Define NSAIDs drugs classfication uses side effects Mechamism of actions
Reading File
Finding Sources
Finding Sources
Searching PubMed
NSAIDs mechanism classification adverse effects
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have rich, comprehensive information from multiple authoritative sources. Let me compile the full answer.
NSAIDs: Complete Reference
Definition
Nonsteroidal anti-inflammatory drugs (NSAIDs) are a pharmacologically diverse group of agents that share three core pharmacological actions: anti-inflammatory, analgesic (pain-relieving), and antipyretic (fever-reducing). They are non-steroidal (structurally unrelated to corticosteroids) and work primarily by inhibiting the cyclooxygenase (COX) enzyme system.
Mechanism of Action
The Arachidonic Acid Cascade
When cells are injured, membrane phospholipids are cleaved by phospholipase A2, releasing arachidonic acid. This free arachidonic acid is then converted by cyclooxygenase (COX) enzymes into prostaglandins, prostacyclin, and thromboxane A2 - the key mediators of pain, fever, and inflammation.
NSAIDs act by blocking COX enzymes, thereby reducing the synthesis of these prostaglandin mediators.
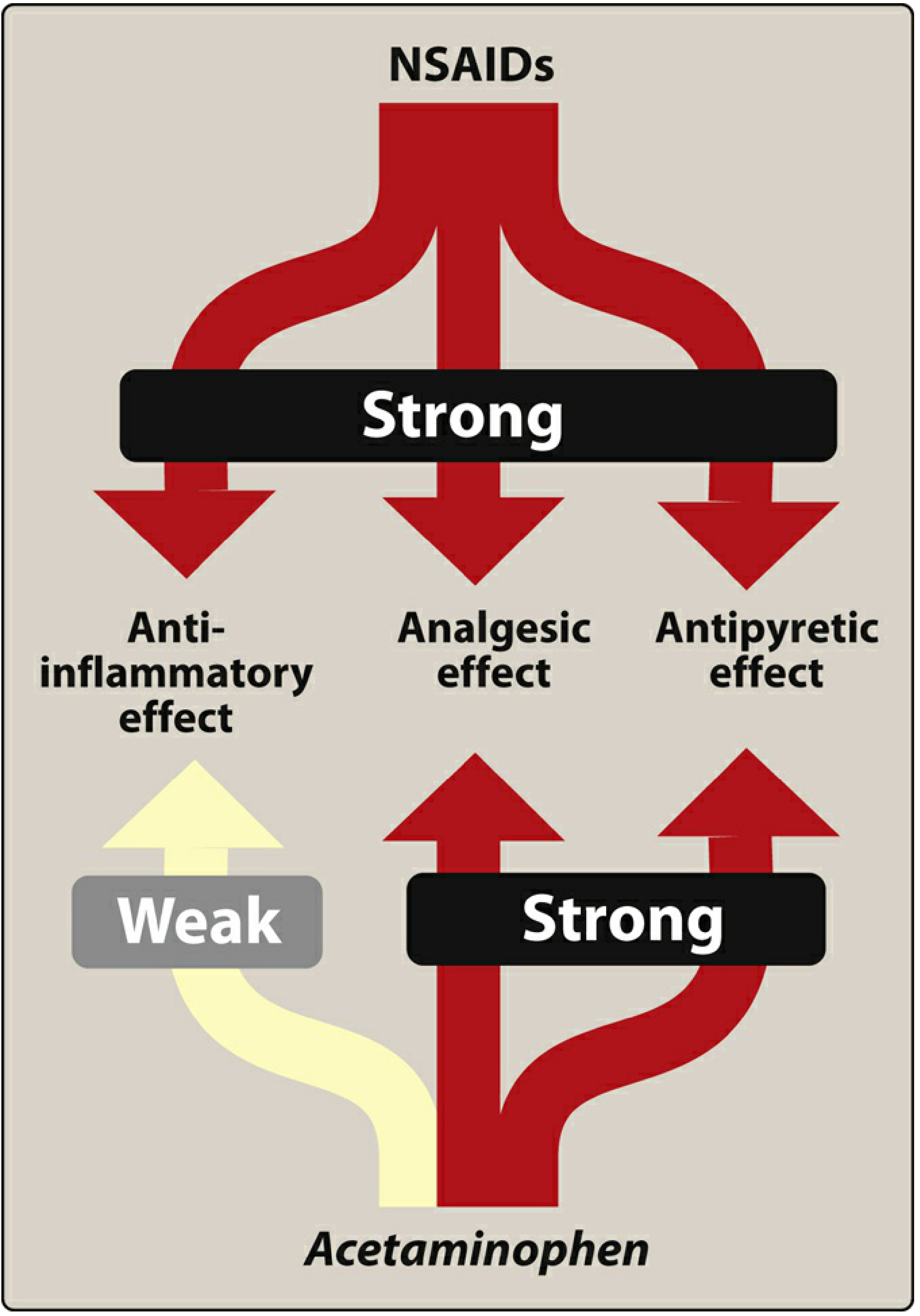
Figure: Actions of nonsteroidal anti-inflammatory drugs (NSAIDs) and acetaminophen - Lippincott Illustrated Reviews: Pharmacology
The Two COX Isoenzymes
| Isoenzyme | Distribution | Key Functions |
|---|---|---|
| COX-1 | Constitutively expressed in virtually all cells | Gastric mucosal protection (mucus + bicarbonate production), platelet thromboxane A2 synthesis, renal blood flow maintenance, homeostatic functions |
| COX-2 | Induced by inflammation, injury, cytokines | Prostaglandin synthesis during inflammation; also constitutively expressed in the kidney and brain |
As stated in Rosen's Emergency Medicine:
"COX-1 is present in all cells and plays an important role in homeostatic functions. COX-2 is induced by injury or inflammation and generates prostaglandins as part of the inflammatory process. Nonselective NSAIDs inhibit both COX-1 and COX-2, resulting in multiple beneficial effects (reduction of inflammation, pain, fever) and some important undesirable effects."
How NSAIDs Block COX
- Aspirin - Transfers an acetyl group irreversibly to a serine residue (Ser530) in the COX active site, permanently inactivating both COX-1 and COX-2. Because platelets cannot synthesize new protein, this antiplatelet effect lasts for the entire platelet lifespan (~10 days).
- Traditional (nonselective) NSAIDs (ibuprofen, naproxen, etc.) - Compete reversibly with arachidonate for the COX active site. Ibuprofen is a rapid, reversible, time-independent inhibitor; indomethacin and diclofenac are time-dependent allosteric inhibitors that bind more slowly but exit the active site only after hours.
- Selective COX-2 inhibitors (coxibs) - Exploit a unique valine substitution at position 523 in COX-2 (vs. isoleucine in COX-1), which opens a hydrophobic side pocket accessible only to bulkier coxib molecules. Celecoxib and etoricoxib occupy this pocket with their sulfur-containing phenyl ring, achieving selective COX-2 inhibition without blocking COX-1.
Three Pharmacological Effects Explained
-
Anti-inflammatory: Reducing prostaglandin synthesis blunts vasodilation, vascular permeability, and sensitization of immune cells at inflammatory sites. NSAIDs suppress inflammation in arthritis but do not arrest disease progression.
-
Analgesic: PGE2 sensitizes peripheral nociceptors to bradykinin and histamine. By decreasing PGE2, NSAIDs raise the pain threshold. This effect is primarily mediated via COX-2 inhibition. All NSAIDs have roughly equivalent analgesic efficacy; ketorolac is an exception as it can address more severe pain (short-term only).
-
Antipyretic: Pyrogens (cytokines from activated WBCs) stimulate PGE2 synthesis in the anterior hypothalamus, raising the thermostat set-point. NSAIDs block this PGE2 synthesis, resetting the thermostat toward normal, increasing peripheral vasodilation and sweating. NSAIDs have no effect on normal body temperature.
(Lippincott Illustrated Reviews: Pharmacology; Fischer's Mastery of Surgery, 8e)

Classification
NSAIDs are classified in two main ways: by chemical structure and by COX selectivity.
By COX Selectivity (Most Clinically Useful)
1. Nonselective COX-1 and COX-2 Inhibitors (traditional NSAIDs - tNSAIDs)
These inhibit both isoforms and constitute the majority of available NSAIDs:
| Drug Class | Examples |
|---|---|
| Salicylates | Aspirin (acetylsalicylic acid), diflunisal, salsalate |
| Propionic acids | Ibuprofen, naproxen, ketoprofen, flurbiprofen, oxaprozin |
| Acetic acids | Indomethacin, diclofenac, etodolac, ketorolac, sulindac, tolmetin |
| Fenamic acids | Mefenamic acid, meclofenamate |
| Oxicams | Piroxicam, meloxicam* |
| Pyrazolidines | Phenylbutazone |
| Naphthylalanine | Nabumetone |
*Meloxicam shows preferential (not absolute) COX-2 selectivity.
2. Preferentially COX-2 Selective
- Meloxicam, nimesulide, etodolac, nabumetone
3. Highly Selective COX-2 Inhibitors (Coxibs)
| Drug | Notes |
|---|---|
| Celecoxib | Currently available; sulfonamide group; lower GI toxicity |
| Rofecoxib | Withdrawn from market (2004) - cardiovascular risk |
| Valdecoxib | Withdrawn - cardiovascular + skin reactions |
| Etoricoxib | Available in many countries; not FDA-approved in USA |
| Lumiracoxib | Withdrawn - hepatotoxicity |
As noted in Firestein & Kelley's Textbook of Rheumatology:
"The prototypical COX-2-selective NSAIDs, celecoxib and rofecoxib, are diaryl compounds containing a sulfonamide (celecoxib) and methylsulfone (rofecoxib). The sulfur-containing phenyl ring of COX-2-selective NSAIDs plays a pivotal role in binding stability by occupying the hydrophobic side pocket characteristic of the COX-2 catalytic site."
Aspirin: A Special Case
Aspirin is unique - it irreversibly inhibits both COX-1 and COX-2, unlike all other NSAIDs which bind reversibly. This makes its antiplatelet effect permanent for each individual platelet, explaining its unique role in cardiovascular prophylaxis.
Therapeutic Uses
1. Musculoskeletal and Inflammatory Conditions
- Osteoarthritis - first-line for symptomatic pain relief
- Rheumatoid arthritis - symptom relief only (do not modify disease; must be combined with DMARDs)
- Ankylosing spondylitis
- Gout (acute attacks) - indomethacin classically used
- Psoriatic arthritis
2. Pain Management
- Mild-to-moderate pain: headache, myalgia, arthralgia, dental pain
- Dysmenorrhea (menstrual cramps) - very effective
- Postoperative pain - part of multimodal analgesia; opioid-sparing effect
- Ketorolac - parenteral NSAID for moderate-to-severe pain (short-term only, max 5 days)
- Cancer pain - useful combined with opioids for opioid-sparing effect
3. Fever
- Aspirin, ibuprofen, naproxen (avoid aspirin in children under 19 with viral infections - Reye syndrome risk)
4. Cardiovascular
- Low-dose aspirin (75-162 mg/day, typically 81 mg): secondary prevention of MI, TIA, stroke; acute MI management
- Irreversible COX-1 blockade reduces thromboxane A2-mediated platelet aggregation
5. Other Uses
- Tocolysis (preterm labor) - indomethacin (COX inhibitor reduces prostaglandin-driven uterine contractions)
- Ductus arteriosus closure in neonates - indomethacin or ibuprofen IV
- Topical applications: Diclofenac gel (osteoarthritis of knee/hands); ketorolac eye drops (allergic conjunctivitis, post-op ocular inflammation); salicylic acid (acne, warts, corns)
- Colorectal cancer chemoprevention (ongoing research)
(Lippincott Illustrated Reviews: Pharmacology; Goldman-Cecil Medicine; Creasy & Resnik's Maternal-Fetal Medicine)
Adverse Effects (Side Effects)
As stated in Rosen's Emergency Medicine: "As a group, and because of their common use, NSAIDs are responsible for more serious drug-related side effects than any other analgesic drug class."
1. Gastrointestinal (Most Common)
Mechanism: COX-1 inhibition reduces gastric mucosal prostaglandins that normally stimulate mucus and bicarbonate production and maintain mucosal blood flow. NSAIDs also have a direct topical toxic effect on the mucosa.
- 10-60% of chronic users develop GI complaints (dyspepsia, nausea, abdominal pain)
- Peptic ulcer disease, gastric/duodenal erosions, bleeding, perforation - more than 100,000 hospitalizations and ~16,500 deaths/year in the USA
- NSAID enteropathy - small bowel mucosal injury (increased permeability, chronic blood loss, ulceration, diaphragm-like strictures) seen in up to 70% of NSAID users on capsule endoscopy
- Risk reduced (but not eliminated) with selective COX-2 inhibitors (coxibs)
- Prevention: proton pump inhibitors (PPIs) co-prescribed; misoprostol (a prostaglandin analog)
2. Cardiovascular
Mechanism: COX-2 generates endothelial prostacyclin (PGI2), a vasodilator that opposes platelet aggregation. Selective COX-2 inhibition reduces PGI2 without reducing platelet thromboxane A2 (which requires COX-1), tipping the balance toward thrombosis and vasoconstriction.
- Selective COX-2 inhibitors (coxibs) - increased risk of MI, stroke, and thrombotic events
- Nonselective NSAIDs - generally balance out cardiovascular effects (reduced TXA2 and reduced PGI2)
- However, all NSAIDs (except aspirin) may increase cardiovascular risk at higher doses or with prolonged use
- Celecoxib contraindicated perioperatively in CABG patients
- Can increase blood pressure (sodium and water retention)
- Can worsen congestive heart failure
3. Renal
Mechanism: Prostaglandins (via COX-1) maintain renal afferent arteriolar vasodilation and GFR, especially in states of reduced perfusion pressure. NSAID-induced prostaglandin loss leads to unopposed vasoconstriction.
- Acute kidney injury (AKI) - especially in volume-depleted patients, those with heart failure, CKD, or elderly
- Sodium and water retention - edema, hypertension
- Hyperkalemia
- Chronic renal failure with prolonged use
- Analgesic nephropathy with long-term phenacetin combination products
4. Hematological
- Platelet dysfunction / prolonged bleeding time - COX-1 inhibition reduces TXA2-mediated platelet aggregation (especially problematic with aspirin, which is irreversible)
- Thrombocytopenia (less common)
- Increased risk of bleeding, particularly with anticoagulants
5. Respiratory
- Aspirin-exacerbated respiratory disease (AERD) / Samter's Triad: aspirin sensitivity in patients with asthma + nasal polyps. Caused by shunting of arachidonic acid toward leukotrienes (via 5-lipoxygenase) when COX is blocked - leukotrienes are potent bronchoconstrictors
- Can precipitate acute bronchospasm in susceptible asthmatic patients
6. Hepatic
- Elevated liver enzymes (transaminases) - usually dose-dependent and reversible
- Rare: serious hepatotoxicity (more associated with specific agents; lumiracoxib withdrawn for this reason)
7. CNS
- Headache, dizziness, tinnitus (especially salicylate toxicity)
- Salicylate toxicity / salicylism (high-dose aspirin): tinnitus, vertigo, hearing loss, hyperventilation, metabolic acidosis
8. Hypersensitivity
- Urticaria, angioedema, anaphylaxis
- Cross-reactivity among NSAIDs common
9. Fetal/Neonatal (Specific to Pregnancy)
- Premature closure of the ductus arteriosus (prostaglandins E2 and prostacyclin normally maintain ductal patency)
- Oligohydramnios (reduced fetal urine output)
- Neonatal pulmonary hypertension
- Risk is greatest after 30-32 weeks gestation - indomethacin use requires fetal Doppler monitoring
10. Reye Syndrome
- Aspirin in children <19 years old with viral illness (influenza, varicella) - risk of fulminating hepatitis with cerebral edema. Aspirin is therefore contraindicated in children for viral fever.
Key Contraindications Summary
| Condition | Reason |
|---|---|
| Active peptic ulcer disease | GI bleeding risk |
| Severe renal or hepatic failure | Nephrotoxicity, impaired metabolism |
| Perioperative CABG | COX-2 inhibitors increase thrombotic risk |
| Aspirin-sensitive asthma | Bronchospasm via leukotriene shunting |
| Third trimester pregnancy | Ductal constriction, oligohydramnios |
| Children with viral illness (aspirin) | Reye syndrome |
| Severe heart failure | Sodium retention, worsening hemodynamics |
Summary Table
| Feature | Nonselective NSAIDs | COX-2 Selective (Coxibs) | Aspirin |
|---|---|---|---|
| COX-1 inhibition | Yes | Minimal | Irreversible |
| COX-2 inhibition | Yes | Yes (selective) | Irreversible |
| GI toxicity | High | Lower | High |
| Cardiovascular risk | Moderate | Higher (TXA2/PGI2 imbalance) | Reduced (antiplatelet) |
| Antiplatelet effect | Reversible | No significant effect | Permanent (life of platelet) |
| Examples | Ibuprofen, naproxen, diclofenac, indomethacin | Celecoxib, etoricoxib | Aspirin |
Sources:
- Lippincott Illustrated Reviews: Pharmacology
- Fischer's Mastery of Surgery, 8e
- Rosen's Emergency Medicine: Concepts and Clinical Practice
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set
- Goldman-Cecil Medicine, International Edition
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
- Harper's Illustrated Biochemistry, 32nd Ed.
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice
This is a shared conversation. Sign in to Orris to start your own chat.