Leather bottle appearance in stomach
Reading File
Finding Sources
Searching the Web
linitis plastica leather bottle stomach pathology gastric cancer
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete, structured answer on the leather bottle (linitis plastica) appearance of the stomach.
Leather Bottle Stomach (Linitis Plastica)
Definition
"Leather bottle" or linitis plastica is a descriptive gross/radiological term for a stomach whose wall has been diffusely infiltrated by tumour, producing a rigid, non-distensible, thickened structure that resembles a leather bottle or flask. The name comes from the Latin linum (linen/flax) and plastica (moulded).
Underlying Pathology - Diffuse Gastric Adenocarcinoma
The classic cause is the diffuse type of gastric adenocarcinoma (Lauren classification). Key features:
| Feature | Detail |
|---|---|
| Growth pattern | Infiltrative - tumour permeates the entire gastric wall as small clusters and individual discohesive cells |
| Histology | Signet-ring cells - large mucin vacuoles push the nucleus to the periphery |
| Molecular basis | Loss of E-cadherin function (CDH1 mutations/methylation), causing cell discohesion |
| Desmoplastic reaction | Infiltrative cells trigger an intense fibrotic (scirrhous) stromal reaction that stiffens the wall |
| Gross result | Diffuse rugal flattening + rigid, thickened wall = leather bottle appearance |
"When there are large areas of infiltration, diffuse rugal flattening and a rigid, thickened wall may impart a leather bottle appearance termed linitis plastica."
- Robbins & Cotran Pathologic Basis of Disease
Gross Appearance
The image below (Panel B) shows the classic linitis plastica - the stomach wall is diffusely thickened, pale, and rigid with flattened, obliterated rugae, in contrast to Panel A (intestinal-type adenocarcinoma presenting as a bulky, ulcerated mass):
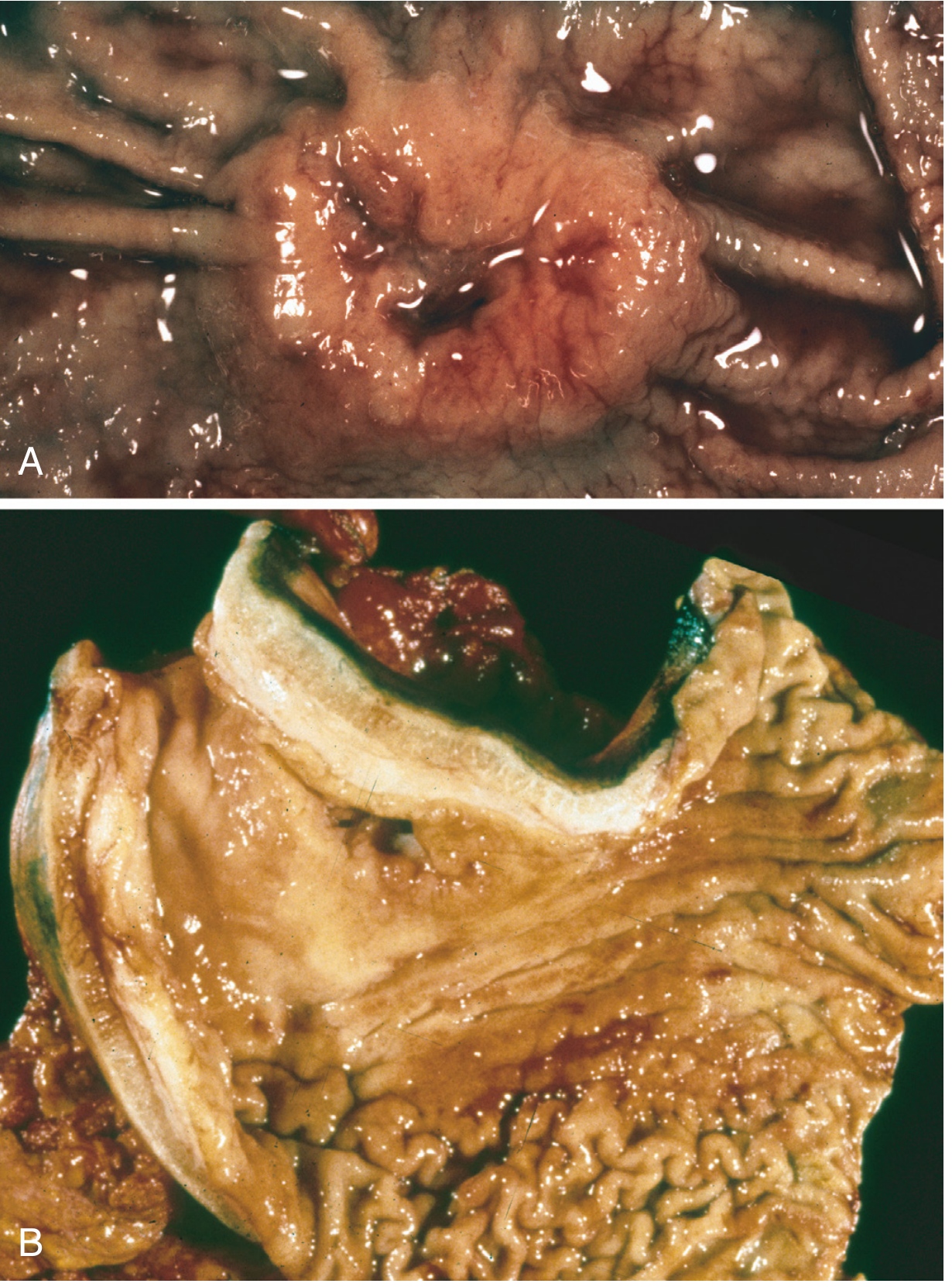
Fig. 17.20 - Robbins & Cotran: (A) Intestinal-type exophytic adenocarcinoma; (B) Diffuse-type infiltrative adenocarcinoma producing the leather bottle/linitis plastica appearance.
Radiological Features
On fluoroscopy (barium meal) - the preferred modality for appreciation:
- Stomach appears narrowed, tubular, and rigid
- Absent or markedly reduced peristalsis
- Failure to distend with gas/contrast
- Flattened or absent mucosal folds
On CT:
- Diffuse circumferential wall thickening (>6 mm)
- Loss of normal trilaminar architecture
- Perigastric fat stranding may indicate T4 disease
"Linitis plastica is a descriptive term for diffuse scirrhous tumour, where the stomach appears as a narrowed, rigid structure (leather bottle stomach) and is better appreciated in fluoroscopic imaging compared with endoscopy."
- Grainger & Allison's Diagnostic Radiology
Endoscopic Appearance
Endoscopy is often deceptively normal or subtle, because the tumour infiltrates submucosal/mural layers while sparing the mucosa initially. Features that may be seen:
- Thickened, non-pliable folds
- Poor distension even with air insufflation
- Mucosal erosion in advanced cases
- Biopsies may be falsely negative if superficial - deep/large biopsies or EUS-guided sampling may be needed
Other Causes of Linitis Plastica Pattern
While gastric adenocarcinoma is the most common cause, other conditions can mimic this appearance:
| Cause | Notes |
|---|---|
| Gastric lymphoma | Can produce diffuse wall thickening |
| Metastatic disease | Especially breast lobular carcinoma (haematogenous submucosal deposition) |
| Amyloidosis | Luminal narrowing from amyloid deposition in the wall |
| Sarcoidosis / Crohn's disease | Rare causes of gastric wall fibrosis |
| Caustic ingestion | Post-inflammatory fibrosis |
Clinical Features
- Symptoms: Early satiety (dominant), weight loss, dyspepsia, dysphagia, nausea
- Age: Mean ~40 years in familial CDH1 mutation carriers; older in sporadic cases
- Sex: Similar M:F ratio (unlike intestinal type which is 2:1 M:F)
- No geographic predilection - diffuse type is uniform worldwide (unlike intestinal type, which clusters in high-risk regions)
- No identified precursor lesion - hence typically diagnosed late
Prognosis
Linitis plastica carries a poor prognosis. Because the diffuse infiltrative pattern does not form a discrete mass, diagnosis is often delayed. Depth of invasion and nodal/distant metastases are the strongest prognostic indicators. For advanced disease, 5-year survival is less than 20%; patients with germline CDH1 mutations are often offered prophylactic gastrectomy.
Sources: Robbins & Cotran Pathologic Basis of Disease (Fig. 17.20); Robbins & Kumar Basic Pathology; Grainger & Allison's Diagnostic Radiology (Advanced Gastric Cancer section).
Crohn disease
Finding Sources
Searching the Web
Crohn disease pathology clinical features 2024
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Loading Image
Reading File
Now I have all the essential information from the textbooks. Here is the complete answer.
Crohn Disease
Definition & Overview
Crohn disease is a chronic, relapsing, transmural inflammatory bowel disease that can involve any segment of the GI tract from the mouth to the anus, though it most commonly affects the terminal ileum, ileocecal valve, and cecum. Together with ulcerative colitis (UC), it forms the entity of inflammatory bowel disease (IBD).
Epidemiology
- Most common in North America, northern Europe, and Australia; rising in Africa, Asia, and South America
- Typically presents in adolescents and young adults (peak onset 15-30 years; second smaller peak 50-70 years)
- 3-5x more common in Ashkenazi Jewish populations
- The hygiene hypothesis - reduced early-life microbial exposure may impair development of regulatory immune processes, predisposing to IBD
- Incidence is rising globally, possibly related to processed food additives and changing gut microbiome
Pathogenesis
IBD (including Crohn disease) results from the combined effects of:
-
Genetic susceptibility - over 200 risk alleles identified, accounting for <20% of disease risk
- NOD2 (chromosome 16) - encodes an intracellular sensor for muramyl dipeptide (a bacterial cell wall component); the most strongly associated gene in European populations. Three major risk alleles present in ~30% of Crohn patients vs 5% of healthy individuals
- NOD2 risk alleles are rare in Asian populations - hence Crohn disease is less common there
- Other important genes: PTPN22, IL10, IL10RA, IL10RB (monogenic very-early-onset IBD)
- IBD risk alleles overlap with type 1 diabetes, ankylosing spondylitis, and psoriasis
-
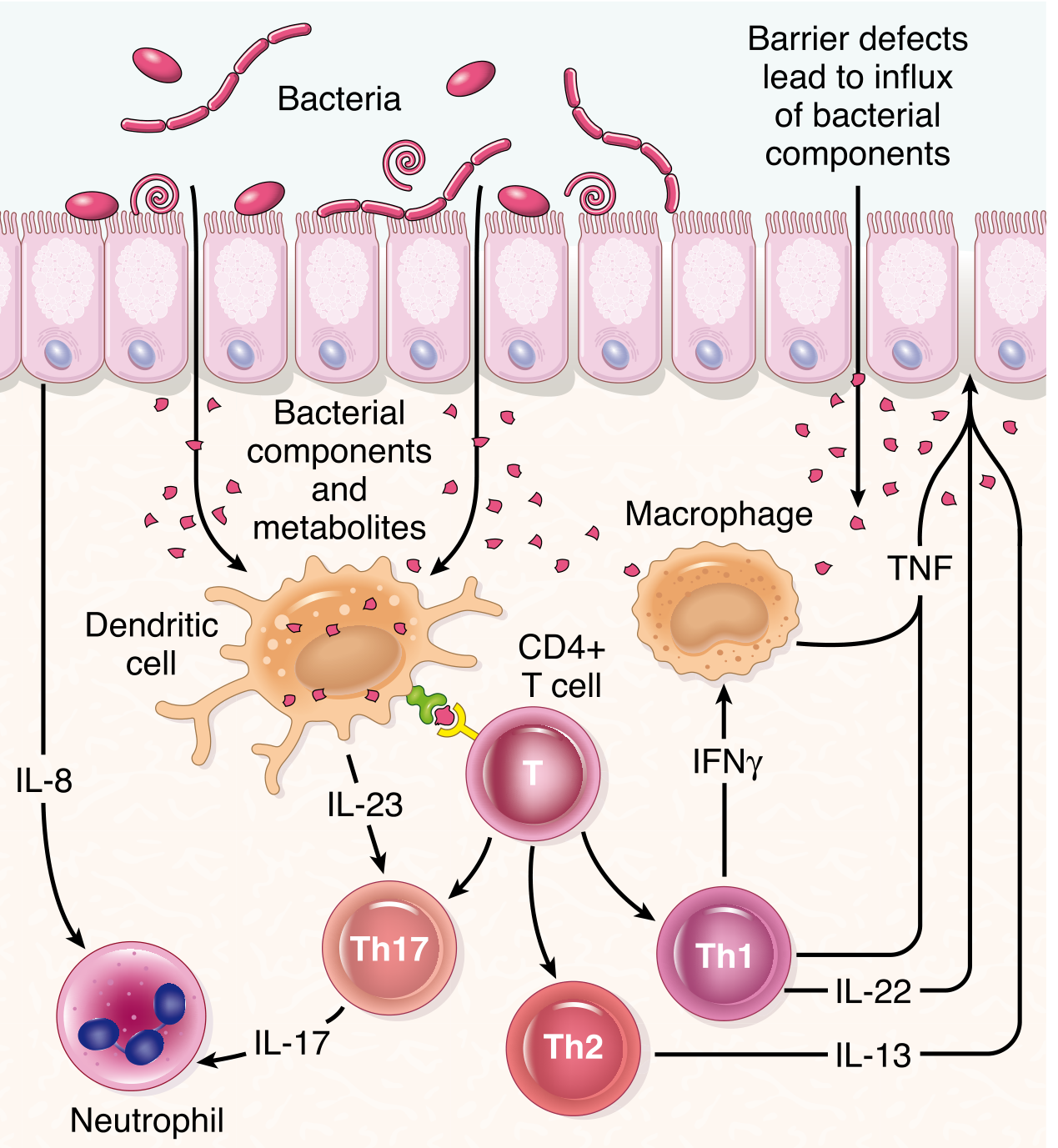
Aberrant mucosal immune responses - dysregulated Th1/Th17 responses with excess TNF-α, IL-12, IL-23, and IFN-γ
-
Intestinal epithelial dysfunction - impaired barrier function allows microbial translocation
-
Gut microbiome dysbiosis - reduced Faecalibacterium prausnitzii is associated with disease recurrence
Morphology
Distribution
- Small intestine only: ~40% of cases
- Small intestine + colon: ~30%
- Colon only: ~30%
- Can involve esophagus and stomach (infrequent)
Gross Pathology
Key gross features:
| Feature | Description |
|---|---|
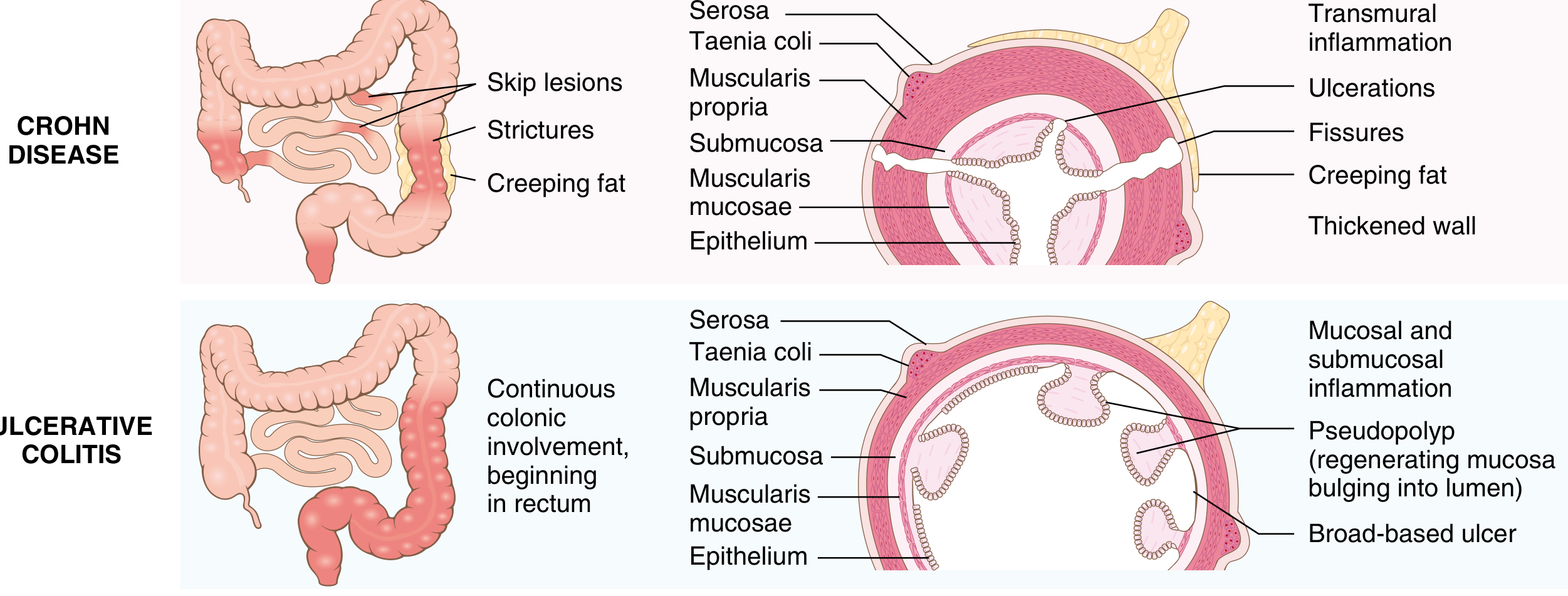
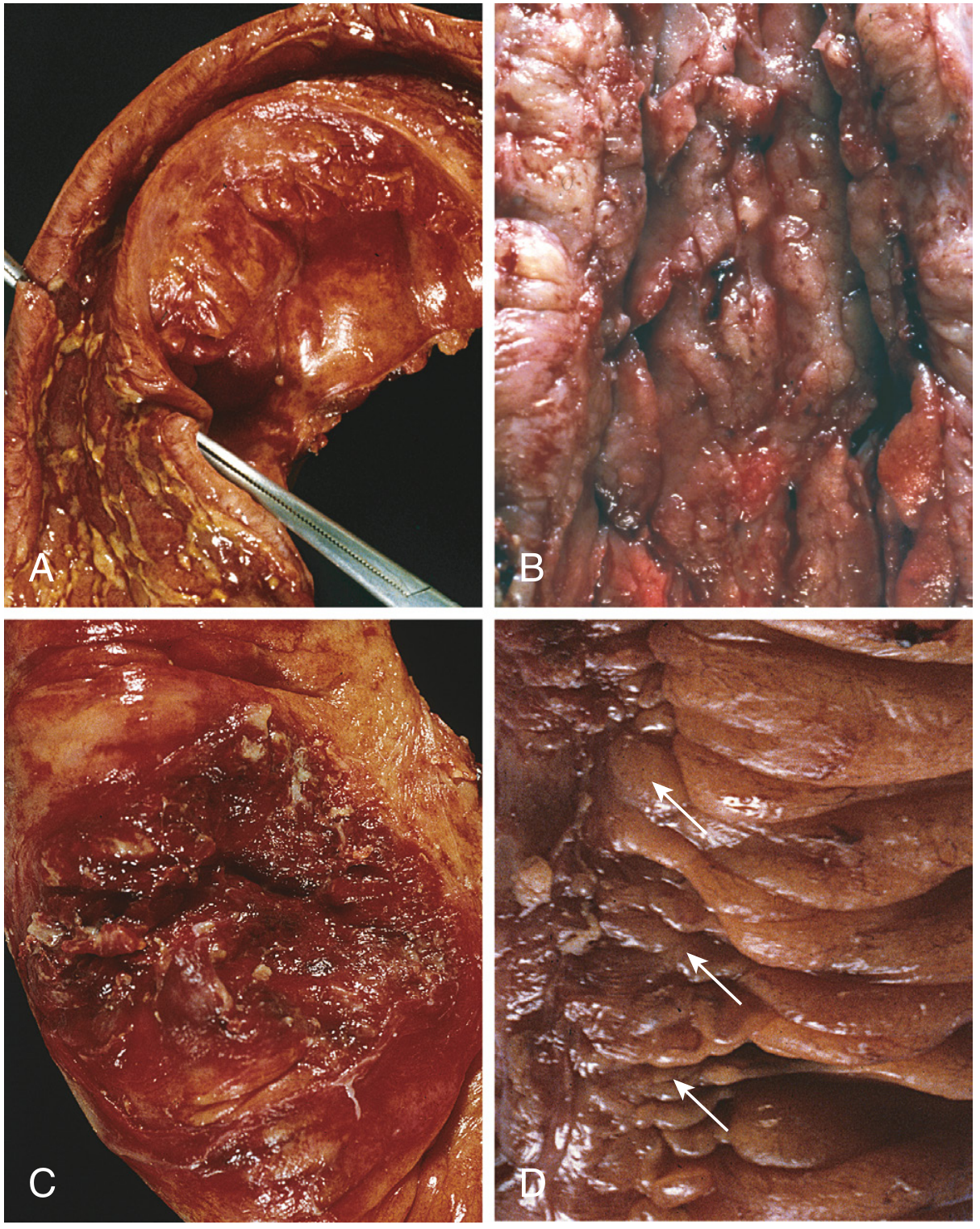
| Skip lesions | Multiple, sharply delineated involved segments separated by normal mucosa - the hallmark distinguishing Crohn from UC |
| Aphthous ulcers | Earliest lesion; progress to elongated serpentine ulcers along the long axis |
| Cobblestone mucosa | Ulceration with sparing of interspersed mucosa creates a cobblestone pattern |
| Fissures | Deep knife-like fissures that extend through the wall, forming abscesses or fistulas |
| Strictures | Wall thickening from edema, transmural inflammation, submucosal fibrosis, and muscularis propria hypertrophy |
| Creeping fat | Mesenteric adipose tissue wrapping over the serosal surface in areas of transmural disease |
| Thickened, rubbery wall | Palpably stiff bowel due to transmural inflammation and fibrosis |
Microscopic Pathology
- Transmural inflammation - the defining feature; lymphoid aggregates through all layers
- Crypt abscesses - clusters of neutrophils within crypts, with crypt destruction
- Crypt architectural distortion - haphazard branching crypts from repeated injury-regeneration cycles
- Noncaseating granulomas (epithelioid, non-caseating) - pathognomonic when present; found in ~35% of cases only; can occur in any wall layer, mesenteric lymph nodes, or even skin. Absence does NOT exclude the diagnosis
- Epithelial metaplasia - pseudopyloric (gastric antral-type) metaplasia; Paneth cell metaplasia in the left colon
- Abrupt transition between ulcerated and normal mucosa
Crohn Disease vs. Ulcerative Colitis - Key Differences
| Feature | Crohn Disease | Ulcerative Colitis |
|---|---|---|
| Bowel region | Ileum ± colon (any GI segment) | Colon only |
| Rectal involvement | Sometimes | Always (starts in rectum) |
| Distribution | Skip lesions | Diffuse, continuous |
| Inflammation | Transmural | Mucosa and submucosa only |
| Wall appearance | Thickened | Thin/normal |
| Ulcers | Deep, knife-like | Superficial, broad-based |
| Strictures | Common | Rare |
| Fistulas/sinuses | Yes | No |
| Granulomas | Yes (~35%) | No |
| Fibrosis | Marked | Mild to none |
| Serositis | Marked | Mild to none |
| Toxic megacolon | No | Yes |
| Perianal fistula | Yes (in colonic disease) | No |
| Fat/vitamin malabsorption | Yes (if small bowel involved) | No |
| Recurrence after surgery | Common | No (colectomy is curative) |
Clinical Features
Typical presentation:
- Intermittent attacks of crampy abdominal pain, low-grade fever, and diarrhea (often non-bloody)
- ~20% present acutely with right lower quadrant pain + fever, mimicking appendicitis
- Bloody diarrhea when colon is involved
- Relapsing-remitting course; triggers include physical/emotional stress, NSAIDs, smoking, specific foods
Complications:
| Complication | Notes |
|---|---|
| Fibrosing strictures | Especially terminal ileum; leads to obstruction |
| Fistulas | Entero-enteric, enterovesical, enterovaginal, perianal, cutaneous |
| Abscesses | Peritoneal, intra-abdominal |
| Perianal disease | Fistulas and abscesses in ~20% of cases |
| Malabsorption | Hypoalbuminemia, iron deficiency anemia, vitamin B12 deficiency (terminal ileal disease) |
| Colorectal/small bowel adenocarcinoma | Increased risk with long-standing colonic Crohn disease |
| Recurrence after surgery | ~40% require further resection within 10 years |
Extraintestinal manifestations (may precede bowel symptoms):
- Joints: Migratory polyarthritis, sacroiliitis, ankylosing spondylitis
- Eyes: Uveitis, episcleritis
- Skin: Erythema nodosum, pyoderma gangrenosum
- Liver/bile ducts: Pericholangitis, primary sclerosing cholangitis (more common in UC)
- Other: Clubbing of fingertips
Diagnosis
- Colonoscopy + biopsy - gold standard; shows skip lesions, aphthous ulcers, cobblestone mucosa, fissures
- CT/MRI enterography - evaluates extent, complications (abscesses, fistulas), comb sign (engorged peri-enteric vasculature in active disease)
- Serology: ASCA (anti-Saccharomyces cerevisiae antibodies) positive in 60-70% of Crohn patients
- Biomarkers: Elevated CRP, fecal calprotectin, fecal lactoferrin indicate active inflammation; CRP correlates with endoscopic activity
- Disease Activity Index: Crohn's Disease Activity Index (CDAI); remission = CDAI <150; response = decrease ≥100 points
Treatment
| Severity | Agents |
|---|---|
| Mild-moderate | Mesalazine (limited efficacy), budesonide (ileal/right-sided disease) |
| Moderate-severe | Systemic corticosteroids (short-term), azathioprine/6-mercaptopurine, methotrexate |
| Biologic therapy | Anti-TNF agents: infliximab, adalimumab, certolizumab pegol; Anti-integrins: vedolizumab; Anti-IL-12/23: ustekinumab |
| Refractory/complications | Surgery (resection of strictures, drainage of abscesses, repair of fistulas) |
- Surgery is not curative (unlike UC) - disease recurs at anastomotic sites; ~40% need repeat resection within 10 years
- Mucosal healing (endoscopic remission + normal biomarkers) is now a key therapeutic target beyond symptom control
Sources: Robbins & Cotran Pathologic Basis of Disease (Figs. 17.35-17.38); Robbins & Kumar Basic Pathology (Figs. 13.28-13.29); Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.