
IMG-20260526-WA0293.jpg
What Happened With Both Lungs
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
I now have enough information for a thorough analysis. Here is my full interpretation:
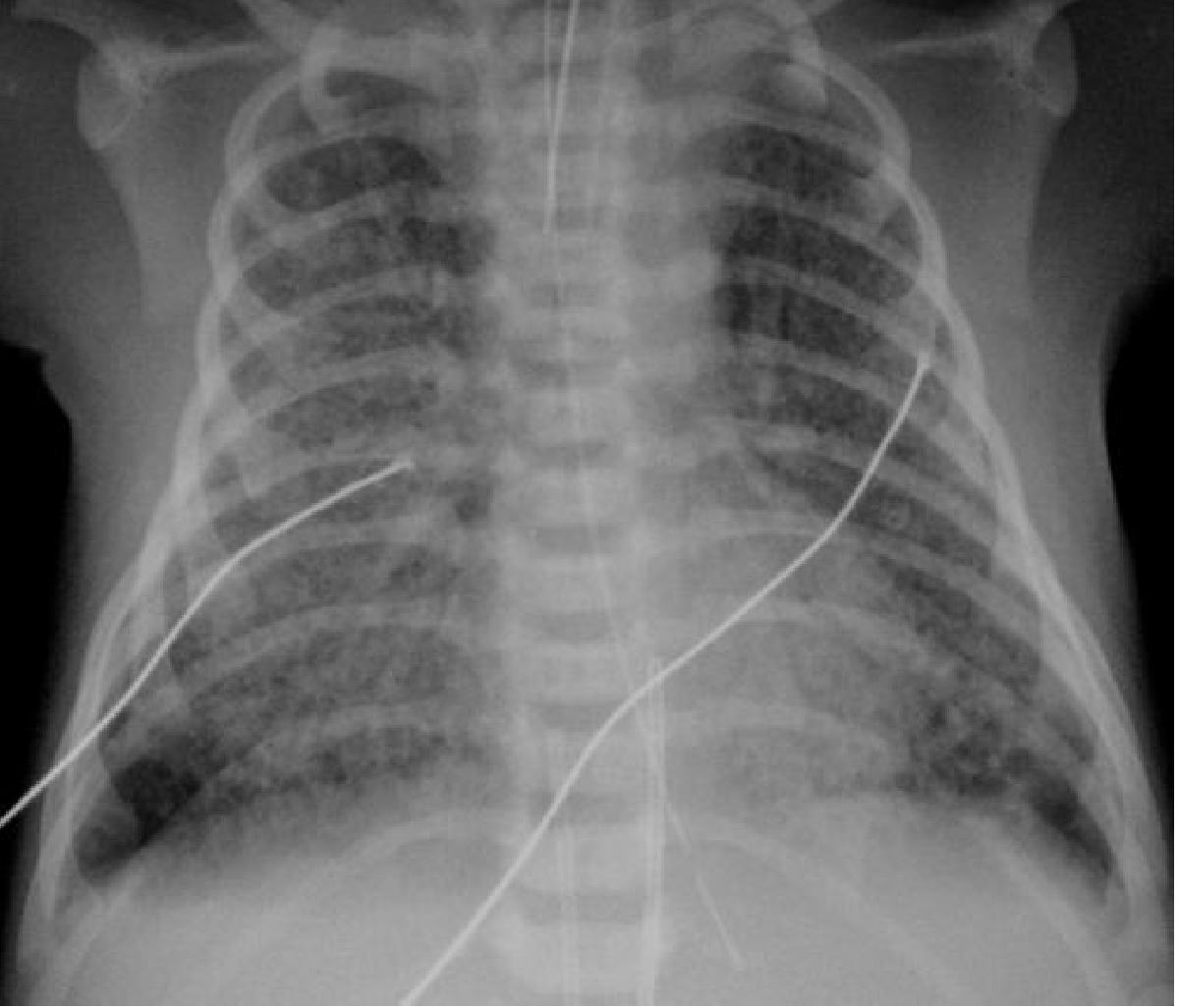
Chest X-Ray Analysis - B/O Ayesha (Pediatric/Neonatal CXR, PA View)
Important disclaimer: This is an educational interpretation only. Formal radiological reporting must be done by a qualified radiologist with full clinical context.
Key Radiological Findings
Looking carefully at the X-ray, here is what stands out in both lungs:
| Finding | Description |
|---|---|
| Bilateral hyperinflation | Both lung fields are excessively dark (black), indicating air trapping. The ribs are spread horizontally (barrel chest appearance) and the diaphragm appears flattened |
| Increased bronchial markings | Prominent perihilar markings (peribronchial thickening) visible in both lung fields, giving a "dirty chest" appearance |
| Bilateral interstitial infiltrates | Increased haziness/streakiness throughout both lungs, most visible in the perihilar regions |
| Flattened diaphragm | A hallmark of air trapping - the diaphragm is pushed downward |
| No focal consolidation | No dense lobar opacity to suggest bacterial pneumonia |
| Heart not clearly displaced | Mediastinum appears central |
The Primary Differential for These Bilateral Findings
1. Bronchiolitis (Most Likely)
- The classic CXR picture of bilateral hyperinflation + peribronchial thickening in an infant is bronchiolitis (most commonly RSV - Respiratory Syncytial Virus)
- Presents with bilateral air-trapping due to small airway obstruction
- The lungs look overinflated because air gets trapped behind mucus plugs in inflamed bronchioles
2. Viral Pneumonia / Chlamydial Pneumonia
- Chlamydial pneumonia in infants shows bilateral symmetric interstitial infiltrates with hyperinflation, exactly as seen here
- Per Rosen's Emergency Medicine: "Chest radiograph usually shows hyperinflation with bilateral and symmetric, diffuse, interstitial infiltrates"
3. Transient Tachypnoea of the Newborn (TTN) - if this is a neonate
- Shows mild overinflation, prominent blood vessels, perihilar interstitial shadowing
- Per Grainger & Allison's Diagnostic Radiology: "the most common appearances are mild overinflation, prominent blood vessels, perihilar interstitial shadowing and fluid in the transverse fissure"
- Usually resolves within 24-48 hours
4. Meconium Aspiration Syndrome (MAS) - if post-term neonate
- Shows bilateral hyperinflation + asymmetrical coarse opacification
- Textbook reference image (below) for comparison:
Summary of What's Happening to Both Lungs
The bilateral lung findings in this CXR indicate air trapping with diffuse small airway disease - both lungs are overinflated and show increased interstitial markings. The most likely diagnoses in a young infant (B/O Ayesha = baby of a mother named Ayesha, suggesting a newborn or young infant) are:
- Bronchiolitis (if infant >1 month) - viral inflammation of small airways causing bilateral air trapping
- Viral/Chlamydial pneumonia - bilateral symmetric interstitial disease
- TTN or MAS - if this is a neonate in the first few days of life
The key clinical next steps would be:
-
Clinical history: age of baby, gestational age, onset of symptoms, feeding difficulties, fever
-
O2 saturation and work of breathing assessment
-
Nasopharyngeal swab for RSV/viral panel if bronchiolitis is suspected
-
Supportive care is the mainstay (oxygen supplementation, hydration)
-
Grainger & Allison's Diagnostic Radiology, neonatal chest section
-
Rosen's Emergency Medicine, pediatric respiratory section
This is a shared conversation. Sign in to Orris to start your own chat.