Hepatomegaly congestion
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Searching Images
congestive hepatomegaly nutmeg liver pathology
Loading Image
Loading Image
Here is a comprehensive overview of hepatomegaly due to congestion (congestive hepatopathy).
Congestive Hepatomegaly
Pathophysiology
Right-sided heart failure transmits increased central venous pressure directly to the hepatic sinusoids via the hepatic veins and inferior vena cava. This produces:
- Decreased hepatic blood flow and arterial oxygen saturation
- Increased hepatic vein pressure → sinusoidal hypertension and edema
- Centrilobular congestion and necrosis — zone 3 (centrilobular zone) is most vulnerable because it is farthest from the portal blood supply
- Superimposed ischemic hepatitis is common when cardiac output drops acutely
With chronic, sustained congestion, progressive centrilobular fibrosis develops. The mechanical force of sinusoidal dilatation and intravascular stasis/thrombosis are the primary drivers of fibrosis. — Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Gross Pathology — "Nutmeg Liver"
The liver is enlarged and heavy (congestive hepatomegaly). On cut section:
- Congested, dark-red centrilobular areas surrounded by pale, non-congested peripheral parenchyma → the classic nutmeg liver appearance
- When left-sided failure coexists, severe central hypoxia produces centrilobular necrosis on top of sinusoidal congestion
- With long-standing severe right-sided failure → cardiac cirrhosis (centrilobular fibrosis becomes bridging fibrosis between central veins — "reverse lobulation")
Gross specimen — nutmeg liver (chronic passive congestion):

— Robbins & Kumar Basic Pathology
Histopathology
- Sinusoidal distention and hepatocyte atrophy in centrilobular zones
- Centrilobular necrosis (correlates with recent hypotension episodes)
- Centrilobular fibrosis progressing to bridging fibrosis between central veins (reverse lobulation) → cardiac cirrhosis
- No significant inflammatory infiltrate — "bland" cirrhosis
Histology — cardiac cirrhosis (Masson trichrome stain):
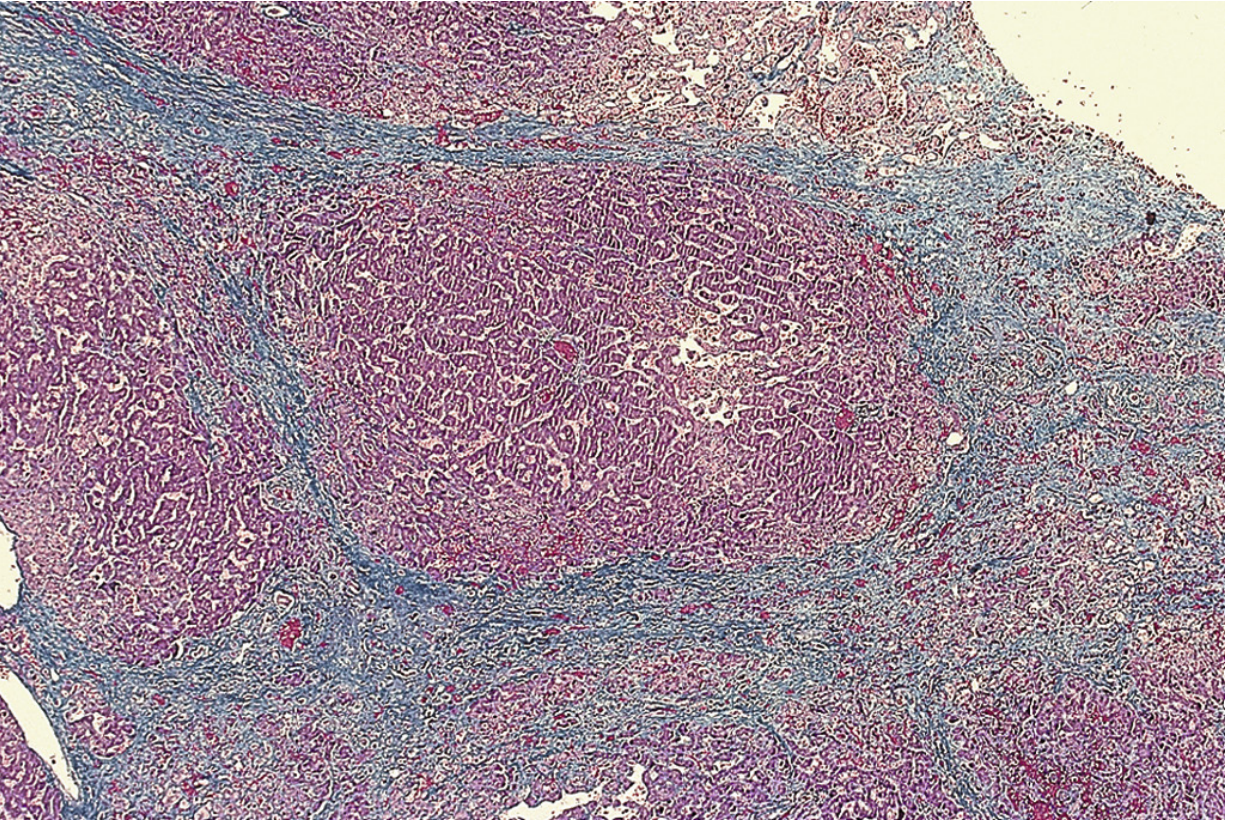
Low-power view showing a portal tract at the center of a regenerative nodule, with fibrotic bands bridging central veins. Sinusoids are dilated and congested. No inflammatory cells. (Masson trichrome) — Sleisenger and Fordtran's Gastrointestinal and Liver Disease, Fig. 85.10
Associated Findings of Right-Sided Heart Failure
| Structure | Consequence |
|---|---|
| Liver | Congestive hepatomegaly, nutmeg liver, cardiac cirrhosis |
| Portal vein | Portal hypertension → congestive splenomegaly |
| Peritoneal cavity | Ascites (high SAAG, high protein) |
| Pleural/pericardial spaces | Transudative effusions |
| Bowel wall | Edema → impaired nutrient/drug absorption |
| Subcutaneous tissue | Dependent pitting edema (feet, lower legs; presacral if bedridden) |
— Robbins & Kumar Basic Pathology
Clinical Features
- Dull RUQ pain with hepatomegaly
- Pulsatile liver if tricuspid regurgitation is present
- Hepatojugular reflux — JVP rises on liver compression
- Ascites with high SAAG and high protein (distinguishes from cirrhosis)
- Mild hyperbilirubinemia (bilirubin usually <3 mg/dL); jaundice in <10%, only in severe/acute failure
- PT prolonged in >75% of cases (vitamin K resistant)
- Aminotransferases mildly elevated; if acute drop in cardiac output occurs → extreme AST/ALT elevation (>3000 U/L) = ischemic hepatitis
- Spider telangiectasias and varices are typically absent; variceal bleeding from congestive hepatopathy alone does not occur
Imaging (CT/US)
- Hepatomegaly
- Dilatation of the IVC and hepatic veins
- Ascites
- Heterogeneous ("nutmeg") hepatic enhancement on contrast CT during portal phase
Treatment
Treatment is directed at the underlying cardiac disease (improve cardiac output, systemic oxygenation). Congestive hepatopathy itself does not worsen prognosis — mortality is determined by severity of cardiac disease. Paracentesis may be needed for tense ascites. — Sleisenger and Fordtran's Gastrointestinal and Liver Disease
Key Causes to Remember:
- Congestive heart failure (most common — especially right-sided)
- Constrictive pericarditis
- Tricuspid stenosis/regurgitation
- Budd-Chiari syndrome
- IVC obstruction
This is a shared conversation. Sign in to Orris to start your own chat.