TURP Syndrome
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information from two authoritative anesthesiology textbooks. Here is a thorough overview of TURP Syndrome.
TURP Syndrome
Definition
TURP syndrome describes a constellation of symptoms caused by systemic absorption of large volumes of hypotonic, electrolyte-free irrigating fluid during transurethral resection of the prostate (or similar endoscopic procedures). The result is a combination of hypervolemia, dilutional hyponatremia, hypoosmolality, and solute toxicity from the irrigant itself. — Miller's Anesthesia, 10e
Why It Happens
During monopolar TURP, isotonic saline cannot be used as irrigation (it disperses the electrocautery current). Instead, slightly hypotonic nonelectrolyte solutions are used:
- Glycine 1.5% (230 mOsm/L) — most common
- Sorbitol 2.7% + mannitol 0.54% (195 mOsm/L)
- Others: sorbitol 3.3%, mannitol 3%, dextrose 2.5–4%, urea 1%
Resection opens prostatic venous sinuses, allowing direct intravascular absorption. On average, 10–30 mL of fluid is absorbed per minute of resection time — procedures lasting 2 hours may result in 6–8 L of absorption. — Miller's Anesthesia, 10e
Factors governing absorption rate:
- Height of irrigating fluid above the surgical table (hydrostatic pressure)
- Degree of bladder distension
- Extent of open venous sinuses
- Duration of resection
Pathophysiology
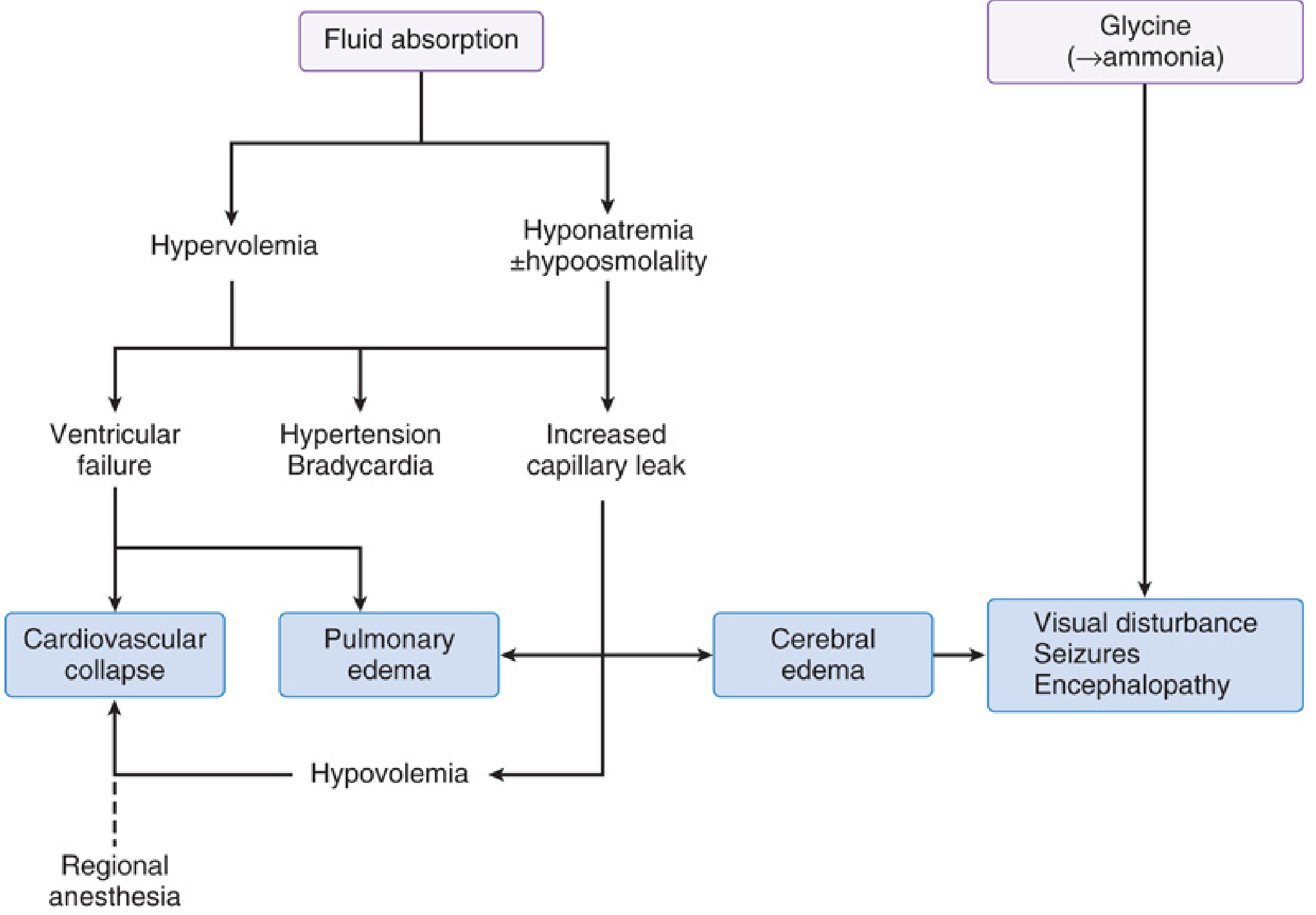
There are three main pathophysiologic axes:
1. Hypervolemia
Rapid intravascular volume expansion leads to:
- Early hypertension + bradycardia (reflex)
- Progression to ventricular failure → cardiovascular collapse
- Pulmonary edema
- Later, hypertension + hyponatremia causes a net outward osmotic/hydrostatic water shift → intravascular hypovolemia → hypotensive shock
2. Hyponatremia ± Hypoosmolality
The dilutional drop in serum sodium is the central problem. Severity of symptoms correlates with rate of fall, not just absolute level:
| Serum Na⁺ | Clinical Features |
|---|---|
| < 120 mEq/L | Restlessness, confusion, CNS symptoms, hypotension, pulmonary edema, CHF |
| < 115 mEq/L | ECG changes: wide QRS, ventricular ectopy, ST elevation |
| < 110 mEq/L | Seizures, loss of consciousness |
| ~100 mEq/L | Respiratory and cardiac arrest |
CNS signs are primarily driven by acute serum hypoosmolality (not hyponatremia per se), causing cerebral edema. — Miller's Anesthesia, 10e
3. Solute Toxicity (Glycine, Ammonia, Others)
- Glycine is an inhibitory retinal neurotransmitter → transient blindness (sluggish/nonreactive pupils — distinguishing it from cerebral edema where pupillary reflexes are preserved)
- Glycine also activates NMDA receptors → seizures
- Glycine can cause T-wave changes and elevated CK-MB (without MI criteria) for up to 24 hours
- Ammonia: glycine is hepatically deaminated to ammonia → encephalopathy; nausea/vomiting typically within 1 hour post-op; coma at high levels (10–12 hours duration)
- Sorbitol → hyperglycemia
- Mannitol → additional intravascular volume expansion
Incidence & Mortality
- Incidence of mild-to-moderate TURP syndrome: 0.78–1.4%
- Incidence across all TURP procedures: up to 10–15% (including subclinical)
- Mortality with severe TURP syndrome (Na⁺ < 120 mEq/L): up to 25%
Risk factors: large prostate gland, resection > 90 minutes, large volumes of irrigation fluid, extensive venous sinus opening. — Miller's Anesthesia, 10e; Morgan & Mikhail, 7e
Clinical Presentation
Onset can be intraoperative or up to several hours postoperatively. Symptoms include:
- Headache, restlessness, confusion
- Nausea, vomiting
- Cyanosis, dyspnea
- Hypertension (early) → hypotension (late)
- Arrhythmias
- Visual disturbances / transient blindness
- Seizures
- Pulmonary edema
Diagnosis
High clinical suspicion is key. Workup when TURP syndrome is suspected:
- Serum electrolytes (confirm hyponatremia)
- Serum osmolality
- Arterial blood gas
- Blood glucose
- 12-lead ECG
- Consider serum ammonia if encephalopathy present
Treatment
Mild (Na⁺ > 120 mEq/L, minimal symptoms)
- Fluid restriction
- Loop diuretic (furosemide) — to eliminate absorbed free water
- Supplemental oxygen, cardiovascular support
Severe (Na⁺ < 120 mEq/L, significant CNS/cardiovascular compromise)
- IV hypertonic saline (3% NaCl) — correct cautiously to avoid central pontine myelinolysis
- Rate of correction: generally no faster than 8–12 mEq/L per 24 hours
- Stop the procedure as rapidly as possible
Novel Prevention
- Tolvaptan 15 mg orally 2 hours preoperatively (selective vasopressin V2 receptor antagonist → free water excretion) has been proposed, especially for long or combined cystoscopic procedures. — Miller's Anesthesia, 10e
Prevention
- Use bipolar TURP with isotonic saline irrigant (eliminates hyponatremia risk)
- Limit resection time (< 90 minutes preferred)
- Limit irrigation fluid bag height
- Monitor fluid balance (input vs. output)
- Use spinal (neuraxial) anesthesia — allows real-time monitoring of mental status changes; also associated with lower 30-day mortality than general anesthesia
- Use ethanol-tagged irrigation fluid and exhaled breath ethanol monitoring (to detect absorption)
Analogous Syndromes
TURP syndrome has also been reported with:
- Transurethral resection of bladder tumors
- Ureteroscopy
- Hysteroscopy (transcervical resection of endometrium)
- Arthroscopy
All share the same mechanism: absorption of large volumes of hypotonic irrigant through open vascular sinuses.
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e, pp. 1302–1305 | Miller's Anesthesia, 10e, pp. 8471–8478 & 6372–6374
This is a shared conversation. Sign in to Orris to start your own chat.