Mandibular first premolar summary
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
The library doesn't have a dedicated dental anatomy textbook, so no results were found for premolar content. I'll provide a comprehensive summary from established dental anatomy knowledge.
Mandibular First Premolar — Summary
Overview
The mandibular first premolar is the 4th tooth from the midline in the mandibular arch (Universal #21 right, #28 left; FDI: 44 right, 34 left). It erupts around 10–12 years of age and is the most anatomically complex of all premolars, often considered a transitional tooth between the canine and the posterior teeth.
Chronology
| Event | Timing |
|---|---|
| Initiation of calcification | 1.5–2.5 years |
| Crown completion | 5–6 years |
| Eruption | 10–12 years |
| Root completion | 12–13 years |
Crown Morphology
Buccal View
- Resembles a mandibular canine from the buccal aspect
- Long, well-developed buccal cusp — sharp, with mesial and distal cusp ridges
- The buccal cusp tip is centered or slightly mesial
- Mesial slope is shorter than the distal slope (unlike the canine, whose mesial slope is longer)
- Mesiobuccal line angle is more prominent than the distobuccal
Lingual View
- The lingual cusp is markedly smaller than the buccal cusp (~⅔ the height), making this tooth appear almost unicuspid
- Lingual cusp is often non-functional (does not occlude with the opposing arch)
- The lingual surface tilts sharply lingually from the occlusal
- A mesiolingual groove (also called the mesial developmental groove) crosses the mesial marginal ridge — this is a key distinguishing feature
Occlusal View
- Outline is roughly pentagonal or "diamond-shaped"
- Buccal cusp dominates the occlusal table; lingual cusp is much smaller and more posteriorly positioned
- A transverse ridge connects the buccal cusp ridge to the lingual cusp ridge, dividing the occlusal surface into mesial and distal fossae
- Mesial fossa is smaller and shallower; distal fossa is larger and deeper
- A mesiolingual developmental groove crosses the mesial marginal ridge — clinically significant (prone to caries, and a distinguishing feature from the second premolar)
Proximal View
- The crown tilts lingually relative to the root axis
- Buccal cusp is large and prominent; lingual cusp barely visible over the cervical line
- The mesial surface shows a distinct mesial developmental depression (concavity), important in periodontal disease and scaling
Root Morphology
- Usually a single root, ovoid/compressed buccolingually
- Root trunk is broad buccolingually, narrow mesiodistally
- Mesial surface often has a distinct longitudinal developmental groove (root concavity), increasing the risk of periodontal pocketing
- Root length averages ~14 mm
- Root may occasionally bifurcate (most commonly in the apical third) — ~25% of cases have two root canals
Pulp Anatomy
- Pulp chamber is wide buccolingually, narrow mesiodistally
- Two pulp horns: buccal horn is prominent; lingual horn is small or absent
- Canal configuration:
- Type I (1-1): Single canal — most common (~75%)
- Type II (2-1): Two canals joining into one
- Type III (1-2-1): Canal splits then rejoins
- Type IV (2-2): Two separate canals — seen in ~25%
- Average root canal working length: ~21 mm
Distinguishing Features (vs. Mandibular Second Premolar)
| Feature | Mandibular 1st Premolar | Mandibular 2nd Premolar |
|---|---|---|
| Lingual cusp(s) | One, much smaller | One or two, nearly equal to buccal |
| Mesiolingual groove | Present (crosses mesial marginal ridge) | Absent |
| Occlusal outline | Asymmetric, lingual cusp offset | More symmetric, square or round |
| Transverse ridge | Prominent | Less distinct |
| Functional cusps | Buccal cusp only | Buccal + lingual |
| Root canals | 1–2 canals, ~25% have 2 | Usually 1 canal |
Clinical Significance
- Most difficult premolar to extract due to root curvature (distal or buccal) and proximity to the mental foramen
- Mental foramen is located near the apex of this tooth — inferior alveolar nerve block anesthesia and local infiltration must account for this proximity
- The mesiolingual groove crossing the marginal ridge is a plaque trap and caries-prone site
- Mesial root concavity increases susceptibility to periodontal attachment loss and complicates root planing
- The crown's lingual tilt affects occlusal adjustment and restoration design — restorations must account for the non-functional lingual cusp
- When used as an orthodontic extraction tooth, loss alters the buccal corridor and arch form significantly
Occlusion
- Buccal cusp is the functional cusp — it occludes in the central fossa of the maxillary first premolar and the distal fossa of the maxillary canine
- The lingual cusp does not have a consistent occlusal contact in most individuals
This tooth's combination of canine-like buccal profile, vestigial lingual cusp, mesiolingual developmental groove, and variable root canal anatomy makes it one of the most clinically challenging and anatomically distinctive teeth in the dentition.
The Thyroid gland surgical antonyms and applied aspects
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Gray's Anatomy for Students and Schwartz's Principles of Surgery. Let me compile the full response.
Thyroid Gland — Surgical Anatomy & Applied Aspects
1. Position & Relations
The thyroid gland lies in the visceral compartment of the neck, enclosed within the pretracheal (visceral) fascia. It sits anterior to the trachea below the cricoid cartilage and is covered by the strap muscles (sternohyoid, sternothyroid, omohyoid).
Components:
- Two lateral lobes covering the anterolateral trachea, cricoid cartilage, and lower thyroid cartilage
- An isthmus crossing the 2nd and 3rd tracheal cartilages anteriorly
- A pyramidal lobe extending superiorly (remnant of the thyroglossal duct) — present in ~50% of individuals
📌 Surgical note: The pretracheal fascia forms a false capsule around the gland; the true capsule is adherent to the gland and sends septa inward. Surgical dissection proceeds between these two layers.
2. Embryology & Developmental Anomalies
- The thyroid arises as a median outgrowth from the floor of the pharynx near the base of the tongue (3rd week of gestation)
- Descends via the thyroglossal duct, passing anterior to the hyoid bone, to its final position
- The foramen cecum on the posterior tongue marks the origin
- The thyroglossal duct normally obliterates by the 8th week of gestation
Developmental Anomalies
| Anomaly | Description | Clinical significance |
|---|---|---|
| Thyroglossal duct cyst | Cyst anywhere along migratory path; 80% near hyoid bone | Midline neck mass that moves upward on tongue protrusion |
| Thyroglossal sinus/fistula | Persists after cyst infection/drainage | Recurrent discharge |
| Lingual thyroid | Failure of descent; gland stays at tongue base | May be only functioning thyroid — must confirm before excision |
| Ectopic thyroid | Along the migratory path | Potential only thyroid tissue |
| Pyramidal lobe | Upward extension of isthmus along thyroglossal duct path | Must be included in total thyroidectomy; missed → recurrence |
📌 Sistrunk operation: For thyroglossal duct cyst, the entire duct + a core of the hyoid bone body must be excised to prevent recurrence (the duct is intimately related to the bone).
3. Arterial Supply
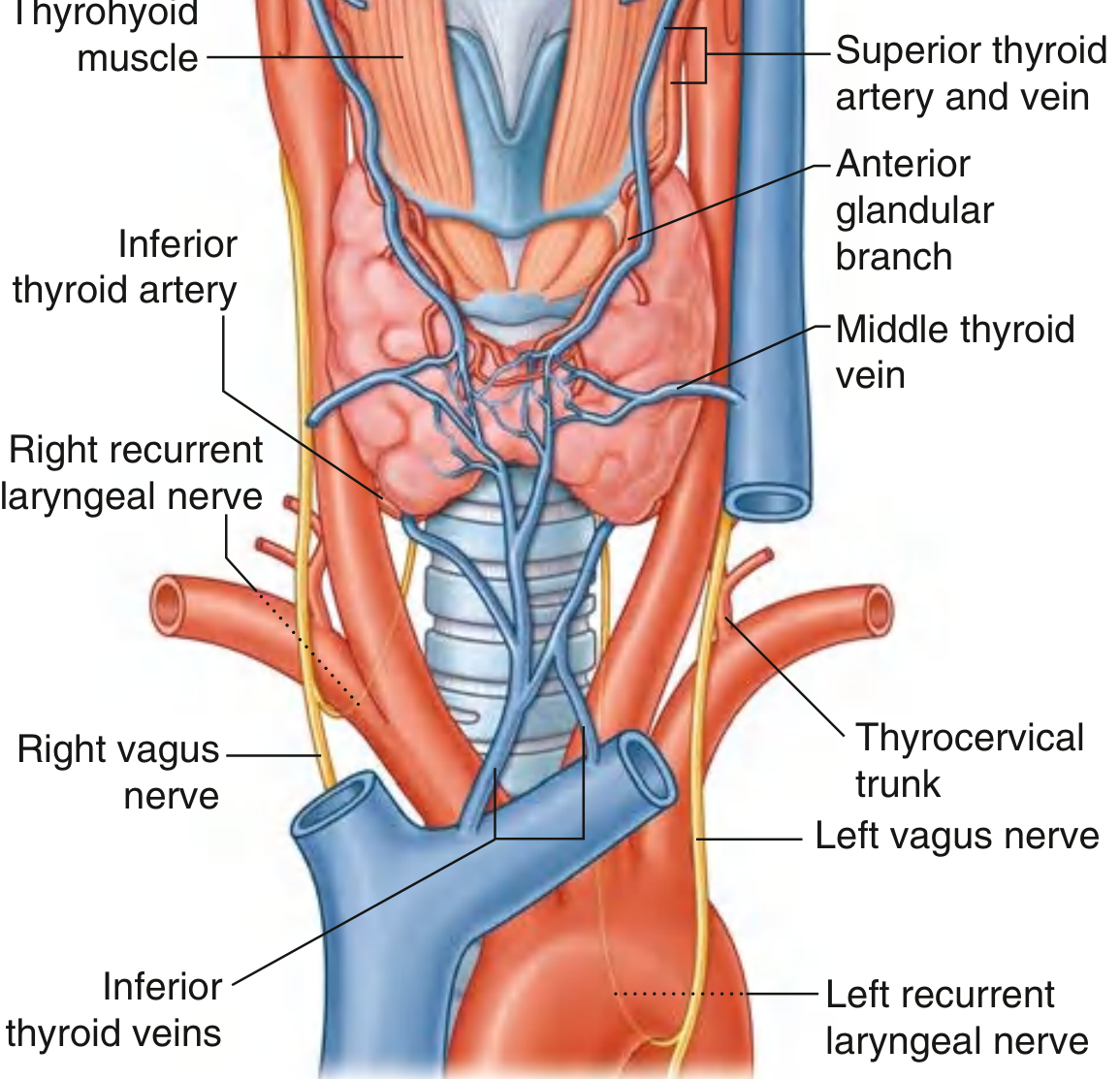
Superior Thyroid Artery
- First branch of the external carotid artery
- Descends along the lateral margin of the thyrohyoid muscle
- Enters the superior pole of the lateral lobe
- Divides into:
- Anterior glandular branch — anastomoses with the opposite side across the isthmus
- Posterior glandular branch — may anastomose with the inferior thyroid artery
📌 Surgical danger: The external branch of the superior laryngeal nerve (EBSLN) runs close to the superior thyroid artery. It must be identified before ligating the superior thyroid artery; injury causes loss of the high-pitched voice (cricothyroid muscle paralysis). The artery must be ligated close to the gland (not en masse) to protect this nerve.
Inferior Thyroid Artery
- Branch of the thyrocervical trunk (from the 1st part of the subclavian artery)
- Ascends along the medial border of the anterior scalene, passes posterior to the carotid sheath
- Reaches the inferior pole and divides into:
- Inferior branch — supplies the lower lobe; anastomoses with the posterior branch of the superior thyroid artery
- Ascending branch — supplies the parathyroid glands (critical!)
📌 Surgical danger: The recurrent laryngeal nerve (RLN) crosses the inferior thyroid artery in a variable relationship — it may pass anterior, posterior, or between branches of the artery. This crossover point is the most dangerous zone in thyroid surgery.
Thyroid Ima Artery
- Occasionally arises from the brachiocephalic trunk or the arch of the aorta
- Ascends on the anterior surface of the trachea to supply the isthmus
- Clinically important during tracheostomy — unrecognized injury causes significant bleeding
4. Venous Drainage
Three veins drain each lobe:
| Vein | Drains into |
|---|---|
| Superior thyroid vein | Internal jugular vein |
| Middle thyroid vein | Internal jugular vein |
| Inferior thyroid veins | Right and left brachiocephalic veins respectively |
📌 Surgical note: The middle thyroid vein has no arterial counterpart and is divided early in mobilization of the lobe. The inferior thyroid veins form a plexus in front of the trachea — danger during low thyroid or tracheostomy access.
5. Lymphatic Drainage
- Primary drainage to paratracheal (level VI) nodes alongside the trachea
- Secondary to deep cervical (level III/IV) nodes along the internal jugular vein, inferior to the omohyoid
📌 Surgical note: The central compartment (level VI) is the first echelon of lymph node spread in thyroid cancer — routine prophylactic central neck dissection is debated, particularly in papillary thyroid cancer.
6. Nerve Relations — The Most Critical Surgical Anatomy
Recurrent Laryngeal Nerve (RLN)
- Branch of the vagus nerve [CN X]
- Right RLN: loops around the right subclavian artery, ascends in the tracheoesophageal groove
- Left RLN: loops around the arch of the aorta (longer course), ascends in the tracheoesophageal groove
- Passes deep to the posteromedial surface of the thyroid lobe
- Enters the larynx deep to the lower margin of the inferior pharyngeal constrictor
- Related to the ligament of Berry (suspensory ligament binding thyroid to trachea and cricoid) — the RLN may pass through or just medial to it
⚠️ Surgical complication: Injury to the RLN causes hoarseness (unilateral) or respiratory distress and stridor (bilateral). The RLN must be visually identified and traced throughout thyroid surgery. Intraoperative neuromonitoring (IONM) is increasingly used.
External Branch of the Superior Laryngeal Nerve (EBSLN)
- Runs with the superior thyroid artery to supply the cricothyroid muscle
- Injury → loss of voice tension/pitch modulation (a devastating injury for singers)
- Must be dissected away before superior pole ligation
Non-Recurrent Laryngeal Nerve (NRLN)
- Rare variant (~0.5–1%) occurring on the right side only, associated with an aberrant right subclavian artery (arteria lusoria)
- The nerve enters the larynx directly from the vagus without looping — at risk if not anticipated
- Preoperative CT/MRI showing aberrant subclavian should alert the surgeon
7. Parathyroid Glands

- Four glands: 2 superior + 2 inferior, on the deep (posterior) surface of the lateral thyroid lobes
- Position is variable: may range from carotid bifurcation to mediastinum
- Superior parathyroids (from 4th pharyngeal pouch) — more constant in position
- Inferior parathyroids (from 3rd pharyngeal pouch, with thymus) — more variable; may descend into mediastinum
Blood supply: Predominantly from the ascending branch of the inferior thyroid artery
📌 Surgical note: During total thyroidectomy, inadvertent removal or devascularization of parathyroids causes hypocalcaemia (tetany). To preserve parathyroids:
- Ligate the inferior thyroid artery branches close to the gland (not the trunk)
- Identify all four glands before ligation
- If devascularized, autotransplant into the sternomastoid or forearm
8. Ligament of Berry (Posterior Suspensory Ligament)
- Attaches the thyroid gland to the cricoid cartilage and upper tracheal rings on each side
- The RLN and branches of the inferior thyroid artery pass in close proximity (often through) this ligament
- Thickened and condensed pretracheal fascia
- The last structure divided during thyroid lobectomy — requires meticulous technique to avoid RLN injury
9. Thyroid Fascia
| Layer | Description |
|---|---|
| True (surgical) capsule | Thin, adherent to gland; sends septa in |
| False (surgical) capsule | Pretracheal fascia condensation |
| Space between capsules | Contains parathyroids, RLN, vessels — the surgical dissection plane |
10. Applied Surgical Aspects
Goitre Surgery
- Substernal goitre: Usually extends into the anterior mediastinum — 80% can be delivered through the cervical incision using blunt digital dissection; 5–10% require sternotomy
- Blood supply is from the cervical vessels (not intrathoracic), facilitating cervical extraction
Thyroidectomy Complications
| Complication | Cause | Presentation |
|---|---|---|
| Hoarseness | Unilateral RLN injury | Weak, husky voice |
| Aphonia/stridor | Bilateral RLN injury | Emergency; may need tracheostomy |
| Hypocalcaemia | Parathyroid injury/removal | Chvostek's and Trousseau's signs, perioral tingling |
| Thyroid storm | In untreated hyperthyroid patient | Hyperpyrexia, tachycardia, confusion |
| Haemorrhage | Vessel slip/ligation failure | Compressive haematoma → airway obstruction |
| Wound infection | Poor technique/contamination | Erythema, discharge |
| Air embolism | Neck vein injury | Sudden cardiovascular collapse |
Thyroid Cancer Surgery
- Papillary thyroid cancer (PTC): Near-total/total thyroidectomy ± central neck dissection (level VI); followed by radioactive iodine (RAI) ablation if indicated
- Follicular thyroid cancer: Hemi/total thyroidectomy (FNA cannot distinguish follicular adenoma from carcinoma — requires histology)
- Medullary thyroid cancer (MTC): Total thyroidectomy + central neck dissection; calcitonin levels monitored postoperatively
- Anaplastic thyroid cancer: Usually unresectable; palliative surgery/debulking for airway
- Encapsulated follicular variants of PTC are now reclassified as NIFTP (Noninvasive Follicular Thyroid Neoplasm with Papillary-like nuclear features) — treated more conservatively
Bethesda Classification (FNA Cytology)
| Category | Malignancy Risk | Recommendation |
|---|---|---|
| I — Nondiagnostic | 1–4% | Repeat FNA |
| II — Benign | ~3% false-negative | Follow-up |
| III — AUS/FLUS | 5–15% | Repeat FNA or molecular testing |
| IV — Follicular neoplasm | 15–35% | Lobectomy |
| V — Suspicious for malignancy | 60–75% | Lobectomy or near-total thyroidectomy |
| VI — Malignant | 97–99% | Near-total/total thyroidectomy |
Thyroid Imaging
- Radioiodine scan: "Cold" nodules (decreased uptake) carry ~20% malignancy risk; "hot" nodules <5%
- Ultrasound: First-line for nodule evaluation; guides FNAB
- CT/MRI: For substernal extension, tracheal/vascular involvement
- PET-CT: For Tg-positive, RAI-negative recurrent disease
Sources: Gray's Anatomy for Students (pp. 1157–1160); Schwartz's Principles of Surgery, 11th ed. (pp. 1625–1660)
This is a shared conversation. Sign in to Orris to start your own chat.