Lung abscess
Reading File
Finding Sources
Searching PubMed
"lung abscess"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have rich, comprehensive information from multiple authoritative sources. Let me compose the full answer.
Lung Abscess
Lung abscess is defined as a localized area of necrosis and suppuration within the pulmonary parenchyma, typically forming one or more cavities >2 cm in diameter following microbial infection.
Classification
| Type | Description |
|---|---|
| Primary (~80%) | Arises from aspiration in a normal host; often anaerobic, polymicrobial |
| Secondary (~20%) | Complicates an underlying condition - obstruction (tumor, foreign body), immunocompromise, septic emboli |
| Acute | <4-6 weeks duration |
| Chronic | >4-6 weeks duration (~40% of cases) |
| Putrid | Foul-smelling, associated with anaerobes |
Etiology and Microbiology
Primary Lung Abscess
The dominant organisms are anaerobes from the gingival crevices - present in up to 93% of cases and sole isolates in 46%:
- Prevotella spp.
- Fusobacterium spp.
- Bacteroides spp. (usually not B. fragilis)
- Peptostreptococcus spp.
- Microaerophilic / milleri group streptococci (S. anginosus)
Secondary / Aerobic / Special Settings
| Setting | Pathogens |
|---|---|
| Necrotizing pneumonia | S. aureus, K. pneumoniae, S. pyogenes, Pseudomonas aeruginosa |
| Immunocompromised | P. aeruginosa, Nocardia, Aspergillus, Cryptococcus, Mucorales |
| Septic emboli / endocarditis | S. aureus, Fusobacterium necrophorum (Lemierre's syndrome) |
| Hematogenous spread | S. aureus - multiple bilateral abscesses |
| Mimic/co-infect cavities | M. tuberculosis, NTM, Histoplasma, Blastomyces, Coccidioides, Entamoeba histolytica, Paragonimus westermani, Echinococcus |
Important note: Metronidazole alone is NOT adequate - it misses microaerophilic streptococci which are often part of the mixed flora.
Pathogenesis and Risk Factors
The classic pathway is:
- Colonization of gingival crevices by anaerobes (periodontal disease is a major risk factor - lung abscesses are rare in edentulous patients)
- Aspiration of infected oral material
- Inflammation → tissue necrosis → cavitation (typically takes 1-2 weeks)
- Cavity may communicate with a bronchus, producing the classic air-fluid level
Risk factors for aspiration:
- Altered mental status (alcoholism, seizures, drug overdose, anesthesia)
- Bulbar dysfunction, neuromuscular disease
- Prior stroke / cardiovascular events
- Esophageal dysmotility, strictures, or tumors
- Gastroesophageal reflux, recumbent position
Location
Because aspiration occurs in the recumbent position and the right main bronchus is more vertical, abscesses preferentially form in:
- Posterior segment of the right upper lobe (most common)
- Apical segments of the lower lobes (especially right)
- Multiple / bilateral / basal - suggests hematogenous seeding or complicating pneumonia/bronchiectasis
Clinical Features
The course is typically indolent, developing over weeks to months:
- Fever, cough, purulent or foul-smelling sputum (putrid smell is pathognomonic of anaerobic infection)
- Pleuritic chest pain
- Constitutional symptoms: night sweats, weight loss, anemia (chronic systemic illness appearance)
- Hemoptysis (can be life-threatening)
- Signs of consolidation on exam
Diagnosis
Imaging
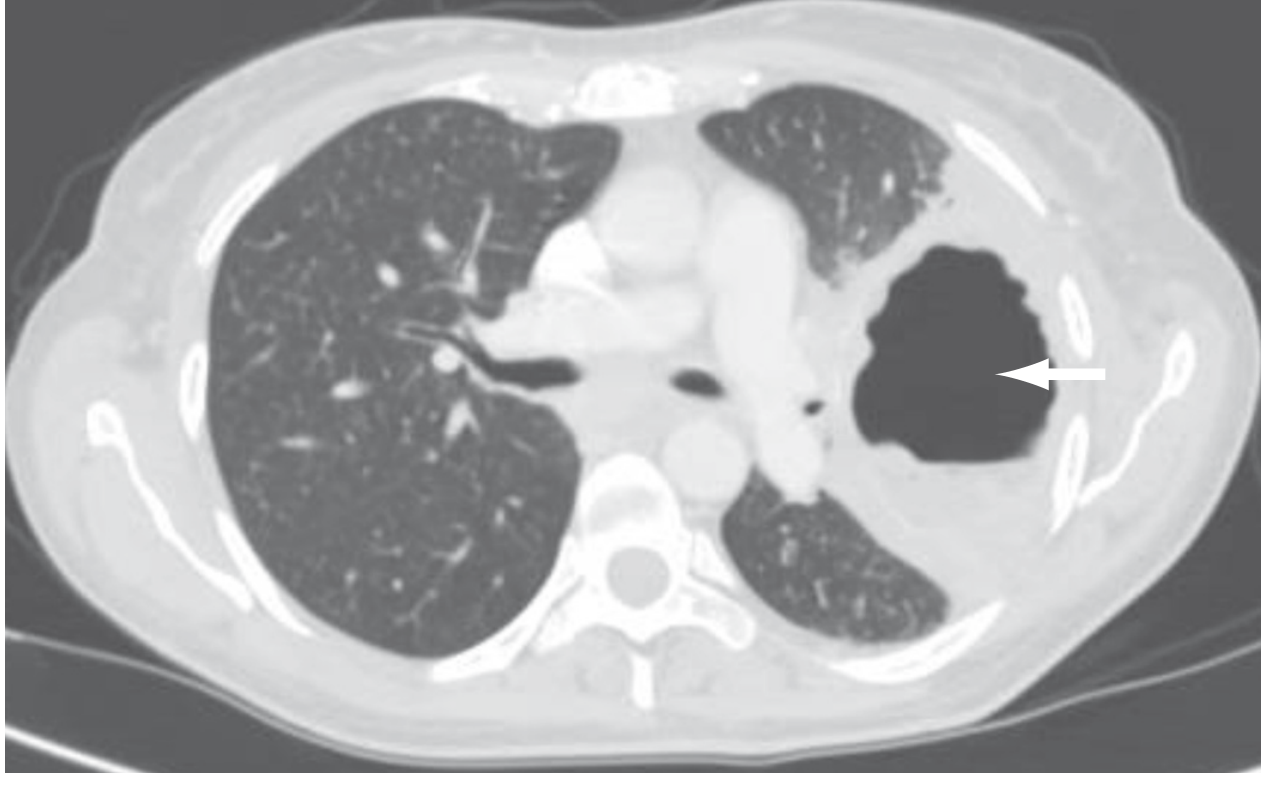
- Chest X-ray: cavitating infiltrate with air-fluid level, typically in a dependent segment
- CT chest (preferred): better defines cavitation, wall thickness, distinguishes parenchymal abscess from pleural empyema (critical distinction - managed very differently), identifies associated mass lesions
Differential Diagnosis of Cavitary Lung Lesions
(Tintinalli's Table 66-2)
- Infectious: anaerobic/aerobic abscess, TB, actinomycosis, fungal (coccidio, histo, blasto, aspergillus, crypto), parasitic (echinococcosis, amebiasis, Paragonimus)
- Neoplastic: bronchogenic carcinoma (squamous cell >> others), metastatic (colorectal, renal), lymphoma
- Inflammatory: Wegener's granulomatosis (GPA), sarcoidosis
- Other: infected bulla, empyema, foreign body
Microbiological Workup
- Blood cultures
- Sputum Gram stain + culture (limited - oral contamination)
- Bronchoscopy with BAL - especially when secondary abscess suspected, to rule out obstruction, or when empirical therapy fails
- Transthoracic needle aspiration (in selected cases)
- Pleural fluid culture if effusion present
Treatment
Antibiotics (Primary Lung Abscess)
First-line options:
| Regimen | Detail |
|---|---|
| Clindamycin (preferred over penicillin alone) | 600 mg IV q8h → step down to 300 mg PO q6h when afebrile |
| Ampicillin-sulbactam (IV) | Then amoxicillin-clavulanate PO |
| Carbapenem (ertapenem, imipenem) | For severe or hospital-acquired cases |
| Moxifloxacin 400 mg/d PO | Small study showed non-inferiority to ampicillin-sulbactam |
Clindamycin proved superior to penicillin in clinical trials due to β-lactamase production by oral anaerobes. Metronidazole alone is inadequate.
Duration: Controversial - typically 3-6 weeks minimum, continuing until imaging confirms resolution or regression to a small scar. At least 6 weeks may be associated with better outcomes.
For secondary abscesses, therapy is targeted to the identified pathogen (often prolonged) + treatment of the underlying cause.
Non-antibiotic Interventions
- Bronchoscopy - assists cavity drainage; also used to relieve obstruction or obtain cultures
- Percutaneous drainage - for patients failing antibiotics who are poor surgical candidates; risks include empyema, pneumothorax, hemothorax
- Surgical resection (lobectomy) - indicated for:
- Persistent cavity ≥2 cm with thick walls
- Failure to clear sepsis after 8 weeks of medical therapy
- Life-threatening hemoptysis
- Abscess >6 cm (less likely to respond to antibiotics)
- Suspected malignancy
85-95% of patients respond to medical management, with complete healing in 3-4 months.
Complications
- Empyema - extension to pleural space (dreaded; requires drainage)
- Life-threatening hemoptysis
- Massive aspiration of abscess contents
- Bronchiectasis or persistent pneumatoceles (especially with large abscesses)
- Recurrence despite appropriate therapy
- Bronchopleural fistula
Prognosis
| Group | Mortality |
|---|---|
| Primary abscess | ~2% |
| Secondary abscess | Up to 75% (some series) |
Poor prognostic factors:
- Age >60
- Malignancy-related abscess
- Aerobic gram-negative organisms
- Sepsis at presentation
- Symptom duration >8 weeks before treatment
- Abscess size >6 cm
- Symptoms >3 months before treatment / cavity >4-6 cm (less likely to respond to medical management)
Lemierre's Syndrome (Special Entity)
Caused by Fusobacterium necrophorum, typically following oropharyngeal infection in adolescents/young adults. Septic thrombophlebitis of the internal jugular vein → septic emboli → multiple lung abscesses. Treatment includes prolonged antibiotics (β-lactam/β-lactamase inhibitor or metronidazole) ± anticoagulation.
Sources: Harrison's Principles of Internal Medicine 22E (2025) | Sabiston Textbook of Surgery | Fishman's Pulmonary Diseases and Disorders | Robbins & Kumar Basic Pathology | Tintinalli's Emergency Medicine
Recent literature (2025-2026): A 2026 review in Thorac Surg Clin (PMID 42336503) specifically covers surgical management for necrotizing pneumonia and lung abscess. A 2025 review in FP Essent (PMID 40094493) updates the primary care approach to lung abscess and pleural effusion - no major departures from established guidelines were identified.
Summy clinical anatomy
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.