Which bp medicine given in which condition
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a thorough, evidence-based guide to antihypertensive drug selection by condition, drawn from Harrison's Principles of Internal Medicine (22nd Ed., 2025) and Fuster & Hurst's The Heart (15th Ed.).
Antihypertensive Drugs: Which Drug for Which Condition
Treatment Flowchart (Uncomplicated Hypertension)
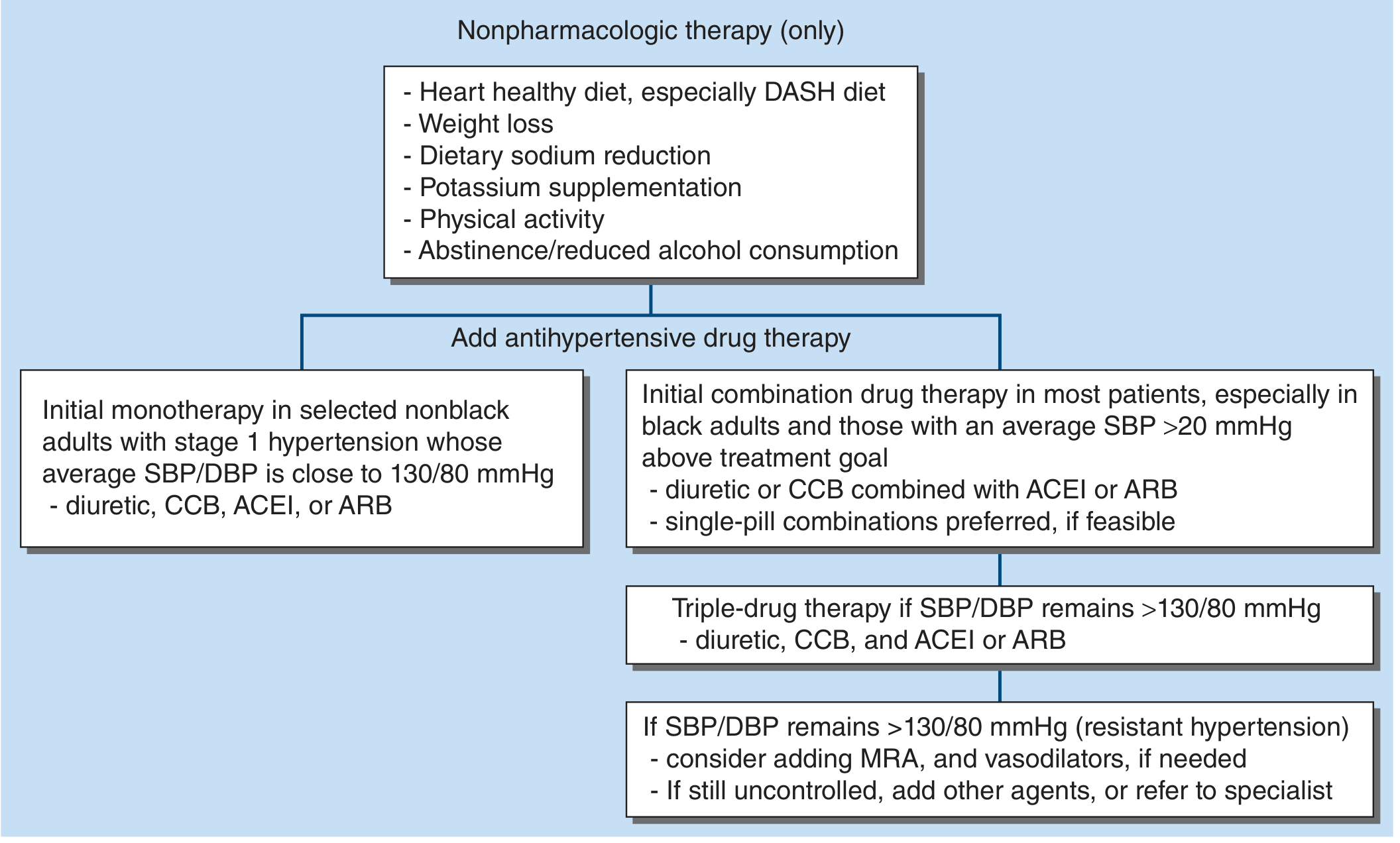
1. Uncomplicated / Primary Hypertension
Four first-line drug classes are equally acceptable when there is no specific compelling indication:
| Drug Class | Examples | Key Notes |
|---|---|---|
| Thiazide/Thiazide-like diuretics | Chlorthalidone, HCTZ, Indapamide | Meta-analyses show "best in class" for CVD prevention; chlorthalidone preferred (longer half-life) |
| ACE Inhibitors (ACEi) | Ramipril, Lisinopril, Enalapril | Avoid in pregnancy; do not combine with ARB |
| Angiotensin Receptor Blockers (ARB) | Losartan, Valsartan, Candesartan | Use when ACEi causes cough; avoid in pregnancy |
| Calcium Channel Blockers (CCB-DHP) | Amlodipine, Felodipine, Nifedipine LA | Best for stroke prevention; good in elderly |
Beta-blockers are no longer recommended as first-line for uncomplicated HTN - head-to-head trials show inferior CVD protection, especially for stroke prevention compared to the four classes above.
Combination strategy:
- Dual therapy: Diuretic OR CCB + ACEi or ARB
- Triple therapy: Diuretic + CCB + ACEi or ARB
- Resistant HTN: Add mineralocorticoid receptor antagonist (MRA) like spironolactone, alpha-blocker, or vasodilator
2. Condition-Specific Drug Choices (Compelling Indications)
Heart Failure (HFrEF)
- ACEi or ARB - cornerstone; reduces mortality
- Beta-blockers (carvedilol, metoprolol succinate, bisoprolol) - proven mortality benefit
- MRA (spironolactone, eplerenone) - reduces mortality and hospitalizations
- SGLT2 inhibitors - especially if diabetes coexists (empagliflozin, dapagliflozin)
- Loop diuretics (furosemide) - for volume overload/congestion
- Non-DHP CCBs (diltiazem, verapamil) are CONTRAINDICATED in HFrEF
Post-Myocardial Infarction (Post-MI)
- Beta-blockers - first-line (metoprolol, carvedilol); reduce reinfarction and mortality
- ACEi or ARB - especially if EF is reduced
- MRA - if EF reduced and no significant renal impairment or hyperkalemia
- Avoid non-DHP CCBs if LV dysfunction is present
Angina / Ischemic Heart Disease
- Beta-blockers - first choice for stable angina (anti-ischemic)
- CCB (both DHP and non-DHP) - alternative or add-on for angina
- ACEi - reduce cardiovascular events in established IHD
- Long-acting nitrates - add-on for symptom control
Chronic Kidney Disease (CKD) / Proteinuria
- ACEi or ARB - primary agents; reduce intraglomerular pressure via efferent arteriolar dilation, slow proteinuria progression. Especially important with proteinuria and advanced CKD
- Diuretics - loop diuretics (furosemide) when eGFR <30 mL/min/1.73m² (thiazides less effective at low eGFR; however, chlorthalidone showed benefit even in stage 4 CKD in a recent RCT)
- CCBs - safe add-on but dilate afferent arteriole; use in combination with ACEi/ARB
- Monitor potassium carefully with ACEi/ARB + CKD
Diabetes Mellitus
- ACEi or ARB - preferred (renal protection, reduce microalbuminuria)
- SGLT2 inhibitors - now strongly recommended for cardio-renal protection beyond BP lowering
- CCBs - good add-on; metabolically neutral
- Thiazides - use with caution (slight dyslipidemia and dysglycemia risk, but still effective)
- Beta-blockers - can mask hypoglycemia symptoms; use if other indications (e.g., post-MI, HF)
Stroke Prevention / Cerebrovascular Disease
- CCBs - particularly effective for stroke prevention (superior to beta-blockers)
- ACEi or ARB - reduce recurrent stroke risk
- Thiazide diuretics - also effective for stroke prevention
- Target: SBP/DBP <130/80 mmHg
Isolated Systolic Hypertension (Elderly)
- Thiazide diuretics or CCBs - first choice; proven in large trials
- Start with lower doses; titrate gradually
- ACEi or ARB - also appropriate
Black / African-American Patients
- Thiazide diuretics + CCBs preferred (ACEi/ARBs less effective as monotherapy in this population)
- Combination therapy is usually needed
- ACEi/ARBs have higher rates of angioedema in Black patients
Hypertension in Pregnancy
- Labetalol (oral) - first-line
- Methyldopa - safe, traditional choice
- Nifedipine (oral) - alternative
- ACEi, ARBs, direct renin inhibitors are CONTRAINDICATED (teratogenic)
Hypertensive Emergency (IV Agents)
- Labetalol IV - versatile; safe in most emergencies
- Nicardipine IV - good for most hypertensive emergencies, including peri-operative
- Sodium nitroprusside IV - severe/refractory emergencies (watch for cyanide toxicity)
- Hydralazine IV - used in pregnancy-related emergencies
- Esmolol IV - aortic dissection, hypertensive crises with tachycardia
Pheochromocytoma
- Alpha-blockers first (phenoxybenzamine or doxazosin) - always before beta-blockers
- Beta-blockers added AFTER alpha-blockade - to control tachycardia (never give beta-blocker alone - can cause paradoxical hypertension)
Primary Aldosteronism (Conn's Syndrome)
- Spironolactone or eplerenone (MRAs) - first-line
- Also effective: amiloride
Benign Prostatic Hypertrophy (BPH) + HTN
- Alpha-1 blockers (doxazosin, terazosin) - treat both BPH and HTN simultaneously
Aortic Dissection
- Beta-blockers IV (labetalol, esmolol) - reduce HR and BP
- Sodium nitroprusside or nicardipine - if BP not controlled, always WITH beta-blockade
3. Quick Reference Summary Table
| Condition | Preferred Drug(s) | Avoid |
|---|---|---|
| Uncomplicated HTN | Thiazide, CCB, ACEi, ARB | Beta-blockers (1st line) |
| Heart failure (HFrEF) | ACEi/ARB + Beta-blocker + MRA | Non-DHP CCB |
| Post-MI | Beta-blocker + ACEi/ARB | - |
| Angina | Beta-blocker, CCB | - |
| CKD / Proteinuria | ACEi or ARB | NSAIDs |
| Diabetes | ACEi or ARB, SGLT2i | Beta-blockers (relative) |
| Stroke prevention | CCB, ACEi/ARB, Thiazide | - |
| Elderly / isolated SBP | Thiazide or CCB | - |
| Black patients | Thiazide + CCB | ACEi/ARB monotherapy |
| Pregnancy | Labetalol, Methyldopa, Nifedipine | ACEi, ARB |
| Pheochromocytoma | Alpha-blocker first, then Beta | Beta-blocker alone |
| Primary aldosteronism | Spironolactone / Eplerenone | - |
| BPH + HTN | Alpha-blocker (doxazosin) | - |
| Hypertensive emergency | IV Labetalol, Nicardipine, Nitroprusside | Oral agents alone |
Sources: Harrison's Principles of Internal Medicine 22E (2025), p. 2187-2190; Fuster & Hurst's The Heart 15th Ed., p. 249-250
This is a shared conversation. Sign in to Orris to start your own chat.