < 90%, apnea, poor feeding, respiratory distress
Croup Protocol
- Mild (no stridor at rest): Dexamethasone 0.15-0.6 mg/kg oral/IM single dose
- Moderate-severe: Dexamethasone 0.6 mg/kg + nebulized epinephrine (0.5 mL/kg of 1:1000, max 5 mL)
- Monitor for 2-3 hours post-epinephrine before discharge
Asthma Exacerbation Protocol
- Mild-moderate: Salbutamol (0.15 mg/kg/dose, min 2.5 mg) q20min x3, ipratropium bromide
- Severe: Continuous salbutamol, IV/IM magnesium sulfate 25-75 mg/kg (max 2.5 g), systemic steroids (prednisolone 1-2 mg/kg)
- Life-threatening: IV salbutamol, intubation as last resort (high risk of complications)
Meningitis Protocol
- Empiric treatment: Ceftriaxone 100 mg/kg/day IV + vancomycin (if Strep pneumoniae suspected)
- Dexamethasone 0.15 mg/kg q6h x4 days (reduces neurological sequelae in H. influenzae and Strep pneumoniae meningitis)
- Do NOT delay antibiotics for CT or LP if meningitis is suspected
7. Weight-Based Dosing - The Broselow Tape
One of the most practical pediatric tools. The Broselow tape uses the child's length to estimate weight, which then maps to color-coded drug doses and equipment sizes. Use it for every resuscitation.
Quick weight estimate:
- < 1 year: Weight (kg) = (Age in months / 2) + 4
- 1-5 years: Weight (kg) = (Age in years x 2) + 8
- 6-12 years: Weight (kg) = (Age in years x 3) + 7
8. Vaccination & Preventive Protocols
Follow the AAP/CDC immunization schedule for all age groups. Key milestones:
- Birth: Hepatitis B
- 2, 4, 6 months: DTaP, IPV, Hib, PCV15/20, Rotavirus, HepB
- 12-15 months: MMR, Varicella, PCV, Hib, HepA
- 11-12 years: Tdap, HPV, Meningococcal
9. Study Strategy for Mastery
To systematically master pediatric protocols:
- Reference resources: Harriet Lane Handbook (best quick-reference for dosing/protocols), Nelson Textbook of Pediatrics (comprehensive), AAP Red Book (infectious disease)
- Simulation: PALS and NRP courses give hands-on resuscitation experience
- AAP clinical practice guidelines: Available at aap.org/CPG - updated with GRADE methodology from 2025 onward
- Pattern-based learning: Master the "age + weight + developmental stage" triad for every condition
- High-yield topics: Febrile infant algorithms, sepsis bundles, respiratory emergencies, growth/development milestones, and vaccination schedules appear most frequently in both exams and clinical practice
The two best single references available in the library for protocol mastery are the Harriet Lane Handbook (Johns Hopkins, 23rd ed.) for quick drug/protocol lookups and the AAP Red Book 2021 for infectious disease protocols. Both are available in the textbook library.
How to score well in exams since they are very specific
Asking for Preferences
Good, that narrows it down well. University pediatrics written exams are notorious for testing very specific numbers, criteria, and protocols. Here is a targeted strategy:
Scoring Well in University Pediatrics Written Exams
The Core Problem
University pediatrics exams test precision - exact cut-off ages, specific mg/kg doses, diagnostic criteria with specific numbers, and named syndromes. Vague knowledge fails. You need to know the exact answer, not just the concept.
1. Know What Gets Asked (Topic Prioritization)
University examiners tend to recycle from these high-yield clusters:
Cluster A - Numbers & Cut-offs (Most Specific)
These are pure memory items that carry disproportionate marks:
| Topic | What to Memorize Exactly |
|---|---|
| Vital signs by age | HR, RR, BP ranges for each age group |
| Weight formulas | Neonate: birth weight regained by day 10; doubles by 5 months; triples by 1 year |
| Height milestones | Birth 50 cm → 75 cm at 1 yr → 100 cm at 4 yrs |
| Head circumference | Birth 34 cm → 47 cm at 1 yr |
| Developmental milestones | Exact age for each motor, language, social skill |
| Vaccination schedule | Exact age, number of doses, route for every vaccine |
| Nutritional requirements | Caloric need by age, protein requirements, breastfeeding duration |
| Fluid calculations | Holliday-Segar formula: 100 mL/kg for first 10 kg, 50 mL/kg for next 10 kg, 20 mL/kg thereafter |
Cluster B - Diagnostic Criteria (Frequently Tested Verbatim)
- Kawasaki disease: Fever ≥ 5 days + 4 of 5 criteria (conjunctivitis, oral changes, rash, extremity changes, cervical lymphadenopathy ≥ 1.5 cm)
- Rheumatic fever (Jones criteria): 2 major OR 1 major + 2 minor + evidence of strep infection
- Nephrotic syndrome: Proteinuria > 40 mg/m²/hr, hypoalbuminemia < 2.5 g/dL, edema, hyperlipidemia
- Dehydration scoring: Mild < 5%, moderate 5-10%, severe > 10%
- Malnutrition (WHO): Weight-for-height Z-score < -3 = severe acute malnutrition
Cluster C - First-Line Treatments (Examiners Love "Drug of Choice")
| Condition | Drug of Choice |
|---|---|
| Neonatal sepsis (early-onset) | Ampicillin + Gentamicin |
| Bacterial meningitis (> 3 months) | Ceftriaxone |
| Febrile convulsion (acute) | Diazepam (rectal/IV) |
| Status epilepticus | IV Lorazepam → Phenytoin → Phenobarbitone |
| Croup (moderate-severe) | Dexamethasone + nebulized epinephrine |
| Nephrotic syndrome (first episode) | Prednisolone 2 mg/kg/day x 4 weeks |
| Kawasaki | Aspirin + IVIG |
| Scurvy | Vitamin C |
| Rickets | Vitamin D + Calcium |
Cluster D - Milestones (Always in Exams)
Memorize in this order - it builds on itself:
| Age | Motor | Language | Social |
|---|---|---|---|
| 2 months | Lifts head 45° | Coos | Social smile |
| 4 months | Rolls front to back | Laughs | Recognizes mother |
| 6 months | Sits with support | Babbles (monosyllables) | Stranger anxiety begins |
| 9 months | Stands with support | "Mama/Dada" non-specific | Waves bye-bye |
| 12 months | Walks with support | 1-2 words meaningful | Plays pat-a-cake |
| 18 months | Runs | 10+ words | Symbolic play |
| 2 years | Up-down stairs | 2-word phrases | Parallel play |
| 3 years | Rides tricycle | 3-word sentences | Group play |
2. The Exam Technique for Specific Questions
Read the question twice - look for the "trapper"
University questions often contain one keyword that changes the answer:
- "Which vaccine is NOT given at birth?" - trapper is "NOT"
- "The FIRST sign of puberty in girls" - answer is breast bud (thelarche), not pubic hair
- "Drug of CHOICE vs drug of FIRST CHOICE vs INITIAL drug" - these may differ
For "what is the next step" questions
The answer priority is: Stabilize → Diagnose → Treat
- If the child is unstable: airway/breathing/circulation FIRST
- If stable: go to the most specific diagnostic test
- Never choose treatment before diagnosis unless it's a resuscitation scenario
For dose-based questions
Learn these in mg/kg not absolute doses, because exams give you weight:
- Paracetamol: 15 mg/kg/dose q4-6h
- Ibuprofen: 5-10 mg/kg/dose q6-8h
- Amoxicillin (standard): 25-50 mg/kg/day in 3 divided doses
- Ceftriaxone: 50-100 mg/kg/day once daily
3. Active Recall Over Passive Reading
Passive reading of textbooks is the least effective method for specific-facts exams.
What works instead:
-
Flashcard system (Anki) - Make one card per specific number/fact. Example front: "Age at which birth weight doubles?" Back: "5 months." Review daily with spaced repetition.
-
Draw tables from memory - After reading vaccination schedules or milestones, close the book and reconstruct the table. Check gaps. Repeat until clean.
-
Past paper drilling - Get 5-10 years of your university's past questions. Most universities recycle 40-60% of questions. Pattern-match which topics come up every year.
-
Teach-back method - Explain a protocol (e.g., febrile seizure management) out loud as if teaching someone else. Where you hesitate = where you need to review.
-
One-page summaries - After each topic, write a single A4 sheet with only the numbers and drug names. Use this sheet for final revision, not the textbook.
4. Topic-Specific High-Yield Tables to Memorize
Vaccination Schedule (EPI - most universities test this)
| Age | Vaccines |
|---|---|
| Birth | BCG, OPV-0, HepB-1 |
| 6 weeks | OPV-1, DPT-1, HepB-2, Hib-1, Rota-1 |
| 10 weeks | OPV-2, DPT-2, Hib-2, Rota-2 |
| 14 weeks | OPV-3, DPT-3, HepB-3, Hib-3, IPV |
| 9 months | Measles/MR-1, OPV-4 |
| 15-18 months | MMR, DPT booster, OPV booster |
(Exact schedule may vary by country - cross-check with your national EPI program)
Dehydration Assessment
| Feature | Mild (< 5%) | Moderate (5-10%) | Severe (> 10%) |
|---|---|---|---|
| Eyes | Normal | Sunken | Very sunken |
| Skin turgor | Normal | Reduced | Very reduced |
| Mucous membranes | Moist | Dry | Very dry |
| Fontanelle | Normal | Sunken | Very sunken |
| Urine output | Normal | Reduced | Oliguria/anuria |
Rehydration Protocol (WHO/ORS)
- Mild-moderate: ORS 75 mL/kg over 4 hours
- Severe (with shock): Ringer's lactate 20 mL/kg IV bolus, repeat if needed
- Maintenance after rehydration: continue ORS + replace ongoing losses
5. Exam Week Strategy
1 week before:
- Only review your one-page summaries and flashcards
- Do past papers under timed conditions
- Do NOT start new topics
Night before:
- Read only the highest-yield tables (milestones, vaccines, diagnostic criteria)
- Sleep - sleep consolidates memory more than a late-night session
During the exam:
- Attempt all questions - no negative marking in most university exams
- For unknown answers: use your knowledge of the age group + "safest/most conservative" option to make an educated guess
- Flag and return to uncertain answers after completing the rest
6. The Single Best Mindset Shift
Most students study pediatrics broadly. Top scorers study it vertically - they master one topic completely (all numbers, criteria, treatment steps, complications) before moving to the next.
For example, mastering nephrotic syndrome means knowing:
- Exact diagnostic criteria (proteinuria threshold, albumin level)
- First-line treatment (prednisolone dose and duration)
- Complications (infections, thrombosis, hyperlipidemia)
- Indication for biopsy (steroid resistance = 4 weeks no response)
- Most common cause in children (minimal change disease, 90%)
That depth on a single topic scores more marks than shallow coverage of 10 topics.
The books most useful for your purpose are:
- Harriet Lane Handbook - protocols, drug doses, normal values (quick lookup)
- Nelson Essentials - concise topic coverage ideal for exam prep
- AAP Red Book - infectious disease protocols, vaccine schedules
- Your university lecture notes + past papers - these define exactly what your examiners want
Find recent past papers or model questions from your university
I don't have access to your university's past papers or internal exam materials - I don't know which university you attend, and even if I did, past papers are typically stored on university intranets, student portals, or department offices, not publicly available online.
Here is what you can actually do to get them:
Where to Find Past Papers
From Your Institution Directly
- Department notice board / library - Most medical school libraries keep physical or digital archives of past professional exam papers
- Your department's student representative - They often collect and circulate past papers
- Ask senior students (final years or those who just sat the exam) - The most reliable source; they often have organized question banks from previous years
- Your course coordinator or faculty office - Some universities officially release past papers after each sitting
Online Sources (General Pediatrics MCQs)
These won't be your university's exact papers, but cover the same content:
- Amboss - High-quality pediatrics question bank aligned with medical school level
- Osmosis - Question bank + explanations
- TeachMePediatrics - Free, topic-based questions
- PassMedicine - Strong for UK-based medical schools
- PreTest Pediatrics (book) - Classic medical school question bank
- BRS Pediatrics (book) - Board-style questions with detailed explanations
For Specific Exam Boards
- If you're in a country with a national medical licensing body (e.g., PMDC in Pakistan, NMC in India, GMC in UK), check their official website - some publish sample questions or past paper formats
What I Can Do
If you tell me your university name or country/region, I can search for any publicly available past papers or question formats specific to your institution. I can also generate a realistic model question paper based on standard university pediatrics exam patterns - covering the high-yield topics, question styles, and difficulty level typical of written exams.
Would you like me to create a model question paper for you?
This is a shared conversation. Sign in to Orris to start your own chat.