Sinonasal tumor surgery in detail
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching PubMed
sinonasal tumor endoscopic surgery outcomes
Reading File
Reading File
Loading Image
Here is a detailed, textbook-grounded overview of sinonasal tumor surgery.
Sinonasal Tumor Surgery
1. Tumor Classification and Histology
Sinonasal tumors span a wide biological spectrum and dictate surgical strategy:
Benign tumors
- Schneiderian (sinonasal) papilloma - the most common benign nasal cavity tumor. Three subtypes: septal (exophytic, no malignant risk), inverted (most common, ~10-15% malignant transformation, arises lateral nasal wall), and cylindrical cell/oncocytic (rarest, equal or slightly higher malignant risk than inverted).
- Fibro-osseous lesions - fibrous dysplasia, ossifying fibroma, osteoma.
- Vascular lesions - hemangioma.
- Encephaloceles / meningoceles / pituitary extensions - intracranial tissue extending into the nasal cavity through skull base defects.
Malignant tumors
-
Squamous cell carcinoma (SCC) - most common sinonasal malignancy.
-
Adenocarcinoma - associated with woodworking dust exposure; low vs. high grade behavior differs.
-
Esthesioneuroblastoma (olfactory neuroblastoma) - neuroectodermal origin from olfactory epithelium; <5% of paranasal sinus malignancies; staged by Kadish system (A: nasal cavity only; B: paranasal sinus extension; C: beyond sinuses; D: nodal/distant mets); cervical metastases in 20-25%.
-
Sinonasal undifferentiated carcinoma (SNUC) - aggressive, >80% present as T4; 5-year OS 22-43%, distant mets in 65%.
-
Adenoid cystic carcinoma - high propensity for perineural spread and bone invasion.
-
Mucosal melanoma - all lesions are T3/Stage III at minimum; 5-year OS 25-42%.
-
Neuroendocrine carcinoma - poor prognosis, rare cure without aggressive multimodal therapy.
-
Rhabdomyosarcoma - most common pediatric paranasal sinus malignancy.
-
Lymphoma - surgery limited to biopsy only.
-
Cummings Otolaryngology, Ch. 20; K J Lee's Essential Otolaryngology, p. 598-599
2. Preoperative Evaluation and Staging
Imaging
- CT - defines bony anatomy and identifies bony destruction; essential for surgical planning.
- MRI - better for soft tissue extent; T2-weighted sequences differentiate tumor from obstructed secretions (inflammatory signal is T2 bright; tumor is lower T2). Identifies intracranial connections, orbital involvement, and cranial nerve encasement.
- Both modalities are complementary and should be obtained together.
Ohngren's Line
A theoretical plane connecting the medial canthus of the eye with the angle of the mandible. Tumors antero-inferior to this plane carry a better prognosis (more accessible surgically, less likely to involve the skull base and orbit).
AJCC Staging (Paranasal Sinuses)
Maxillary sinus:
| T stage | Description |
|---|---|
| T1 | Tumor limited to sinus mucosa, no bone involvement |
| T2 | Erosion of bone including hard palate/middle meatus |
| T3 | Posterior maxillary wall, orbital floor/medial wall, subcutaneous tissue, pterygoid fossa, ethmoids |
| T4a | Anterior orbital contents, facial skin, pterygoid plates, infratemporal fossa, cribriform plate, sphenoid/frontal sinuses |
| T4b | Orbital apex, dura, brain, middle cranial fossa, CNs other than V2, nasopharynx, clivus |
Nasal cavity and ethmoid sinus:
| T stage | Description |
|---|---|
| T1 | One subsite, with or without bony invasion |
| T2 | Two adjacent subsites or adjacent region in nasoethmoidal complex |
| T3 | Medial orbital wall/floor, maxillary sinus, palate, cribriform plate |
| T4a | Anterior orbit, facial skin, minimal anterior cranial fossa, pterygoid plates, sphenoid/frontal sinuses |
| T4b | Orbital apex, dura, brain, middle cranial fossa, CNs other than V2, nasopharynx, clivus |
N and M staging follow standard head and neck SCC criteria.
- K J Lee's Essential Otolaryngology, p. 597-598
Prognostic Factors
- Histological subtype (worst: mucosal melanoma; best: minor salivary gland tumors, low-grade sarcomas)
- T stage and intracranial involvement
- Resection margins (most direct determinant of survival)
- Prior radiation / incomplete prior resection
- Nodal disease and distant metastasis
3. Surgical Approaches
The choice of approach is governed by tumor location, size, extent, histology, and the need for en-bloc vs. piecemeal resection.
3A. Open (Transfacial) Approaches
Lateral Rhinotomy
The foundational open approach. An incision connects three surface points: (1) midway between nasion and medial canthus, (2) at the start of the alar crease, and (3) at the columella base. It provides adequate exposure for medial maxillectomy. Extensions include:
- Lip-splitting extension (Weber-Fergusson) - adds exposure of the maxilla and orbit, permits total maxillectomy.
- Lynch-type extension - upward toward the orbit.
- Weber-Fergusson incision - incorporates lip-splitting and subciliary incisions into lateral rhinotomy for maximal maxillary exposure.
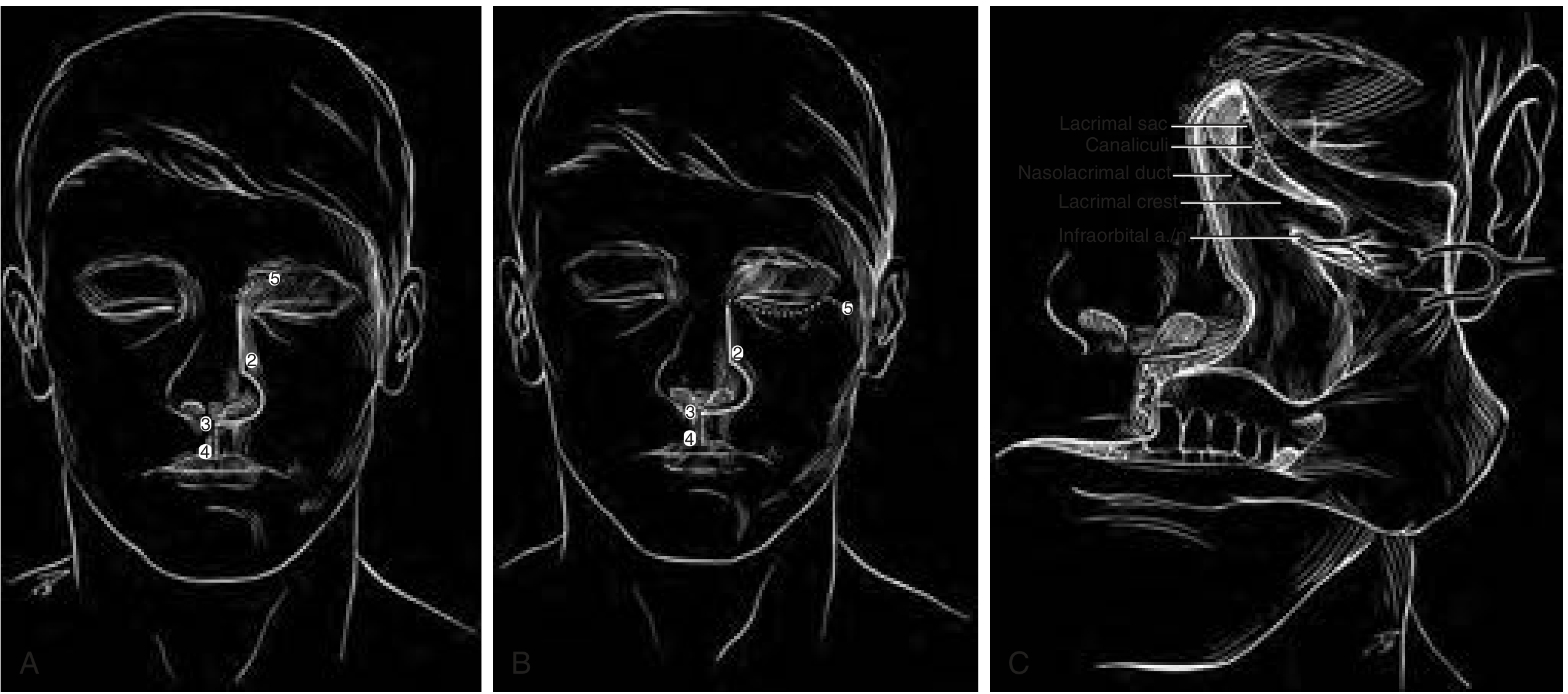
Lateral rhinotomy with extension options. (A) Basic incision points 1-3. (B) Extended access with lip-split (points 3-4) and Lynch-type (points 1-5) extensions. (C) Subperiosteal dissection with infraorbital nerve preservation after extended lateral rhinotomy. - Cummings Otolaryngology
Medial Maxillectomy - removes medial maxillary wall with lateral nasal wall; used for tumors of the lateral nasal wall, maxillary antrum medial wall, and ethmoid sinuses.
Total / Extended Maxillectomy - removes the entire maxilla. An infrastructure maxillectomy removes the maxilla below the orbital floor; a total maxillectomy includes the orbital floor; an extended/radical maxillectomy includes the orbital contents (orbital exenteration) when tumor invades orbital fat.
Mandibulotomy (Mandibular Swing) - used when tumor deeply involves the parapharyngeal space or when safe dissection along the internal carotid artery (ICA) from its bifurcation in the neck to the temporal bone is necessary. Useful for tumors originating in the central compartment with lateral extension.
3B. Craniofacial Resection (CFR)
The historical gold standard for tumors involving or approaching the anterior skull base (e.g., esthesioneuroblastoma, sinonasal SCC with cribriform plate invasion).
- Sinonasal component: resected via a transfacial approach (lateral rhinotomy or Weber-Fergusson).
- Skull base/intracranial component: via a frontal craniotomy.
- Allows en-bloc removal of the skull base and dura.
- Provides direct access for reconstruction with a pericranial flap.
- Overall 5-year survival ~50% for sinonasal cancer.
- Mortality 4.7% (higher with comorbidities).
- Morbidity 33-36%: wound complications 20%, systemic 5%, orbital 1.5% (increased by prior radiation, dural/brain invasion).
3C. Endoscopic Endonasal Approach (EEA)
The modern preferred approach for appropriately selected lesions.
Advantages: No facial incisions, no craniotomy, no brain retraction, excellent visualization and magnification, decreased hospital stay, improved quality of life, reduced morbidity.
Expanded endonasal approaches (EEA) - developed by Kassam et al. (University of Pittsburgh, 2005) - provide access along the entire ventral skull base via modular corridors:
| Module | Access | Key pathologies |
|---|---|---|
| Transfrontal | Posterior frontal sinus table and floor | Frontal osteoma, mucocele, nasal dermoid |
| Transcribriform | Crista galli to planum sphenoidale | Olfactory groove meningioma, esthesioneuroblastoma, sinonasal tumors, CSF leak |
| Transplanum/Transtuberculum | Suprasellar region | Planum meningioma, craniopharyngioma, optic glioma |
| Transsellar | Sella turcica | Pituitary adenoma |
| Transclival | Clivus (superior/middle/inferior) | Chordoma, clival meningioma |
Surgical steps for EEA:
- Removal of posterior two-thirds of nasal septum.
- Wide sphenoidotomy with intersinus septectomy.
- Gradual debulking to identify tumor origin while preserving orientation landmarks.
- Exposure of the skull base in the relevant module.
- Dural opening if intracranial extension present.
- Tumor resection.
- Skull base reconstruction (see Section 5).
Indications for EEA in sinonasal malignancy:
- Ethmoid cancer with cribriform plate, ethmoidal roof, or lamina papyracea involvement
- Medially located frontal sinus lesions
- Small maxillary sinus lesions (medial, superior, or posterior walls)
- Sphenoid sinus lesions
- Pterygopalatine fossa invasion and limited infratemporal fossa extension
- Periorbital extension without orbital invasion
- Anterior skull base dura or olfactory bulb invasion
Contraindications to EEA:
- Nasal bone, palate, skin, or subcutaneous tissue invasion
- Massive frontal sinus involvement
- Maxillary lesions involving the lateral, anterior, or inferior walls
- Massive lacrimal pathway invasion
- Massive infratemporal fossa invasion
- Invasion of orbital contents
- Broad invasion of brain parenchyma or lateral extension over the orbit
All patients should be counseled on possible conversion to open approaches if needed for margin clearance.
- K J Lee's Essential Otolaryngology, p. 600; Cummings Otolaryngology, p. 3366-3384
4. Histology-Specific Surgical and Multimodal Protocols
| Histology | Primary Treatment | Adjuvant |
|---|---|---|
| SCC | Margin-negative resection | IMRT; elective neck RT for T3-T4 (23% locoregional met risk); platinum chemo for positive margins or lymphovascular invasion |
| Adenocarcinoma | Surgery alone for T1-2 low grade | IMRT for high-grade or T3-4; chemo for T3-4; low neck met risk (7%), elective ND uncommon |
| Esthesioneuroblastoma | Surgery + radiation | Radiosensitive; elective neck management debated (20-25% cervical mets) |
| SNUC | Neoadjuvant chemo + chemoRT or surgery + IMRT | Trimodality if tolerated; bilateral neck treatment considered (26-27% nodal disease) |
| Adenoid cystic carcinoma | Radical resection | Postop RT (IMRT or particle therapy); perineural spread mandates wide margins |
| Neuroendocrine carcinoma | Neoadjuvant etoposide/cisplatin → resection | Adjuvant IMRT |
| Soft tissue sarcoma / Ewing | Chemo ± RT (primary); surgery for nonresponders/recurrence | - |
| Lymphoma | Biopsy only (surgery limited to diagnosis) | Chemo ± RT |
| Mucosal melanoma | Surgical resection (standard of care) | IMRT debated (improves local control, not survival); immunotherapy emerging |
| Rhabdomyosarcoma | Chemotherapy primary | Surgery / RT for nonresponders |
- K J Lee's Essential Otolaryngology, p. 598-599; Cummings Otolaryngology, p. 1736
5. Skull Base Reconstruction
Reconstruction is mandatory after EEA or craniofacial resection to separate the cranial cavity from the sinonasal tract - preventing CSF leak, meningitis, and pneumocephalus.
Defect Classification
| Defect size | Preferred reconstruction |
|---|---|
| Small (<1 cm) | Acellular/non-vascularized grafts |
| Medium (1-3 cm) | Local vascularized flaps |
| Large (>3 cm) | Regional or free flap |
Extradural defects - intact dura, no CSF leak guarantee.
Intradural defects - dural violation; guaranteed CSF leak; further classified as low-flow vs. high-flow (cistern violation).
Flap Options
Nasoseptal flap (Hadad flap) - workhorse
- Mucosa with mucoperiosteum/mucopericondrium.
- Vascular supply: posterior septal artery (branch of sphenopalatine artery).
- Indicated for medium to large anterior and middle cranial fossa defects with high CSF leak risk.
- CSF leak rate historically <5% with this flap.
- Limitation: size of flap may not cover very large anterior defects.
Posterior-pedicled inferior turbinate flap
- Used when prior septectomy or wide sphenoidectomy has compromised the posterior septal artery.
- Blood supply: inferior turbinate artery from posterior lateral nasal artery (sphenopalatine artery).
- Best for posterior defects (sellar, parasellar, mid-clival).
- Limitations: small size, short pedicle, restricted rotation angle.
Posterior-pedicled middle turbinate flap
- Supply: middle turbinate branch of posterior lateral nasal artery.
- Indicated when nasoseptal flap is unavailable; for planum sphenoidale, sellar, and fovea ethmoidalis defects.
- Advantage over inferior turbinate flap: greater length and arc of rotation.
Endoscopic-assisted pericranial flap
- Based on supraorbital and supratrochlear arteries.
- Harvested externally, tunneled endoscopically through a nasion defect.
- Used for cribriform, planar, and sellar defects.
- Large-volume vascularized coverage.
Temporoparietal fascial flap
- Laterally based, vascularized by anterior branch of the superficial temporal artery.
- Does not include temporalis muscle or deep temporal artery.
- Indicated for orbital, clival, and anterior/middle cranial fossa defects.
Acellular/cellular grafts
-
Collagen or dermal matrix (acellular); free mucosal grafts from nasal floor, middle turbinate, or septum; fat graft for dead space obliteration (harvested from abdomen).
-
Reserved for small defects only.
-
K J Lee's Essential Otolaryngology, p. 601-602
6. Special Considerations
2-surgeon, 4-handed technique - used in EEA; one surgeon manages the endoscope, the other operates bimanually. Improves technical results and hemostasis.
Intraoperative navigation - CT/MRI-guided navigation systems improve margin status in advanced anterior craniofacial malignancies (PMID: 39662109).
Orbital management:
- Orbital floor invasion alone does not mandate exenteration.
- Invasion of orbital fat or extraocular muscles is the threshold for exenteration in most centers.
- Degree of orbital involvement is a prognostic factor that also determines EEA feasibility.
Prior radiation - significantly increases wound complication risk and impairs flap healing. Vascularized reconstruction is essential in previously irradiated fields.
Patient risk factors for postoperative CSF leak: intracranial hypertension, obesity, obstructive sleep apnea.
7. Complications
Endoscopic Approach Complications
| Complication | Notes |
|---|---|
| CSF leak | Most common; risk reduced to 4-6% with vascularized reconstruction |
| Tension pneumocephalus | Less common than with open approach; presents with rapid neurologic decline, confusion, loss of consciousness |
| Vascular injury | Ranges from venous bleeding to carotid injury. Carotid injury: immediate muscle tamponade (crushed muscle from neck/thigh) + nasoseptal flap coverage + gentle packing → urgent angiography. Hemostatic agents: warm irrigation, Gelfoam with thrombin, FloSeal, cautery, aneurysm clipping |
| Cerebrovascular accident | Due to vascular injury, venous infarct from CSF pressure changes, or embolic phenomena |
| Meningitis/infectious | 2% rate; typically from postoperative crusting |
| Neurologic deficits | Transient 2.5%; permanent 1.8% |
| Anosmia | Expected with transcribriform resections |
| Orbital injury/diplopia | From medial orbital wall/periorbita dissection |
| Minor | Sinusitis, vestibular burns, synechiae |
Open/Craniofacial Approach Complications
-
Wound complications 20%
-
Systemic complications 5%
-
Orbital complications 1.5%
-
Mortality 4.7% (craniofacial resection)
-
K J Lee's Essential Otolaryngology, p. 639; Cummings Otolaryngology, p. 3366
8. Outcomes Summary
| Approach | Mortality | Morbidity | 5-yr Survival |
|---|---|---|---|
| Craniofacial resection | 4.7% | 33-36% | ~50% (all sinonasal cancers) |
| Endoscopic endonasal | 0.9% | CSF leak 4-6% | Comparable to open in selected cases |
Recent evidence (PMID: 42169562, systematic review/meta-analysis 2026) confirms favorable long-term quality-of-life outcomes after endoscopic resection. Navigation-assisted surgery improves margin status in advanced craniofacial malignancies (PMID: 39662109).
Key takeaways:
- Surgical approach selection depends on tumor location, extent, and histology - endoscopic endonasal for medially located and skull base lesions without lateral/skin/palate invasion; open/craniofacial for extensive or laterally placed disease.
- Margin-negative resection is the single most important determinant of survival.
- Multimodality therapy (surgery + IMRT ± chemotherapy) is standard for most malignant histologies.
- Vascularized skull base reconstruction (especially the nasoseptal flap) has dramatically reduced CSF leak rates.
- 2-surgeon, 4-handed endoscopic technique and intraoperative navigation are current best practices.
This is a shared conversation. Sign in to Orris to start your own chat.