The Thyroid gland surgical anatomy and applied aspect
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
I now have extensive, comprehensive content from Sabiston and Gray's Anatomy. Let me compile a complete, well-structured answer.
Thyroid Gland: Surgical Anatomy and Applied Aspects
1. Gross Anatomy
The thyroid gland is the largest endocrine organ in the body. It lies anterior to the trachea, below and lateral to the thyroid cartilage, straddling the 2nd–4th tracheal rings. It consists of:
- Two lateral lobes — covering the anterolateral surfaces of the trachea, the sides of the thyroid cartilage, and the cricoid cartilage
- Isthmus — connecting the two lobes anteriorly, lying over the 2nd–3rd tracheal rings
- Pyramidal lobe — a superior projection of the isthmus (remnant of the thyroglossal duct), present in ~50% of people; may extend as high as the hyoid bone and contains functional thyroid tissue
Capsule and fascia: The gland has a true fibrous capsule from which septa extend inward, dividing it into lobules. It is enclosed in a false capsule derived from the pretracheal (deep cervical) fascia. The space between the true and false capsules contains parathyroid glands, blood vessels, and lymphatics — a critical surgical plane.
— Gray's Anatomy for Students, p. 1156; Sabiston Textbook of Surgery, p. 1519
2. Blood Supply
Arterial Supply
| Artery | Origin | Territory |
|---|---|---|
| Superior thyroid artery | First branch of external carotid artery | Upper pole of each lobe |
| Inferior thyroid artery | Thyrocervical trunk (subclavian a.) | Lower and posterior lobe |
| Thyroid ima artery | Brachiocephalic trunk or aortic arch (10%) | Anterior surface of isthmus |
The inferior thyroid artery is the most surgically important — it supplies the parathyroid glands and crosses in close proximity to the recurrent laryngeal nerve (RLN).
Venous Drainage
Three pairs of veins drain the thyroid:
- Superior thyroid vein → internal jugular vein
- Middle thyroid vein → internal jugular vein (no corresponding artery; identified and ligated early in thyroidectomy)
- Inferior thyroid veins (often a plexus) → right and left brachiocephalic veins
Lymphatic Drainage
Drains to paratracheal (level VI) nodes and deep cervical nodes inferior to the omohyoid along the internal jugular vein. This pathway is the primary route of spread for thyroid cancers, making central compartment dissection (level VI) important for well-differentiated carcinoma.
— Gray's Anatomy for Students, p. 1159
3. Recurrent Laryngeal Nerve (RLN)
The RLN is the single most important structure in thyroid surgery.
Course:
- Right RLN: loops around the right subclavian artery, then ascends obliquely in the neck — more lateral and oblique, entering the tracheo-esophageal groove higher up
- Left RLN: loops around the arch of the aorta, then ascends in the tracheo-esophageal groove — more vertical and medial
Both nerves pass deep to the posteromedial surface of the lateral thyroid lobe, near the ligament of Berry, to enter the larynx deep to the inferior constrictor of the pharynx at the cricothyroid joint.
Relationship to the inferior thyroid artery: The RLN may pass anterior to, posterior to, or between the branches of the inferior thyroid artery. This relationship is variable and the nerve must be individually identified before ligation of the artery.
Non-recurrent laryngeal nerve (NRLN): Occurs in ~1% on the right (associated with an aberrant right subclavian artery — arteria lusoria), virtually never on the left unless there is a right-sided aortic arch. The NRLN passes directly from the vagus to the larynx horizontally at the level of the cricothyroid membrane — easily mistaken for a vessel and injured if not anticipated.
Function: Motor to all intrinsic laryngeal muscles (except cricothyroid). Injury causes:
- Unilateral RLN injury → hoarseness, weak voice (ipsilateral cord palsy)
- Bilateral RLN injury → stridor, respiratory distress, may require tracheostomy
— Gray's Anatomy for Students, p. 1159; Sabiston Textbook of Surgery, p. 1519
4. Superior Laryngeal Nerve (SLN)
Often overlooked but equally important:
- External branch of SLN (ESLN): motor to the cricothyroid muscle (the "tensor" of the vocal cord, responsible for high-pitched voice). It descends along the inferior constrictor, closely associated with the superior thyroid artery near the upper pole.
- Internal branch of SLN: sensory to the supraglottis and laryngeal mucosa
Surgical relevance: During superior pole dissection, the ESLN may be injured if the superior thyroid artery is ligated in bulk rather than close to the thyroid capsule. Injury causes subtle dysphonia — loss of high-pitched phonation — particularly significant for singers and professional voice users.
The Cernea classification describes variants of ESLN proximity to the superior thyroid vessels:
- Type 1: crosses superior thyroid vessels >1 cm above the upper pole (safe zone)
- Type 2a: crosses < 1 cm above upper pole (risk)
- Type 2b: crosses at or below the upper pole (highest risk)
5. Parathyroid Glands
Four parathyroid glands (occasionally 3–6) lie on the posterior surface of the thyroid lobes, between the true and false capsules.
| Gland | Embryological origin | Position |
|---|---|---|
| Superior (PT IV) | 4th pharyngeal pouch | Posterior, at middle 1/3 of thyroid, near cricothyroid junction (~1 cm above RLN crossing ITA) |
| Inferior (PT III) | 3rd pharyngeal pouch | More variable; may be in tracheo-esophageal groove, thyrothymic ligament, or anterior mediastinum |
Blood supply: Almost exclusively from the inferior thyroid artery — hence the importance of ligating this artery distally (at the thyroid capsule) rather than proximally (which would devascularize the parathyroids).
Surgical rule: If a parathyroid gland is inadvertently devascularized, it should be autotransplanted (minced into 1 mm³ fragments and implanted into a sternocleidomastoid muscle pocket, or the non-dominant forearm in MEN2A).
6. Ligament of Berry (Posterior Suspensory Ligament)
A dense, fibrous condensation attaching the posteromedial thyroid capsule to the cricoid cartilage and upper tracheal rings. It:
- Fixes the thyroid to the trachea — explaining why the thyroid rises on swallowing (key clinical test)
- Contains the terminal branches of the RLN as it enters the larynx — the nerve may be embedded within or just medial to this ligament
- The RLN is at highest risk at the point of division of this ligament during thyroidectomy
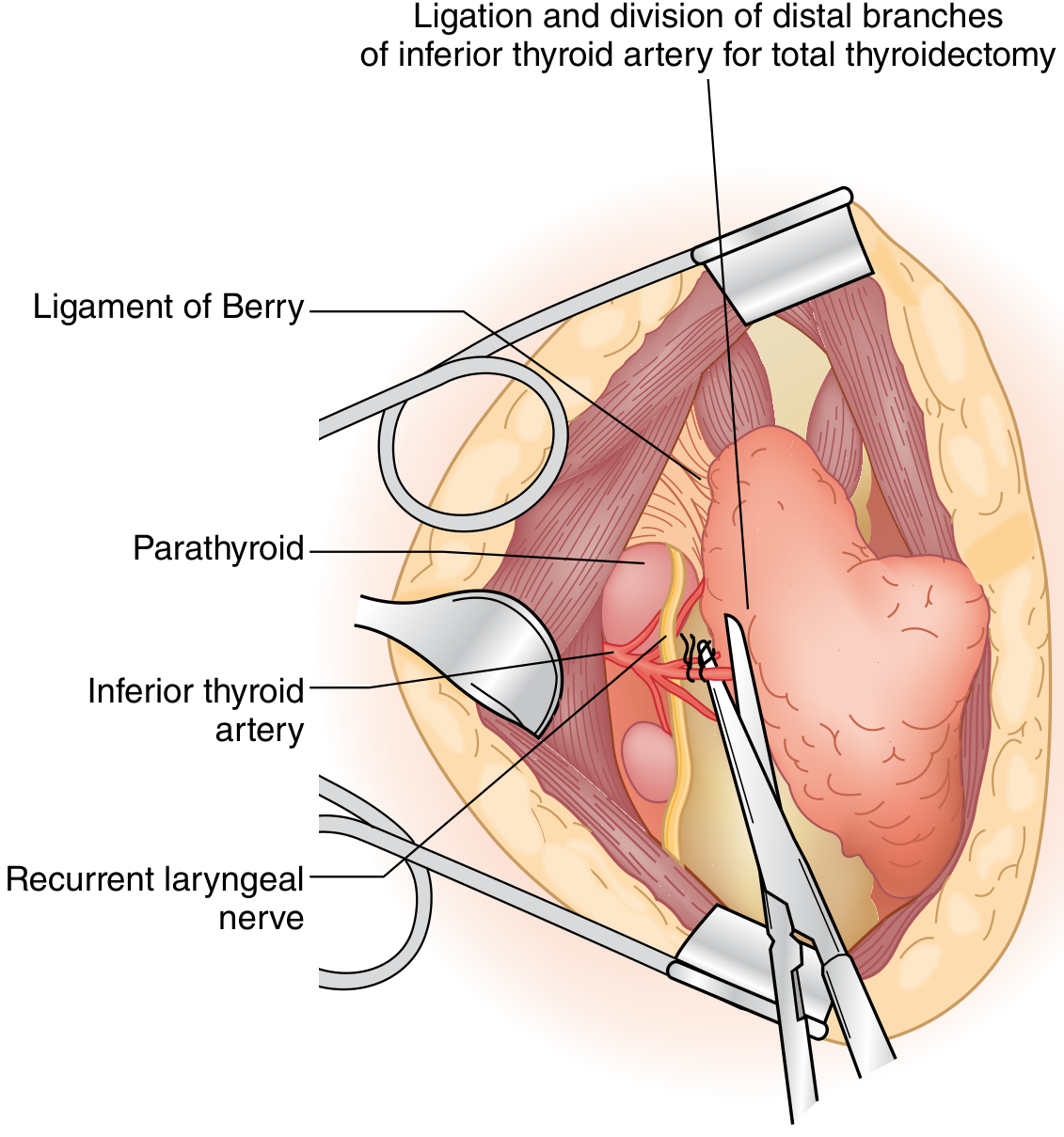
Surgical view: Ligament of Berry, parathyroid gland, inferior thyroid artery (ligated distally), and recurrent laryngeal nerve — Sabiston Textbook of Surgery
7. Key Surgical Relations
| Structure | Relevance |
|---|---|
| Trachea | Medial — may be compressed/deviated by large goiters |
| Esophagus | Posteromedial to left lobe — at risk in re-operative surgery |
| Common carotid arteries | Lateral — enclosed in carotid sheath |
| Internal jugular vein | Lateral in carotid sheath |
| Sternothyroid & sternohyoid muscles | Anterior — divided in midline or retracted during thyroidectomy |
| Cricothyroid muscle | Superior — innervated by ESLN |
8. Thyroglossal Duct and Developmental Considerations
The thyroid gland develops from the foramen cecum of the tongue and descends along the thyroglossal duct (in front of the hyoid bone) to its final pretracheal position. Remnants of this duct can form:
- Thyroglossal duct cysts — midline neck cysts, move with swallowing AND protrusion of the tongue
- Ectopic thyroid — may occur anywhere along the descent path; lingual thyroid is the most common ectopic site and may be the only thyroid tissue in some patients
Sistrunk operation: Surgical excision of a thyroglossal duct cyst requires removal of the central portion of the hyoid bone to prevent recurrence (because the duct passes through or near the hyoid).
9. Applied/Clinical Points
Complications of Thyroid Surgery
| Complication | Cause | Consequence |
|---|---|---|
| Hoarseness | RLN injury | Unilateral cord palsy |
| Stridor/respiratory distress | Bilateral RLN injury | Emergency; may need tracheostomy |
| Hypocalcemia (tetany) | Hypoparathyroidism — devascularization or inadvertent removal of parathyroids | Tingling perioral, Chvostek's sign, Trousseau's sign, seizures |
| Hypothyroidism | Insufficient thyroid remnant | Lifelong replacement therapy needed |
| Thyroid storm | Inadequate preoperative preparation in hyperthyroid patients | Life-threatening; tachycardia, hyperthermia, agitation |
| Haematoma | Vessel injury (superior thyroid or middle thyroid vein) | Can cause airway compression — emergency reopening of wound at bedside |
| Wound infection / scar | Incision complications | — |
"Safe" Surgical Principles
- Identify the RLN visually before any ligation — do not assume the nerve's position based on expected anatomy
- Ligate the inferior thyroid artery distally (close to thyroid capsule) to preserve parathyroid blood supply
- Dissect the superior pole vessels individually close to the capsule to protect the ESLN
- Divide the ligament of Berry with caution — the RLN is at its closest here
- Use intraoperative neuromonitoring (IONM) — stimulate the vagus/RLN before and after resection to confirm integrity; recommended when ≥26 cases/year threshold is exceeded
Goiter and the Airway
A large retrosternal goiter can cause tracheal compression, deviation, or the tracheomalacia sign (softening of tracheal rings). Pemberton's sign (facial plethora, venous engorgement when arms are raised) indicates superior thoracic inlet obstruction.
Thyroid Cancer Surgery
- Total thyroidectomy is standard for papillary/follicular cancers >1 cm
- Central compartment dissection (level VI) for central nodal metastases
- Medullary thyroid cancer (MTC): total thyroidectomy + bilateral central neck dissection; prophylactic thyroidectomy in hereditary MTC (RET mutation carriers) based on timing determined by mutation risk category
- Berry-picking of central nodes is insufficient — formal level VI clearance reduces recurrence risk
Substernal/Retrosternal Goiter
50% of thyroid volume extends below the thoracic inlet. Most (>95%) can be removed through a cervical incision by careful superior pedicle ligation and gentle downward traction. Sternotomy is rarely required unless there is a separate intrathoracic blood supply from mediastinal vessels.
10. Surgical Anatomy Summary Diagram
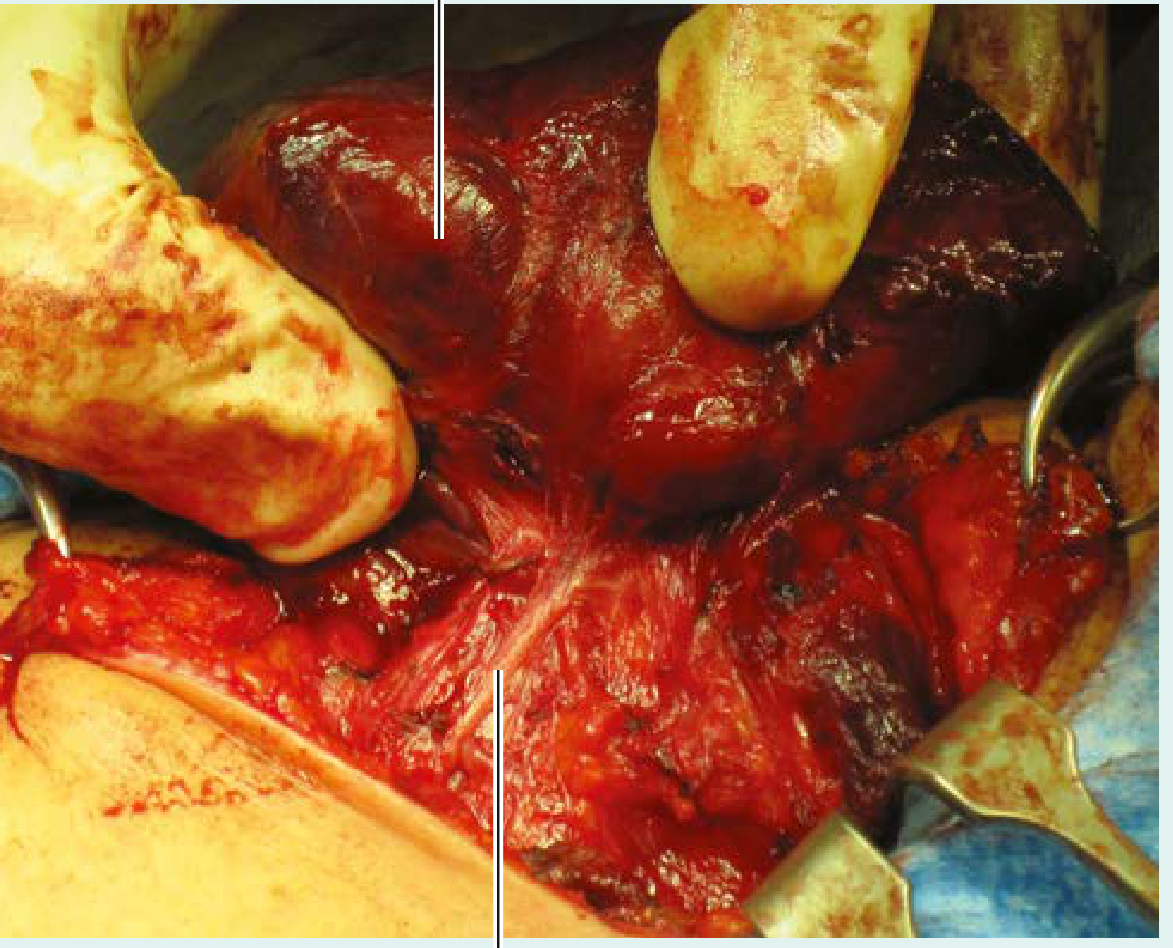
Intraoperative identification of the left recurrent laryngeal nerve — Gray's Anatomy for Students
Sources:
- Gray's Anatomy for Students, pp. 1156–1165 (Thyroid & Parathyroid Glands, Recurrent Laryngeal Nerves, Thyroidectomy)
- Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice, pp. 1519–1627 (Thyroidectomy — Surgical Technique, Complications, Applied Anatomy)
This is a shared conversation. Sign in to Orris to start your own chat.