Gi assesment: palpation,jaundice and
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
I have comprehensive content from Yamada's. Let me synthesize a thorough answer.
GI Assessment: Palpation, Jaundice & Percussion
Based on Yamada's Textbook of Gastroenterology, 7th ed.
1. Palpation
Palpation and percussion together can identify:
- Localized masses
- Free peritoneal fluid (ascites)
- Areas of tenderness
- Localized or diffuse peritoneal inflammation
Key principles
- Start with light palpation to identify areas of tenderness, then progress to deep palpation for organ assessment and masses.
- Voluntary vs. involuntary guarding: Cold examiner hands or brusque contact can produce voluntary guarding — warm hands and gentle technique are essential for accurate assessment. True involuntary guarding reflects genuine peritoneal irritation.
- Rebound tenderness (Blumberg's sign): Eliciting it may suggest peritonitis when positive, but it is not always reliable on its own.
- Less reliable for chronic pain: Palpation is less likely to elicit peritoneal signs (rebound tenderness, guarding) in chronic or recurrent abdominal pain compared to acute pain.
- Attention during palpation should also be paid to skin lesions, rashes, pallor, jaundice, and edema.
Organ-specific palpation
| Organ | What to assess |
|---|---|
| Liver | Begin at the liver edge; palpate for hepatomegaly, tenderness (hepatitis, congestion), or pulsatility (tricuspid regurgitation) |
| Spleen | Ask patient to take deep breaths; feel for splenomegaly tip in the LUQ |
| Gallbladder | Murphy's sign: deep inspiration during RUQ palpation causing arrest of inspiration indicates cholecystitis |
Murphy's Sign (Cholecystitis)
Deeply palpate the right upper quadrant (RUQ) and ask the patient to inhale. Sudden arrest of inspiration due to pain = positive Murphy's sign, indicating acute cholecystitis.
2. Percussion
Percussion combined with inspection provides the best chance of identifying:
- Organ size (hepatic and splenic dullness)
- Ascites (shifting dullness, fluid wave)
- Distended bowel (tympany)
- Solid masses or organomegaly (dullness)
Liver percussion
- Normal liver span: ~6–12 cm in the mid-clavicular line.
- Dullness over the liver area; loss of hepatic dullness → pneumoperitoneum (free air under diaphragm — surgical emergency).
Splenic percussion
- Inspection and percussion combined with palpation provide the best chance of identifying an enlarged spleen. The patient should take deep breaths while checking for the tip of the spleen.
- Dullness in Traube's space (left lower anterior chest) suggests splenomegaly.
Ascites
- Shifting dullness: Percuss from midline (tympanic) to flank (dull); roll patient to opposite side and recheck — if dullness shifts, ascites likely.
- Fluid wave / puddle sign: Useful for large-volume ascites.
Bowel / Obstruction
- Infrequent, prolonged rushes of high-pitched "tinkling" peristalsis are heard over distended bowel loops in intestinal obstruction.
- Diffuse tympany suggests obstruction or ileus.
- Absent bowel sounds + diffuse tenderness → peritonitis.
3. Jaundice
Jaundice is a key finding on GI physical examination and represents elevated serum bilirubin (>2–3 mg/dL visible clinically).
Detection on exam
- Best seen in sclera (icteric sclerae) and mucous membranes — scleral icterus often appears first.
- Also visible in the skin, particularly on the face and trunk in natural light.
- Associated findings to assess simultaneously: pallor, edema, rashes/skin lesions, spider angiomata, palmar erythema, asterixis (hepatic encephalopathy).
Categories of jaundice (clinical approach)
| Type | Mechanism | Key Features |
|---|---|---|
| Pre-hepatic | Hemolysis → excess unconjugated bilirubin | Pale stools, dark urine, anemia; no hepatomegaly |
| Hepatocellular | Liver cell damage (hepatitis, cirrhosis) | Tender hepatomegaly, stigmata of chronic liver disease |
| Post-hepatic (obstructive) | Biliary obstruction (stones, stricture, cancer) | Dark urine, pale/clay-coloured stools, Courvoisier's sign |
Courvoisier's Sign
In a jaundiced patient, a palpable, non-tender gallbladder suggests malignant biliary obstruction (e.g., pancreatic head cancer), since gallstones typically cause a scarred, non-distensible gallbladder.
Jaundice + Percussion findings
- Dullness to percussion in the lower lung fields may be present with hepatic abscess or empyema.
- Hepatomegaly percussed > 12 cm MCL: suggests hepatitis, congestion, or malignant infiltration.
- Tympany + jaundice: consider proximal bowel obstruction with biliary involvement.
Clinical Pearls
- Always inspect before palpating/percussing: note scars, distension, visible pulsations or peristalsis.
- Auscultate before palpation to avoid altering bowel sounds.
- A systematic approach (Inspection → Auscultation → Percussion → Palpation) ensures no finding is missed.
- Jaundice, ascites, and splenomegaly together = portal hypertension until proven otherwise.
- RUQ tenderness + fever + jaundice = Charcot's triad → ascending cholangitis (emergency).
— Yamada's Textbook of Gastroenterology, 7th ed. | Goldman-Cecil Medicine
Jvp and murmur examination
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have all the material needed. Here is the full synthesis:
JVP & Murmur Examination
— Harrison's Principles of Internal Medicine, 22nd ed. | Fuster & Hurst's The Heart, 15th ed.
PART 1: Jugular Venous Pressure (JVP)
Why It Matters
The JVP is the single most important bedside measurement from which to estimate volume status and right heart filling pressure.
Which Vein to Use
- Internal jugular vein (IJV) — preferred. It is valveless and directly in line with the SVC and right atrium.
- External jugular vein — valved and not directly in line, but can still discriminate high vs. low CVP.
How to Measure
- Position patient at 30–45° (adjust if needed — elevated JVP may require sitting upright).
- Identify the highest point of jugular venous pulsation.
- Measure the vertical distance from this point to the sternal angle (angle of Louis).
- >4.5 cm above the sternal angle = elevated JVP (abnormal).
- If pulsations are visible above the clavicle in the sitting position, this is clearly abnormal (distance from clavicle to right atrium is ≥10 cm).
Note: Sternal angle measurement tends to underestimate true CVP; it should be used to distinguish normal from elevated, not for precise quantification.
JVP vs. Carotid Pulse — How to Differentiate
| Feature | JVP | Carotid |
|---|---|---|
| Pulsation character | Biphasic (in sinus rhythm) | Monophasic |
| Obliteration with pressure | Easily obliterated | Not easily obliterated |
| Effect of posture/inspiration | Changes with position | Does not change |
The JVP Waveform
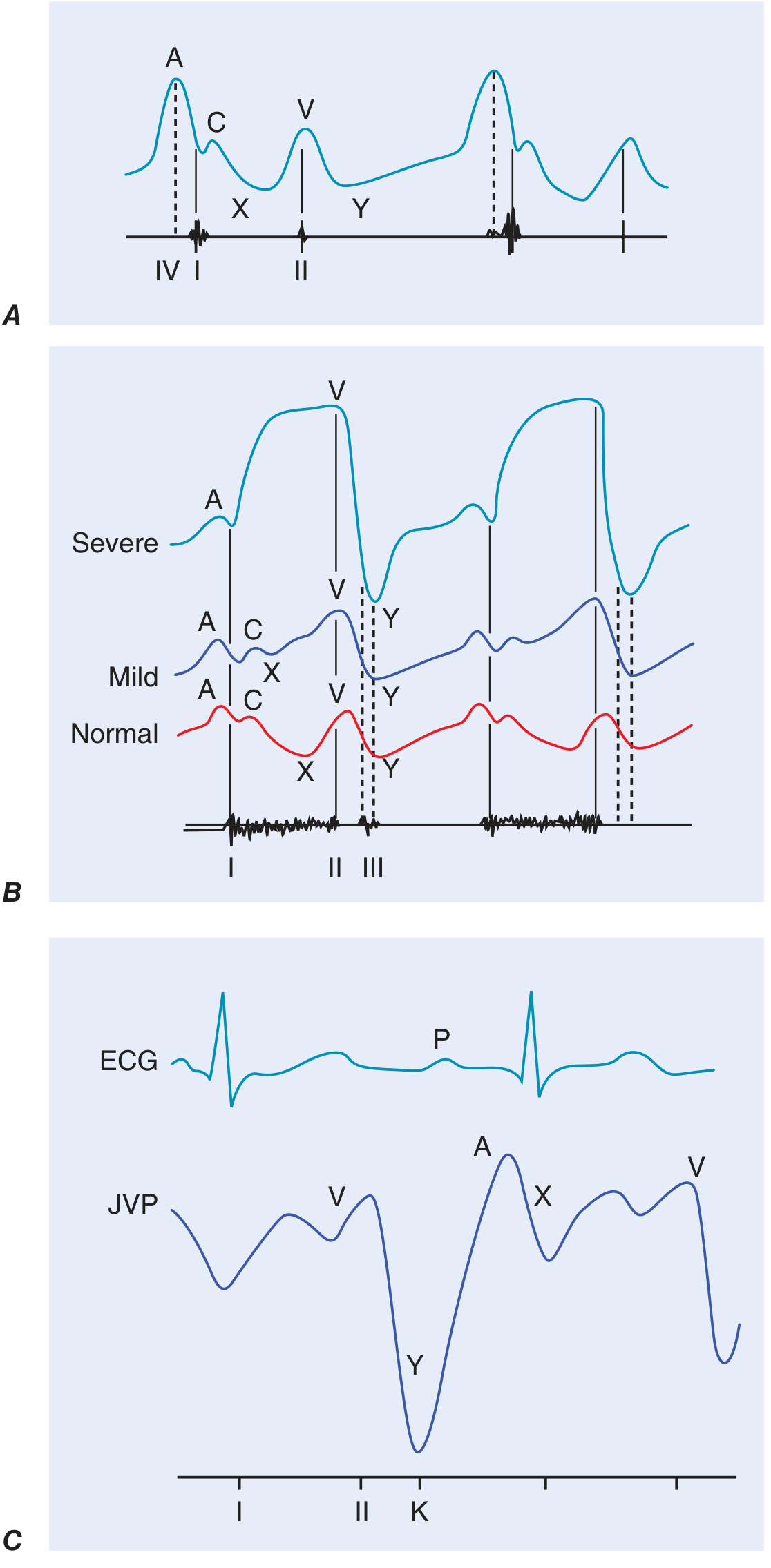
Panel A: Normal JVP with labeled A, C, V waves and X, Y descents. Panel B: Comparison of normal, mild, and severe tricuspid regurgitation patterns. Panel C: JVP correlated with ECG in constrictive pericarditis.
| Component | Timing | Represents |
|---|---|---|
| a wave | After P wave, just before S1 | Right atrial presystolic contraction |
| x descent | After a wave | Fall in RA pressure after tricuspid valve opens |
| c wave | Interrupts x descent | Closed tricuspid valve pushed into RA during early systole |
| v wave | During ventricular systole | Atrial filling (venous return to RA) |
| y descent | After v wave peak | Tricuspid valve opens → RA empties into RV |
Abnormal Waveform Patterns
| Finding | Interpretation |
|---|---|
| Prominent a wave | Reduced RV compliance (pulmonary stenosis, pulmonary HTN) |
| Cannon a wave | AV dissociation → RA contracts against closed tricuspid valve; identifies ventricular tachycardia |
| Absent a wave | Atrial fibrillation |
| Prominent v wave + rapid y descent | Tricuspid regurgitation (TR); severe TR → "ventriculararized" waveform |
| Blunted/slow y descent | Obstruction to RV inflow: tricuspid stenosis, pericardial tamponade |
| Kussmaul's sign | Rise or failure to fall in JVP with inspiration → classically constrictive pericarditis; also: restrictive cardiomyopathy, massive PE, RV infarction, advanced LV failure |
Special Maneuvers
Abdominojugular Reflux (Hepatojugular Reflux)
- Apply firm continuous pressure over the RUQ for >15 seconds.
- Positive = sustained rise in JVP by >3 cm.
- Assess after 10 seconds to allow respiratory artifacts to settle. Patient must not hold breath or Valsalva.
- Predicts pulmonary artery wedge pressure >15 mmHg in heart failure.
PART 2: Murmur Examination
Systematic Approach to Any Murmur
Evaluate each murmur for these 8 attributes:
- Timing — systolic, diastolic, or continuous
- Duration — early, mid, late, or holo (pan)
- Intensity — graded I–VI
- Quality — harsh, blowing, rumbling, musical
- Frequency — high, medium, low pitched
- Configuration — crescendo, decrescendo, crescendo-decrescendo (diamond), plateau
- Location — where it is loudest (aortic, pulmonary, tricuspid, mitral areas)
- Radiation — where it transmits to
Grading of Murmur Intensity (Levine Scale)
| Grade | Description |
|---|---|
| I/VI | Barely audible, only with intense concentration |
| II/VI | Soft but easily heard |
| III/VI | Moderately loud, no thrill |
| IV/VI | Loud + palpable thrill |
| V/VI | Very loud, heard with stethoscope partially off chest |
| VI/VI | Audible without stethoscope |
Systolic Murmurs
| Type | Timing | Typical Cause | Key Features |
|---|---|---|---|
| Ejection (midsystolic) | Starts after S1, ends before S2 | Aortic stenosis (AS), pulmonary stenosis (PS), flow murmur | Crescendo-decrescendo (diamond shape) |
| Holosystolic (pansystolic) | Begins with S1, ends at S2 | MR, TR, VSD | Plateau; no gap |
| Late systolic | Mid-to-late systole | Mitral valve prolapse (MVP) | Preceded by click |
Aortic Stenosis specifics: Coarse crescendo-decrescendo murmur at RUSB, radiates to carotids. In severe AS: parvus et tardus pulse (slow-rising, low-volume). Soft murmur does not exclude severe AS in low-output states.
Diastolic Murmurs
| Type | Timing | Cause | Features |
|---|---|---|---|
| Early diastolic (decrescendo) | Immediately after S2 | Aortic regurgitation (AR), pulmonary regurgitation (PR) | High-pitched, blowing |
| Mid-to-late diastolic (rumble) | After OS or S3 | Mitral stenosis (MS) | Low-pitched, rumbling; heard at apex with bell |
All diastolic murmurs are pathological and warrant further investigation.
Continuous Murmurs
- Heard throughout systole and diastole.
- Classic cause: Patent ductus arteriosus (PDA) — "machinery" murmur.
When to Order Echocardiography
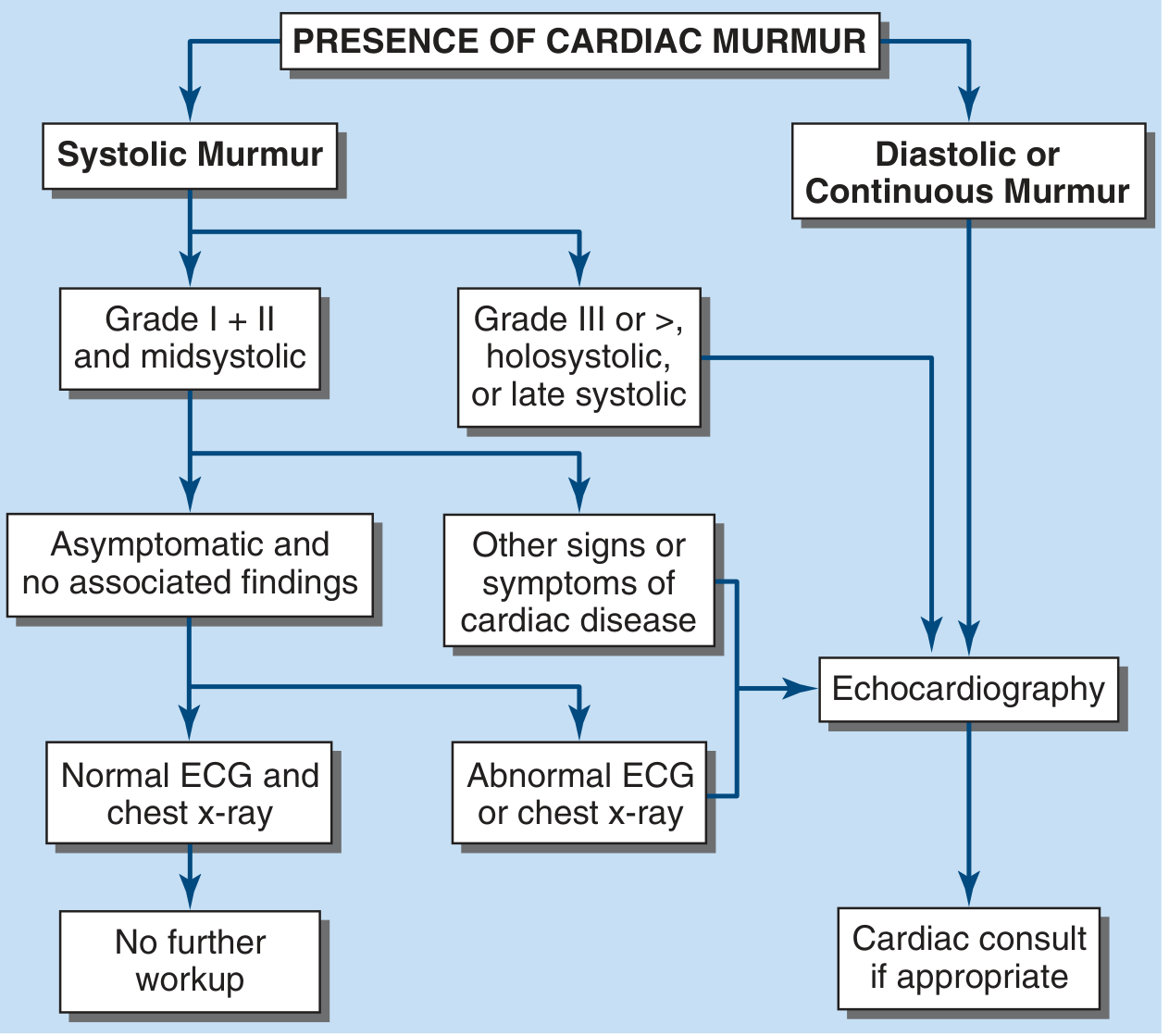
- No further workup needed: Asymptomatic, Grade I–II midsystolic murmur, normal ECG and CXR, no other cardiac findings.
- Echo indicated: Grade ≥III/VI, holosystolic or late systolic murmur, any diastolic or continuous murmur, or any systolic murmur with abnormal ECG/CXR or symptoms of heart disease.
Maneuvers to Characterize Murmurs
| Maneuver | Effect on murmur | Clinical use |
|---|---|---|
| Valsalva (strain phase) | ↓ most murmurs; ↑ HCM, MVP | Distinguishes HCM from AS |
| Standing | ↓ most murmurs; ↑ HCM, MVP | |
| Squatting / passive leg raise | ↑ most murmurs; ↓ HCM, MVP | |
| Handgrip | ↑ MR, AR, VSD; ↓ AS, HCM | Increases afterload |
| Inspiration | ↑ right-sided murmurs (TR, PR) — Carvallo's sign | |
| Expiration | ↑ left-sided murmurs |
Clinical Pearls
- A prominent JVP + holosystolic murmur at the lower sternal border louder on inspiration = tricuspid regurgitation.
- Elevated JVP + S3 gallop + mitral regurgitation murmur = decompensated heart failure.
- Cannon a waves in the neck during a wide-complex tachycardia → the rhythm is ventricular tachycardia.
- Kussmaul's sign + distant heart sounds + pulsus paradoxus = pericardial tamponade or constrictive pericarditis — do not miss.
— Harrison's Principles of Internal Medicine, 22nd ed. | Fuster & Hurst's The Heart, 15th ed.
Respiratory examination : Auscultation and percussion
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
I have excellent, comprehensive content from both sources. Let me now synthesize the full answer.
Respiratory Examination: Auscultation & Percussion
— Murray & Nadel's Textbook of Respiratory Medicine, 7th ed. | Harrison's Principles of Internal Medicine, 22nd ed.
PART 1: Percussion
Technique
Skillful percussion depends on:
- A uniform, free, easy stroke of the striking finger (plexor) striking the finger being struck (pleximeter).
- The ability to sense minor changes in pitch — the note is not just heard but predominantly felt.
- Always compare symmetrically — left vs. right at the same level.
- Percuss from top to bottom, both anteriorly and posteriorly.
Percussion Notes & Their Meanings
| Note | Quality | Clinical Meaning |
|---|---|---|
| Resonant | Normal, hollow sound | Normal air-containing lung |
| Hyper-resonant | Louder, booming | Pneumothorax, emphysema (air-trapping) |
| Tympanitic | Drum-like | Tension pneumothorax |
| Dull | Low-intensity, short duration, relatively high pitch | Pleural effusion, consolidation (pneumonia), collapse |
| Flat | No resonance (like percussing the liver) | Massive effusion completely below the fluid level |
Three Tonal Zones in Large Pleural Effusion
Percussing a large pleural effusion from top to bottom reveals:
- Resonant — above the fluid (normal lung)
- Dull — at the level of the fluid
- Flat — completely below the fluid level (maximum attenuation)
Pneumothorax vs. Pleural Effusion on Percussion
| Condition | Percussion | Breath Sounds | Tactile Fremitus |
|---|---|---|---|
| Pneumothorax | Hyper-resonant / tympanitic | Absent | Decreased/absent |
| Pleural effusion | Dull | Absent/reduced | Decreased/absent |
| Consolidation | Dull | Bronchial (loud, harsh) | Increased |
Diaphragm Excursion
- Percuss down the posterior chest during full inspiration, then full expiration.
- Mark the level of resonance-to-dullness transition each time.
- Normal excursion: ~5–7 cm.
- Reduced excursion: hyperinflation (COPD), pleural effusion, diaphragmatic paralysis.
PART 2: Auscultation
How to Auscultate
- Use both the diaphragm (high-pitched sounds) and bell (low-pitched sounds).
- Auscultate systematically: compare left vs. right at each level (apex, mid-zones, bases), anteriorly and posteriorly.
- Instruct the patient to breathe deeply through the mouth.
Normal Breath Sounds
| Sound | Location | Character |
|---|---|---|
| Vesicular | Most of the lung fields | Soft, low-pitched; inspiratory > expiratory; no gap between phases |
| Bronchial | Over the trachea/manubrium | Loud, harsh, high-pitched; expiratory > inspiratory; gap between phases |
| Bronchovesicular | 1st/2nd intercostal spaces anteriorly, between scapulae | Intermediate in character |
Bronchial breath sounds heard over peripheral lung = pathological → consolidation (fluid-filled alveoli transmit sound well).
Abnormal Breath Sounds (Added Sounds)
1. Crackles (Rales)
- Discontinuous, non-musical sounds.
- Caused by sudden opening of collapsed or fluid-filled airways/alveoli.
| Type | Sound | Cause |
|---|---|---|
| Fine crackles (end-inspiratory) | Velcro-like ripping apart | Pulmonary fibrosis (IPF), early pulmonary oedema |
| Coarse/wet crackles (pan-inspiratory or expiratory) | Bubbly, lower-pitched | Pulmonary oedema, pneumonia, bronchiectasis |
- Crackles in pulmonary oedema: predominantly bibasal.
- Crackles in IPF: described as "Velcro" — dry, fine, end-inspiratory, bibasal.
- Note: "Wet" vs. "dry" crackles distinction has not been shown to reliably differentiate etiologies — do not rely on this alone.
2. Wheeze
- Continuous, musical, high-pitched — generated by turbulent airflow through narrowed airways.
- Predominantly expiratory, but can be biphasic.
| Type | Meaning |
|---|---|
| Polyphonic wheeze (multiple pitches) | Widespread small airway obstruction → asthma, cardiac asthma (pulmonary oedema) |
| Monophonic wheeze (single pitch) | Fixed obstruction of a single airway → bronchogenic carcinoma, foreign body |
Not all wheeze = asthma. Peribronchial oedema in congestive heart failure also causes diffuse wheeze ("cardiac asthma").
3. Rhonchi
- Low-pitched, continuous, snoring/gurgling sounds.
- Caused by secretions in medium-sized airways.
- Acute: viral/bacterial bronchitis.
- Chronic: bronchiectasis, COPD.
- Clear partially or completely with coughing (distinguishes from wheeze).
4. Stridor
- High-pitched, focal, inspiratory wheeze — best heard over the neck.
- Indicates upper airway obstruction (larynx, trachea).
- Causes: croup, epiglottitis, foreign body, laryngeal tumour.
- Stridor is an emergency until proven otherwise.
5. Pleural Rub
- Creaking, grating sound — like leather rubbing on leather.
- Heard in both inspiration and expiration.
- Caused by inflamed pleural surfaces rubbing together.
- Indicates pleuritis (pneumonia, PE, TB, malignancy).
- Disappears when effusion develops (fluid separates the surfaces).
Vocal Resonance Tests
These tests distinguish consolidation from effusion when breath sounds are diminished:
| Test | How | Consolidation | Effusion/Pneumothorax |
|---|---|---|---|
| Vocal fremitus (palpation) | Patient says "99" while examiner feels chest | Increased | Decreased |
| Vocal resonance (auscultation) | Patient says "99" through stethoscope | Increased/bronchophony | Decreased |
| Egophony | Patient says "EEE" — heard as "AYY" | Present (E→A change) | Absent |
| Whispered pectoriloquy | Whisper "1-2-3" — clearly heard | Present | Absent |
Egophony (E→A change) = abnormal sound transmission through consolidated parenchyma → present in pneumonia, absent in IPF and effusion. Extremely useful to distinguish causes of crackles.
Diminished/Absent Breath Sounds
| Cause | Other Clues |
|---|---|
| Emphysema | Diffusely quiet chest, barrel chest, prolonged expiration, hyper-resonant |
| Pleural effusion | Dull to percussion, ↓ fremitus, stony dullness |
| Pneumothorax | Hyper-resonant, tracheal deviation (tension), ↓ fremitus |
| Pleural thickening | History of TB, asbestosis |
Clinical Summary Table
| Finding | Percussion | Breath Sounds | Added Sounds | Fremitus |
|---|---|---|---|---|
| Normal | Resonant | Vesicular | None | Normal |
| Consolidation | Dull | Bronchial | Fine crackles | ↑ Increased |
| Pleural effusion | Stony dull | Absent/reduced | None (± rub early) | ↓ Decreased |
| Pneumothorax | Hyper-resonant | Absent | None | ↓ Decreased |
| Asthma/COPD | Hyper-resonant | ↓ Vesicular | Wheeze, rhonchi | Normal/↓ |
| Pulmonary fibrosis | Resonant | Vesicular | Fine "Velcro" crackles | Normal |
| Pulmonary oedema | Resonant → dull at bases | Vesicular | Bibasal crackles ± wheeze | Normal |
| Pleuritis | Resonant | Normal | Pleural rub | Normal |
Clinical Pearls
- Always auscultate before percussion is not mandatory in chest exam (unlike abdomen), but systematically cover all zones.
- Pulsus paradoxus — exaggerated fall in systolic BP >10 mmHg on inspiration — is an ominous sign in obstructive lung disease, indicating significant negative intrathoracic pressures and impending respiratory failure.
- JVD + peripheral oedema in a respiratory patient → cor pulmonale from chronic hypoxia.
- A unilateral silent chest in a breathless patient = pneumothorax or massive effusion until proven otherwise — act urgently.
— Murray & Nadel's Textbook of Respiratory Medicine, 7th ed. | Harrison's Principles of Internal Medicine, 22nd ed.
This is a shared conversation. Sign in to Orris to start your own chat.