GERD in git
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have enough to give a thorough answer. Here is a comprehensive overview of GERD:
Gastroesophageal Reflux Disease (GERD)
Definition
GERD develops when the reflux of stomach contents into the esophagus causes troublesome symptoms or complications. Physiologic reflux occurs in healthy individuals; it becomes pathologic when it overwhelms or disrupts the normal defense mechanisms.
Epidemiology
- Prevalence: 10–20% in the Western world, <5% in Asia
- In the US, up to 44% of people report ever having GERD symptoms; ~30% had symptoms in the prior week
- Higher prevalence in North America > Europe, and northern > southern Europe
- Risk factors: obesity (especially central), increasing age, positive family history
- Genetic contribution: more common in monozygotic than dizygotic twins
Pathophysiology
Normal defense has three layers:
- Antireflux barrier at the gastroesophageal junction — lower esophageal sphincter (LES), crural diaphragm, phrenoesophageal ligament, and angle of His
- Esophageal clearance — peristalsis clears volume; weakly alkaline saliva neutralizes residual acid
- Epithelial defense — pre-epithelial (bicarbonate/unstirred water layer), epithelial (tight junctions, ion transporters), and postepithelial (blood supply)
Mechanisms of failure:
- Transient LES relaxations (tLESRs) — the primary mechanism; vagally mediated, triggered by gastric distention
- Low resting LES pressure — allows reflux when intra-abdominal pressure rises
- Hiatal hernia — spatially separates the LES from the crural diaphragm, acts as a reservoir, reduces LES pressure
- Obesity — increased intra-abdominal fat raises intragastric pressure, increases tLESRs frequency, and predisposes to hiatal hernia
- Acid pocket — unbuffered acid in the gastric cardia, displaced into a hiatal hernia, is the source of postprandial acid reflux
- Impaired peristalsis — contractions <20 mmHg are ineffective for clearance; worsens with esophagitis severity
- Reduced saliva — smoking, Sjögren syndrome impair neutralization
Damage occurs when acid and acidified pepsin breach intercellular junctions → dilate intercellular spaces → trigger chemokine release → attract inflammatory cells.
Montreal Classification
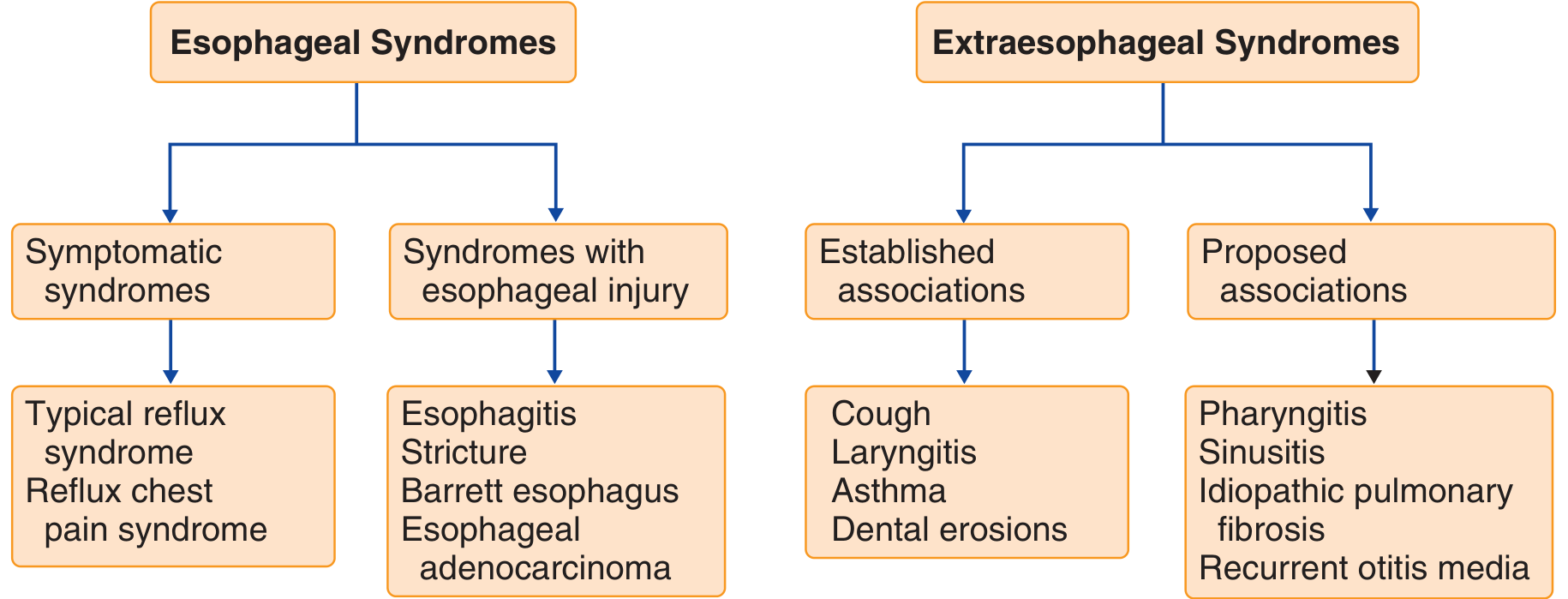
Esophageal syndromes:
- Symptomatic: typical reflux syndrome, reflux chest pain syndrome
- With esophageal injury: esophagitis, stricture, Barrett esophagus, esophageal adenocarcinoma
Extraesophageal syndromes:
- Established associations: cough, laryngitis, asthma, dental erosions
- Proposed associations: pharyngitis, sinusitis, idiopathic pulmonary fibrosis, recurrent otitis media
Clinical Manifestations
| Category | Symptoms |
|---|---|
| Classic (esophageal) | Heartburn, acid regurgitation |
| Atypical (esophageal) | Chest pain, dysphagia, odynophagia |
| Extraesophageal | Chronic cough, laryngitis, asthma, dental erosions |
Extraesophageal symptoms are more reliably attributed to GERD when they are accompanied by classic symptoms and confirmed by objective testing.
Complications
- Erosive esophagitis — mucosal breaks visible on endoscopy; graded by Los Angeles classification (A–D)
- Peptic stricture — from chronic acid exposure causing fibrosis; presents as progressive dysphagia
- Barrett esophagus — intestinal metaplasia of the esophageal mucosa (specialized columnar epithelium replacing squamous); a precancerous condition
- Esophageal adenocarcinoma — risk rises with BMI; relative risk 2.27–11.3× in obese patients vs. normal weight
Diagnosis
Empirical PPI trial is the initial approach for typical symptoms (heartburn/regurgitation) without alarm features.
Upper endoscopy (EGD) is indicated for:
- Alarm symptoms: dysphagia, odynophagia, weight loss, GI bleeding, anemia
- Failure of PPI therapy
- Screening for Barrett esophagus in high-risk patients (chronic GERD >5 years + risk factors)
Ambulatory pH or pH-impedance monitoring:
- Gold standard for documenting abnormal esophageal acid exposure
- Useful when diagnosis is uncertain or symptoms persist despite PPI
Esophageal manometry: evaluates LES pressure and peristaltic function; required before anti-reflux surgery.
Management
Lifestyle modifications
- Weight loss (most evidence-based lifestyle intervention)
- Elevate head of bed
- Avoid trigger foods (fatty/spicy foods, chocolate, caffeine, alcohol, mint)
- Avoid meals within 2–3 hours of recumbency
- Smoking cessation
Pharmacologic therapy
| Drug class | Role |
|---|---|
| Proton pump inhibitors (PPIs) | First-line; most effective acid suppression (omeprazole, lansoprazole, esomeprazole, etc.) |
| H₂ receptor antagonists (H₂RAs) | Second-line or as-needed; less potent than PPIs |
| Antacids | Symptomatic relief for mild/infrequent symptoms |
| Alginates | Form a raft over gastric contents; useful for postprandial reflux |
| Baclofen | GABA-B agonist; reduces tLESRs; used in refractory cases |
PPIs are taken 30–60 minutes before a meal for maximal efficacy.
Surgical / endoscopic therapy
- Laparoscopic Nissen fundoplication — wrap of gastric fundus around the LES; indicated for patients intolerant of or non-responsive to antisecretory therapy (especially those with documented reflux and predominant regurgitation)
- LINX device — magnetic sphincter augmentation
- Endoscopic therapies (e.g., transoral incisionless fundoplication [TIF]) for selected patients
Barrett Esophagus & Surveillance
Barrett esophagus carries a ~0.5%/year risk of progression to adenocarcinoma. Surveillance endoscopy intervals depend on degree of dysplasia:
- No dysplasia: every 3–5 years
- Low-grade dysplasia: every 6–12 months or endoscopic eradication therapy
- High-grade dysplasia: endoscopic eradication therapy (endoscopic mucosal resection + radiofrequency ablation)
— Goldman-Cecil Medicine, pp. 1429–1431 | Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.