Thyroiditis in detail
Reading File
Finding Sources
Searching PubMed
thyroiditis classification management
Searching Images
thyroiditis histology types
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive material from Harrison's, Robbins (both editions), Goldman-Cecil, and Tietz, plus three excellent images. I'll compile the full detailed answer.
Thyroiditis — A Comprehensive Overview
Thyroiditis encompasses a diverse group of disorders characterized by thyroid inflammation. They are classified by onset and duration (acute/subacute/chronic), presence or absence of pain, and underlying etiology (autoimmune, infectious, drug-induced, post-radiation). — Harrison's Principles of Internal Medicine 22E
Classification
| Category | Type | Key Feature |
|---|---|---|
| Acute | Suppurative / radiation / drug-induced | Bacterial/fungal infection, acute pain, fever |
| Subacute | De Quervain's (granulomatous) | Painful, post-viral, transient thyrotoxicosis |
| Subacute | Silent / postpartum (lymphocytic) | Painless, autoimmune, transient thyrotoxicosis |
| Chronic | Hashimoto's (autoimmune) | Most common; goiter → hypothyroidism |
| Chronic | Riedel's thyroiditis | Rare; invasive fibrosis |
| Chronic | Drug-induced | Amiodarone, IFN, checkpoint inhibitors, TKIs |
1. Acute (Suppurative) Thyroiditis
Etiology & Pathogenesis
Rare. Caused by bacterial infection (Staphylococcus, Streptococcus, Enterobacter) or fungal organisms (Aspergillus, Candida, Coccidioides, Histoplasma, Pneumocystis — particularly in immunocompromised patients). In children and young adults, the most common predisposing cause is a piriform sinus fistula (remnant of the 4th branchial pouch), predominantly left-sided. In the elderly, risk factors include long-standing goiter and degeneration in thyroid malignancy. — Harrison's 22E
Clinical Features
- Thyroid pain, often referred to throat or ears
- Small, tender, possibly asymmetric goiter
- Fever, dysphagia, erythema over thyroid
- Cervical lymphadenopathy
- Thyroid function usually normal
Investigations
- ↑ ESR, ↑ WBC
- FNA: polymorphonuclear leukocyte infiltration; culture identifies organism
- CT/ultrasound: localizes abscess
Complications
Tracheal obstruction, septicemia, retropharyngeal abscess, mediastinitis, jugular venous thrombosis — uncommon with prompt antibiotics.
Treatment
- Antibiotics guided by Gram stain and culture
- Surgical drainage if abscess forms
2. Subacute (De Quervain's / Granulomatous / Viral) Thyroiditis
Etiology
The most common cause of a painful thyroid in outpatient practice. Multiple viruses implicated: mumps, coxsackie, influenza, adenoviruses, echoviruses, and SARS-CoV-2 (including post-COVID-vaccine cases). Peak incidence: 30–50 years; women 3× more commonly than men. — Harrison's 22E
Pathophysiology
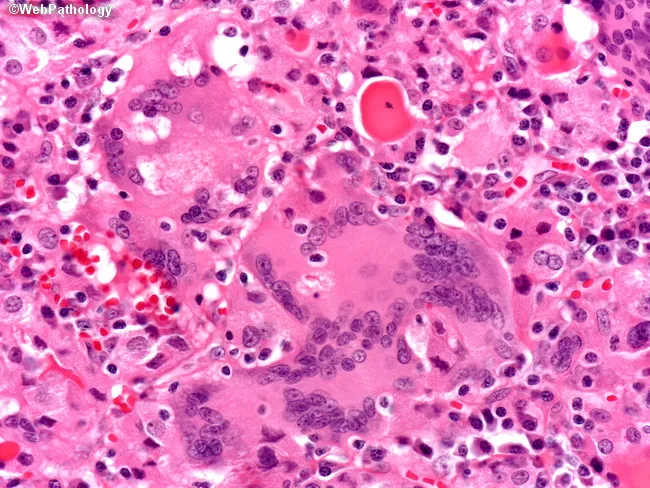
Characteristic patchy inflammatory infiltrate with disruption of thyroid follicles and multinucleated giant cells within follicles → granulomas with fibrosis → eventual return to normal.
The sequence of thyroid function changes:
- Thyrotoxic phase: Follicular destruction → release of stored T4 and T3 → ↑ T4/T3, suppressed TSH, low/absent radioiodine uptake (<5%)
- Hypothyroid phase: Stored hormone depleted → ↓ free T4, ↑ TSH
- Recovery phase: T4/T3/TSH return to normal over ~6 months
The T4:T3 ratio during thyrotoxic phase is lower than in Graves' disease (where T3 is disproportionately elevated), reflecting passive hormone release rather than synthesis.
Clinical Course
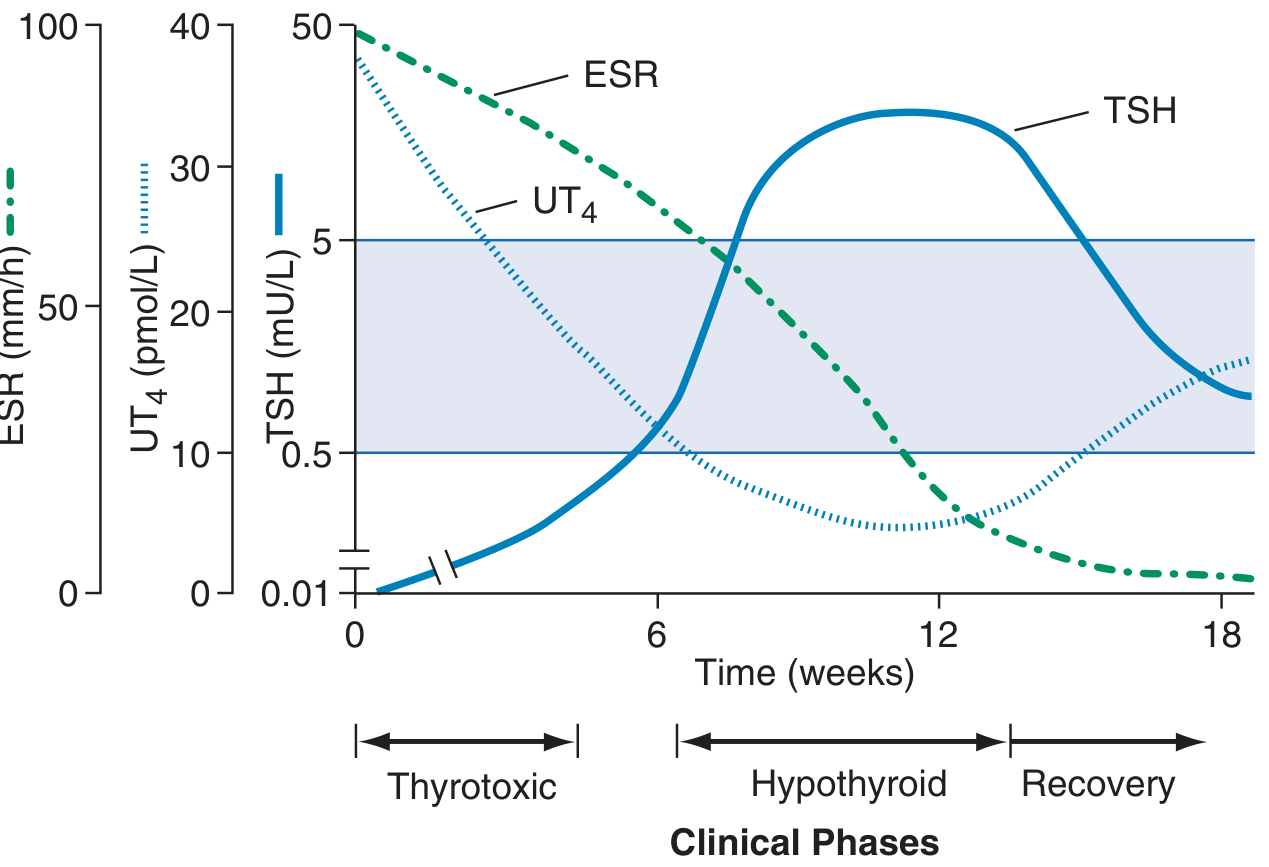
Clinical phases of subacute thyroiditis. During the thyrotoxic phase, UT4 is elevated and TSH is suppressed. ESR peaks early and declines with inflammation. The hypothyroid phase follows as hormone stores are depleted, with TSH rising above normal, before eventual recovery. — Harrison's 22E
- Painful, enlarged thyroid (exquisitely tender); pain referred to jaw or ear
- Malaise, preceding URI symptoms
- Fever and features of thyrotoxicosis/hypothyroidism depending on phase
- Permanent hypothyroidism in ~15%, especially those with underlying thyroid autoimmunity
Investigations
- ↑ ESR (hallmark — often very high), ↑ T4/T3, suppressed TSH (thyrotoxic phase)
- Radioiodine uptake: very low (<5%) during thyrotoxic phase
- Thyroid antibodies: negative (distinguishes from Hashimoto's)
- FNA: granulomatous inflammation with giant cells (if needed)
Histology
Treatment
- Mild-moderate: Aspirin 600 mg every 4–6 h or NSAIDs (+ PPI for gastroprotection)
- Severe or inadequate response: Prednisone 15–40 mg/day, tapered over 6–8 weeks guided by symptom and ESR response
- Thyrotoxic symptoms: β-blockers (propranolol) — antithyroid drugs are NOT effective (no excess synthesis)
- Hypothyroid phase: Levothyroxine if symptomatic; usually temporary
3. Hashimoto's Thyroiditis (Chronic Autoimmune / Chronic Lymphocytic Thyroiditis)
Epidemiology
Most common cause of hypothyroidism in iodine-sufficient regions. Most prevalent between 45–65 years. Female:male ratio 10:1 to 20:1. First described by Hakaru Hashimoto in 1912 ("struma lymphomatosa"). — Robbins & Cotran Pathologic Basis of Disease; Tietz Lab Medicine
Pathogenesis
Breakdown of self-tolerance to thyroid autoantigens (thyroglobulin, thyroid peroxidase). Strong genetic component with polymorphisms in:
- CTLA4 (cytotoxic T lymphocyte-associated antigen-4)
- PTPN22 (protein tyrosine phosphatase non-receptor type 22)
- IL2RA (IL-2 receptor α chain)
These are regulators of T-cell responses. Environmental risk factors include smoking, iodine excess, selenium deficiency, and infections. — Robbins & Cotran
Multiple immune mechanisms drive thyroid cell death:
- CD8+ cytotoxic T cell–mediated destruction of follicular cells
- Cytokine-mediated injury: CD4+ Th1 cells → IFN-γ → macrophage recruitment and follicular damage
- Antibody-mediated mechanisms: Anti-TPO and anti-thyroglobulin antibodies → complement-dependent or ADCC-mediated injury (role still debated — may be consequence as well as cause)
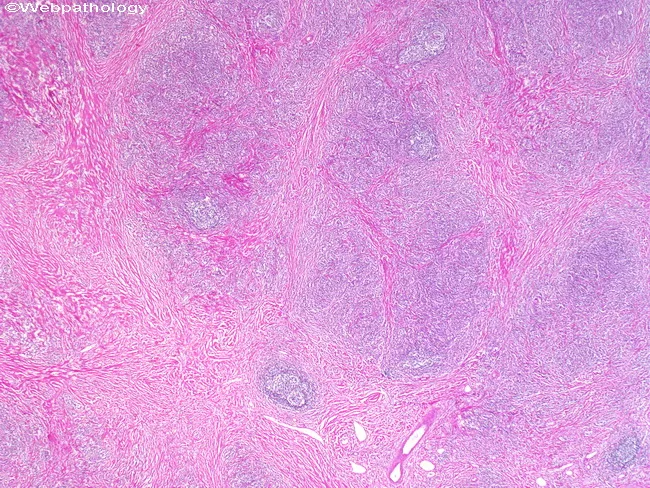
Morphology
- Thyroid diffusely enlarged, well-demarcated, pale yellow-tan and firm on cut surface
- Extensive lymphoplasmacytic infiltrate with prominent germinal centers
- Hürthle cell (oncocyte) change: follicular epithelium replaced by cells with abundant eosinophilic, granular cytoplasm — a metaplastic response to chronic injury
- Atrophic follicles in advanced disease
- With progression: fibrosis (fibrous variant ~10–12% of cases — dense hyalinized stroma with residual follicular islands; capsule intact, distinguishing it from Riedel's)
Clinical Features
- Goiter: usually firm, symmetric, non-tender; may be lobulated
- Gradual onset of hypothyroidism: fatigue, weight gain, cold intolerance, constipation, dry skin, bradycardia, myxedema
- Can pass through transient thyrotoxicosis ("Hashitoxicosis") early in disease
- Progresses from euthyroid → subclinical hypothyroidism → overt hypothyroidism
- Associated with other autoimmune diseases: type 1 diabetes, SLE, RA, Sjögren syndrome, pernicious anemia, Addison's disease
Investigations
- Anti-TPO antibodies: positive in ~90% (most sensitive marker)
- Anti-thyroglobulin antibodies: positive in 20–50%
- TSH, free T4: depends on phase (may be normal, ↑ TSH with normal T4 in subclinical, or ↑ TSH + ↓ T4 in overt hypothyroidism)
- Thyroid ultrasound: hypoechoic and heterogeneous parenchyma
- Radioiodine uptake: variable (elevated if TSH is high, low in destructive phase)
Treatment
- Overt hypothyroidism: Levothyroxine (goal: normalize TSH to 0.5–2.5 mU/L)
- Subclinical hypothyroidism with high antibody titers: levothyroxine recommended
- Goiter reduction: short-term TSH-suppressing doses may reduce goiter size
- Monitoring: serial TSH; lifelong follow-up needed
Complications & Associated Malignancy
- Primary B-cell lymphoma of the thyroid (MALT lymphoma): rare but well-established risk from prolonged intrathyroidal B-cell stimulation
- Papillary thyroid carcinoma: increased frequency, particularly in women
- FNA biopsy indicated for suspicious nodules
4. Silent (Painless) Thyroiditis & Postpartum Thyroiditis
Overview
Both are variants of destructive autoimmune thyroiditis, essentially the same disorder — distinguished only by timing: postpartum thyroiditis occurs in the first 12 months after delivery. — Goldman-Cecil Medicine; Tietz
Epidemiology
- Postpartum thyroiditis: up to 10% of pregnancies; ~20× more common than Graves' in postpartum period; risk ↑ with positive anti-TPO in first trimester, personal/family history of autoimmunity
- Sporadic painless thyroiditis: less common; ages 30–60; slightly more common in women (1.5:1)
- 50% of anti-TPO positive women in first trimester will develop postpartum thyroiditis
Clinical Phases
Classic triphasic pattern (experienced by ~20% of postpartum cases):
- Thyrotoxic phase (1–3 months): palpitations, tachycardia, heat intolerance; non-tender goiter; symptoms milder than Graves'
- Euthyroid interlude (1–2 months)
- Hypothyroid phase (up to 12 months): fatigue, cold intolerance, constipation
~50% experience only hypothyroidism; ~30% only thyrotoxicosis.
Key Distinguishing Features from Graves' Disease
| Feature | Silent/Postpartum Thyroiditis | Graves' Disease |
|---|---|---|
| Thyroid pain | Absent | Absent |
| Goiter | Non-tender | Non-tender, with bruit |
| Ophthalmopathy/dermopathy | Absent | Present |
| T3:T4 ratio | <20 (passive release) | T3 preferentially elevated |
| RAIU | Low/undetectable | High |
| TRAb | Negative | Positive |
| Anti-TPO | Usually positive | Often positive |
| Color Doppler | ↓ flow | ↑ flow |
Treatment
- Thyrotoxic phase: β-blockers if symptomatic; antithyroid drugs are contraindicated (no excess synthesis)
- Hypothyroid phase: Levothyroxine if TSH >10 mIU/L or symptomatic
- Women with history of postpartum thyroiditis: annual TSH measurement (↑ risk of permanent hypothyroidism — up to 30–50% at 1 year remain hypothyroid)
5. Drug-Induced Thyroiditis
Several drugs can cause thyroiditis, presenting as subacute or chronic disease:
| Drug | Pattern |
|---|---|
| Amiodarone | Type 1 (iodine-induced hyperthyroidism) or Type 2 (destructive thyroiditis) |
| Interferon-α | Autoimmune or destructive thyroiditis |
| Tyrosine kinase inhibitors | Hypothyroidism or destructive thyroiditis |
| Immune checkpoint inhibitors (anti-PD-1, anti-CTLA-4) | Autoimmune thyroiditis, hypo- or hyperthyroidism |
| Lithium | Hypothyroidism |
Amiodarone is particularly notable: it contains 37% iodine by weight and can cause thyrotoxicosis (both excess synthesis and destructive release) or hypothyroidism. Checkpoint inhibitor–induced thyroiditis is increasingly recognized as a major immune-related adverse event.
6. Riedel's Thyroiditis
Features
- Rare, fibrosing disorder of unknown etiology; now considered part of the IgG4-related disease spectrum
- Dense, keloid-like fibrosis that extends beyond the thyroid capsule into adjacent soft tissues (strap muscles, trachea, esophagus, carotid vessels) — this extracapsular invasion distinguishes it from fibrous Hashimoto's
- Thyroid is rock-hard ("iron-hard goiter"), mimicking anaplastic carcinoma
- Associated with other fibrosclerotic conditions: retroperitoneal fibrosis, orbital pseudotumor, sclerosing cholangitis
- Symptoms: compressive symptoms (dysphagia, stridor, dysphonia), hypothyroidism
- Treatment: glucocorticoids, tamoxifen; surgical release for tracheal compression; thyroid hormone replacement
Key Differential Diagnosis Summary
| Parameter | De Quervain's | Hashimoto's | Postpartum | Acute Suppurative | Riedel's |
|---|---|---|---|---|---|
| Pain | Yes | No | No | Yes (severe) | No |
| Fever | Mild-mod | No | No | High | No |
| Thyrotoxicosis | Transient | Occasional | Transient | No | No |
| Hypothyroidism | Transient | Permanent | Often transient | No | Variable |
| Anti-TPO | Negative | Positive (90%) | Positive | Negative | Negative |
| ESR | Very high | Normal/mild↑ | Normal | ↑ | Normal |
| RAIU | Very low | Variable | Very low | Normal | Normal/low |
| Histology | Granulomas, giant cells | Lymphoid follicles, Hürthle cells | Lymphocytic | PMN infiltrate | Dense fibrosis |
References
- Harrison's Principles of Internal Medicine 22E, pp. 3081–3082
- Robbins & Cotran Pathologic Basis of Disease, pp. 998–1001
- Robbins & Kumar Basic Pathology, p. 3184–3192
- Goldman-Cecil Medicine (International Edition), pp. 3102–3135
- Tietz Textbook of Laboratory Medicine 7E, pp. 3870–3936
This is a shared conversation. Sign in to Orris to start your own chat.