Drugs causing thrombocytopenia
Reading File
Finding Sources
Searching PubMed
"drug-induced thrombocytopenia" mechanisms management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive information to give a thorough, well-organized answer. Here it is:
Drug-Induced Thrombocytopenia (DITP)
Drug-induced thrombocytopenia is one of the most frequent causes of cytopenias evaluated by physicians. It can arise through several distinct mechanisms, and identifying the offending drug is the most important step in management.
Mechanisms
1. Immune-Mediated (Drug-Dependent Antibody)
The most common mechanism. The drug (or its metabolite) binds to a platelet surface glycoprotein, alters its conformation, and creates a "neoantigen." Drug-dependent antibodies form and bind this complex, leading to platelet destruction - primarily in the spleen. When the drug is removed, the neoantigen disappears and thrombocytopenia resolves.
- "Innocent bystander" mechanism (classic example: quinine/quinidine) - the platelet is coated with a drug-antibody complex, complement is fixed, and intravascular platelet lysis occurs.
- GPIIb/IIIa conformational change - drugs like abciximab, tirofiban, and eptifibatide induce conformational changes in glycoprotein IIb/IIIa, creating an immunogenic epitope.
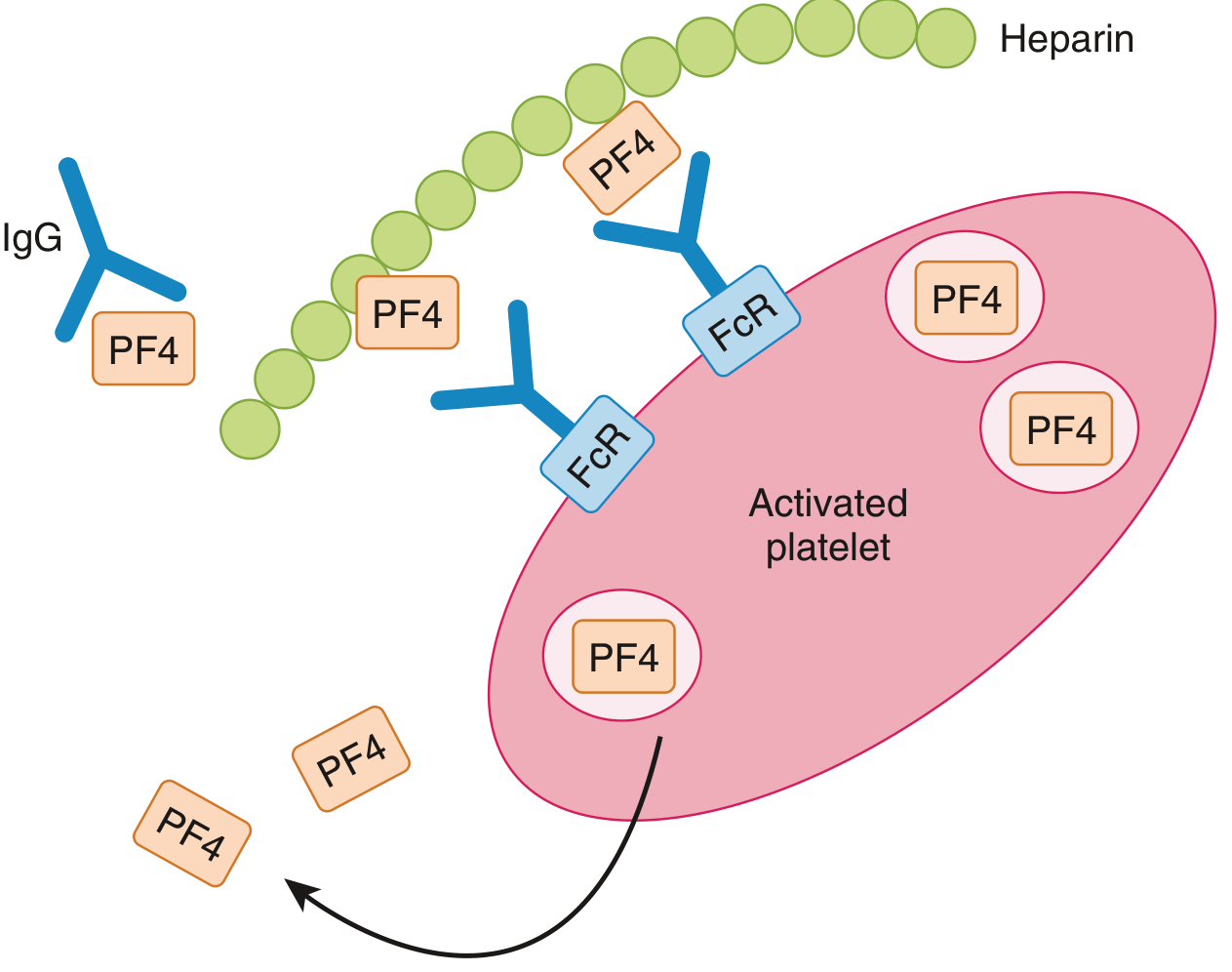
2. Heparin-Induced Thrombocytopenia (HIT) - Distinct Mechanism
HIT deserves its own category because it is uniquely prothrombotic rather than hemorrhagic.
- Type I HIT: Mild, occurs rapidly after onset of heparin, likely due to direct platelet-aggregating effect. Little clinical importance; may resolve even if heparin is continued.
- Type II HIT: Life-threatening. Occurs 5-14 days after starting heparin (or sooner with prior sensitization). Caused by IgG antibodies against the heparin-PF4 complex. These antibodies bind FcγRII receptors on platelets, causing platelet activation, aggregation, and simultaneous activation of coagulation pathways - leading to paradoxical thrombosis even while platelets are low.
3. Bone Marrow Suppression (Non-Immune)
Chemotherapy and other myelotoxic agents reduce platelet production directly by suppressing megakaryopoiesis, independent of immune mechanisms.
Drugs Strongly Associated With Thrombocytopenia
Antibiotics & Antivirals
| Drug | Notes |
|---|---|
| Quinine / Quinidine | Classic offenders; "innocent bystander" mechanism; even quinine in tonic water can trigger severe DITP ("gin and tonic purpura") |
| Vancomycin | Drug-dependent antibody to platelet glycoproteins |
| Trimethoprim-sulfamethoxazole | Immune-mediated; life-threatening |
| Sulfonamides | Notorious for severe, prolonged thrombocytopenia |
| Penicillin / Cephalosporins | Immune-mediated |
| Rifampin | Immune-mediated |
| Linezolid | Direct bone marrow suppression + immune |
| Valacyclovir / Ganciclovir | Myelosuppressive |
| Indinavir (and other protease inhibitors) | Immune-mediated |
Cardiovascular Medications
| Drug | Notes |
|---|---|
| Heparin (UFH > LMWH) | HIT (Type II) - thrombotic, not hemorrhagic |
| Abciximab, Tirofiban, Eptifibatide (GPIIb/IIIa inhibitors) | Immune-mediated via conformational change in GPIIb/IIIa |
| Digoxin | Immune-mediated |
| Furosemide | Immune-mediated |
| Salicylates / NSAIDs | Immune-mediated (also platelet function impairment) |
Neurological / Psychiatric
| Drug | Notes |
|---|---|
| Valproate | Bone marrow suppression |
| Phenytoin | Immune-mediated |
| Carbamazepine | Immune-mediated |
Gastrointestinal
| Drug | Notes |
|---|---|
| Cimetidine, Ranitidine, Famotidine (H2 blockers) | Immune-mediated |
Oncology
| Drug | Notes |
|---|---|
| Oxaliplatin | Immune-mediated; drug-dependent antibody |
| Chemotherapy (in general) | Bone marrow suppression |
| Checkpoint inhibitors | Immune-mediated |
| Interferon | Bone marrow suppression |
Differentiating DITP from ITP
| Feature | DITP | ITP |
|---|---|---|
| Onset | Abrupt, days to weeks after starting a new drug | Gradual, over months to years |
| Recovery | Resolves within 1-7 days of stopping drug | Persists without treatment |
| History | Clear temporal link to new medication | No drug correlation |
| Thrombosis | Absent (except HIT) | Absent |
HIT Risk Stratification: The 4Ts Score
| Category | 2 pts | 1 pt | 0 pts |
|---|---|---|---|
| Thrombocytopenia | Fall >50%, nadir ≥20k | Fall 30-50% or nadir 10-19k | Fall <30% or nadir <10k |
| Timing | Clear onset days 5-10 | Consistent with days 5-10 but uncertain | Fall <4 days without recent exposure |
| Thrombosis | New confirmed thrombosis or skin necrosis | Progressive thrombosis or skin lesions | None |
| Other causes | None apparent | Possible | Definite |
- Score <3: Low probability
- Score 4-5: Intermediate probability
- Score 6-8: High probability
Management
General DITP
- Stop all suspected offending drugs - the platelet count typically begins to improve within 1-2 days and normalizes within 1 week.
- For profound thrombocytopenia (<10,000-15,000/µL) or active bleeding: platelet transfusion.
- If ITP cannot be excluded in life-threatening cases: corticosteroids and/or IVIG are options.
- Note: drugs with long half-lives (sulfonamides, quinine, quinidine) may cause more prolonged courses.
HIT-Specific Management
- Immediately stop ALL heparin - including heparin flushes and LMWH (which can cross-react).
- Do NOT give warfarin initially - it decreases protein C and worsens thrombosis risk; avoid until platelets recover to ≥150,000.
- Start a non-heparin anticoagulant immediately:
- Argatroban (direct thrombin inhibitor) - FDA-approved for HIT; preferred in most cases. Dose: 2 mcg/kg/min IV (reduce to 0.5-1.2 mcg/kg/min in hepatic dysfunction). Monitor aPTT to 1.5-3x baseline.
- Bivalirudin - preferred with bleeding risk, critical illness, or urgent surgery.
- Fondaparinux - an alternative (not FDA-approved for HIT but widely used).
- DOACs (rivaroxaban, apixaban, dabigatran) - increasing evidence supports their use.
- Danaparoid - available outside the US.
- Continue anticoagulation for at least 2-3 months (no thrombosis) or 3-6 months (with thrombosis).
- IVIG may be considered for severe HIT.
Sources: Robbins & Cotran Pathologic Basis of Disease | Goldman-Cecil Medicine | Rosen's Emergency Medicine | Andrews' Diseases of the Skin
Cefotaxime in thrombocytopenia
Finding Sources
Searching PubMed
cefotaxime thrombocytopenia
Reading File
Finding Sources
Searching PubMed
cefotaxime "immune thrombocytopenia" OR "drug-induced thrombocytopenia" cephalosporin
Reading File
Reading Article
PMID: 28074730
Finding Sources
Searching PubMed
cephalosporin "drug-induced immune thrombocytopenia" antibody mechanism neonates
Now I have enough information to give a thorough, clinically useful answer.
Cefotaxime and Thrombocytopenia
The relationship between cefotaxime and thrombocytopenia has two distinct clinical dimensions: (1) cefotaxime as a cause of thrombocytopenia, and (2) cefotaxime used in clinical settings where thrombocytopenia is already present (e.g., neonatal sepsis, meningitis).
1. Cefotaxime as a Cause of Thrombocytopenia
Mechanism
Cefotaxime, like other cephalosporins, can cause thrombocytopenia through immune-mediated mechanisms. The drug or its metabolite binds to platelet surface glycoproteins, alters their conformation, and creates a neoantigen. Drug-dependent antibodies then form and destroy these opsonized platelets, primarily in the spleen.
This is listed explicitly as a known adverse effect: toxicities of cefotaxime include allergy, neutropenia, thrombocytopenia, and eosinophilia, along with a false-positive direct Coombs test - the latter reflecting the same immune mechanism acting on red cells as well as platelets. - Harriet Lane Handbook, 23rd ed.
Cefotaxime and Coagulation (PT Prolongation)
Beyond thrombocytopenia, cefotaxime also has a separate hemostatic effect: it inhibits vitamin K-dependent coagulation factor synthesis, which can prolong the prothrombin time (PT). Other cephalosporins with this effect include cefamoxazole and cefoperazone. This is distinct from thrombocytopenia but compounds bleeding risk. - Tintinalli's Emergency Medicine
Cephalosporin Class Effect
Thrombocytopenia is a recognized class effect across cephalosporins. Other members with documented DITP include:
- Ceftriaxone - probably the best-documented cephalosporin causing DITP, with multiple case reports and even fatal hemolytic episodes
- Cefepime - immune-mediated thrombocytopenia (case series published 2023, PMID 37927729)
- Piperacillin/tazobactam - well-documented, with published drug challenge cases
Cefotaxime shares this potential, though the literature is more limited compared to ceftriaxone and cefepime.
Clinical Course of Cephalosporin-DITP
- Onset: typically days to a few weeks after starting the drug (immune sensitization lag period)
- Platelet count can fall below 10,000/mm³ in severe cases
- Spontaneous recovery after stopping the drug, usually within 1-7 days
- May be confused with ITP or the thrombocytopenia of the underlying infection being treated
- Rechallenge is not recommended (thrombocytopenia will recur)
2. Cefotaxime Used When Thrombocytopenia is Already Present
This is actually the more common clinical scenario. Cefotaxime is a first-line antibiotic for several serious infections where thrombocytopenia is a presenting feature or complication:
| Indication | Thrombocytopenia context |
|---|---|
| Neonatal sepsis | Thrombocytopenia is common in neonatal sepsis (bacterial, CMV, toxoplasma, HSV); cefotaxime ± ampicillin or gentamicin is standard first-line therapy |
| Bacterial meningitis | Septicemia-associated thrombocytopenia or DIC may be present |
| HSV neonatal infection | Thrombocytopenia is a hallmark feature; if skin vesicles, CSF pleocytosis, leukopenia, hepatitis, or thrombocytopenia are present, HSV must be considered alongside bacterial infection |
| Gram-negative sepsis | Thrombocytopenia from DIC, endotoxin-mediated platelet consumption |
In these settings, thrombocytopenia worsening during cefotaxime therapy creates a diagnostic dilemma: is it disease progression, DIC, or drug-induced DITP?
3. Distinguishing Drug-Induced vs. Disease-Related Thrombocytopenia
| Feature | Drug-Induced (DITP) | Sepsis/Infection-Related |
|---|---|---|
| Timing | Thrombocytopenia develops or worsens after starting the drug | Present from onset, often improving with treatment |
| Trend | Worsens progressively with ongoing drug use | Improves as infection resolves |
| Response to stopping drug | Platelet count improves within 1-7 days | Does not respond to stopping antibiotic alone |
| Other cytopenias | Isolated thrombocytopenia common | Often pancytopenia or leukocytosis |
| Coagulation | Normal PT/aPTT (pure DITP) | Often abnormal if DIC present |
4. Management
- If cefotaxime-induced DITP is suspected: stop the drug; substitute with a non-cephalosporin antibiotic appropriate for the indication (e.g., meropenem, aztreonam for Gram-negative cover, depending on organism and sensitivity).
- For severe thrombocytopenia (<10,000-15,000/µL) or active bleeding: platelet transfusion.
- IVIG or corticosteroids if ITP cannot be excluded or thrombocytopenia is life-threatening.
- Note: the PT prolongation from cefotaxime (vitamin K inhibition) is treated with vitamin K supplementation.
Bottom line: Cefotaxime is a recognized (though not the most commonly cited) cause of immune-mediated thrombocytopenia as a class effect of cephalosporins. More often clinically, it is used to treat infections in which thrombocytopenia is already present - requiring careful monitoring to distinguish disease-related from drug-induced platelet drops.
Sources: Harriet Lane Handbook 23rd ed. | Tintinalli's Emergency Medicine | Goldman-Cecil Medicine | Red Book 2021
Cefoperazone and sulbactum in thrombocytopenia
Finding Sources
Searching PubMed
cefoperazone sulbactam thrombocytopenia
Reading Article
PMID: 39253607
Reading Article
PMID: 36967671
Reading Article
PMID: 34497130
Reading File
Reading Article
PMID: 35347732
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from both textbooks and recent clinical studies. Here is a detailed answer:
Cefoperazone-Sulbactam (Sulperazon) and Thrombocytopenia
Cefoperazone-sulbactam is a combination of a third-generation cephalosporin (cefoperazone) and a beta-lactamase inhibitor (sulbactam). It has two distinct mechanisms by which it affects hemostasis and can cause thrombocytopenia, making it one of the more hemostasis-relevant antibiotics in clinical practice.
Mechanism 1: Immune-Mediated Thrombocytopenia (Direct DITP)
Like other beta-lactam antibiotics, cefoperazone-sulbactam can cause drug-induced immune thrombocytopenia (DITP). The drug or its metabolite binds to platelet surface glycoproteins, alters their conformation, and creates a neoantigen. Drug-dependent IgG antibodies form and destroy these opsonized platelets via splenic macrophages.
Key Clinical Evidence
Large real-world retrospective study (Zhu et al., 2024, PMID 39253607) - 6,489 patients treated with cefoperazone-sulbactam at Beijing Hospital over 6 years:
- Incidence: 2.4% (155/6,489 patients) developed thrombocytopenia
- Despite the relatively low incidence, cases could be severe and complicated by hemorrhage
- Multivariate analysis identified the following independent risk factors:
| Risk Factor | Threshold |
|---|---|
| Duration of cefoperazone-sulbactam therapy | >14 days |
| Baseline platelet count | <200 × 10⁹/L |
| Daily dose | ≥6 g/day |
| Total bilirubin | >21 µmol/L (hepatic dysfunction) |
| AST | >35 U/L (liver injury) |
| Use of non-invasive ventilator | (critical illness marker) |
Dramatic acute case (Lv et al., 2023, PMID 34497130) - Patient developed acute reactive thrombocytopenia with a platelet count fall from 168 × 10⁹/L to 1 × 10⁹/L within just 29 hours of sulperazon (cefoperazone-sulbactam) exposure during treatment of SLE. The drug was stopped, IVIG was given for 6 days, and platelets recovered fully with no major complications except petechiae.
Mechanism 2: N-Methylthiotetrazole (NMTT) Side Chain - Hypoprothrombinemia and Bleeding
This is the more pharmacologically distinctive and clinically important mechanism unique to cefoperazone.
Cefoperazone contains an N-methylthiotetrazole (NMTT) side chain - the same structural moiety found in cefamandole, cefmetazole, and cefotetan. This side chain:
- Inhibits vitamin K-dependent coagulation factor synthesis - prolongs the prothrombin time (PT/INR)
- Causes a disulfiram-like reaction when alcohol is consumed concomitantly
- These effects compound the bleeding risk when thrombocytopenia is also present
"Cephalosporins containing a thiotetrazole group (cefoperazone, cefotetan, cefamandole) can prolong the prothrombin time, an effect that may be associated with clinically significant bleeding among patients receiving anticoagulation or with vitamin K deficiency." - Goodman & Gilman's Pharmacological Basis of Therapeutics
"Hypoprothrombinemia is frequent with cephalosporins that have a methylthiotetrazole group (eg, cefamandole, cefmetazole, cefotetan, and cefoperazone)." - Jawetz Medical Microbiology 28th ed.
Prevention: Oral vitamin K, 10 mg twice weekly, can prevent NMTT-mediated hypoprothrombinemia. - Katzung's Basic & Clinical Pharmacology, 16th ed.
Mechanism 3: Cross-Reactivity with Other Beta-Lactams
A notable case report (He et al., 2023, PMID 36967671) demonstrated cross-reactivity of platelet-specific antibodies between piperacillin-tazobactam and cefoperazone-sulbactam:
- A 79-year-old patient developed DITP on piperacillin-tazobactam
- After recovery and switch to meropenem, thrombocytopenia recurred on cefoperazone-sulbactam
- This implies shared structural epitopes between the two beta-lactam combinations that can trigger the same platelet-reactive antibody
Clinical implication: If a patient develops DITP on one beta-lactam combination (e.g., piperacillin-tazobactam), substituting cefoperazone-sulbactam may not be safe - cross-reactivity is possible.
Summary of Hemostatic Effects
| Effect | Mechanism | Clinical Result |
|---|---|---|
| Thrombocytopenia | Immune-mediated (drug-dependent antibody) | Low platelets, bleeding risk |
| Hypoprothrombinemia | NMTT side chain inhibits vitamin K | Prolonged PT/INR, bleeding risk |
| Disulfiram-like reaction | NMTT side chain | Flushing, hypotension, tachycardia with alcohol |
| Cross-reactive DITP | Shared antibody epitope with other beta-lactams | Recurrent thrombocytopenia if switched |
When Cefoperazone-Sulbactam is Used Despite Thrombocytopenia
Because of its excellent Gram-negative and anaerobic coverage (including Acinetobacter baumannii and Pseudomonas aeruginosa), cefoperazone-sulbactam is often the drug of choice in critically ill patients who may already have thrombocytopenia from sepsis, DIC, or their underlying illness. In such cases:
- Baseline platelet count and PT/INR must be checked before starting
- Monitor platelets closely, especially if therapy extends beyond 14 days
- Supplement with vitamin K prophylactically to prevent NMTT-mediated PT prolongation
- Be aware that the drug itself may worsen existing thrombocytopenia
- If platelets fall significantly during therapy, consider whether DITP is contributing versus the underlying illness
Management of Cefoperazone-Sulbactam-Induced Thrombocytopenia
- Stop the drug - platelet count should begin to recover within 1-7 days
- For platelet count <10,000-15,000/µL or active bleeding: platelet transfusion
- IVIG (as shown in the SLE case above) for severe immune-mediated thrombocytopenia
- Do not re-challenge - thrombocytopenia will recur
- Choose an alternative antibiotic that avoids beta-lactam cross-reactivity if possible (e.g., meropenem, colistin, tigecycline depending on the organism)
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics | Katzung's Basic & Clinical Pharmacology 16th ed. | Jawetz Medical Microbiology 28th ed. | Dermatology 5th ed. (Dermatol Bolognial) | Zhu et al. 2024 (PMID 39253607) | He et al. 2023 (PMID 36967671) | Lv et al. 2023 (PMID 34497130)
This is a shared conversation. Sign in to Orris to start your own chat.