Arsenic poisoning short note
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have all the information needed. Here is the comprehensive short note on arsenic poisoning:
Arsenic Poisoning
Introduction
Arsenic is a metalloid poison obtained from compounds such as arsenic trioxide (As₂O₃), copper arsenite (Paris green), calcium/lead arsenate (pesticides), and arsine gas (AsH₃). It is implicated in accidental, suicidal, and homicidal poisoning. Arsenic occurs in three oxidation states: elemental, trivalent (arsenite), and pentavalent (arsenate) - trivalent forms are the most toxic.
Fatal dose: 180-300 mg of arsenic trioxide
Fatal period: 12-48 hours (may be fatal within 2-3 hours in fulminant cases)
Mechanism of Toxicity
Arsenic exerts its toxic effects through multiple mechanisms:
- SH-group binding: Combines reversibly with sulphydryl (-SH) groups of tissue proteins and enzymes, inhibiting cellular metabolism
- Enzyme inhibition: Disrupts key enzyme systems (pyruvate dehydrogenase, lipoic acid)
- Capillary poison: Dilates and damages capillaries, causing transudation of fluid
- Organ-specific: Fatty degeneration of the liver, renal tubular necrosis, and axonal neuropathy (disintegration of the axis cylinder with myelin fragmentation)
Acute Arsenic Poisoning
Routes of exposure
Oral ingestion (most common), inhalation (arsine gas), skin absorption, rectal/vaginal introduction.
Signs and Symptoms
Onset is typically within 30 minutes of ingestion:
- Metallic/garlicky taste, xerostomia (dry mouth), dysphagia
- Severe nausea and vomiting - projectile, dark brown/yellow, containing mucus, blood and bile
- Profuse diarrhoea - initially dark and bloody, later colourless, odourless, rice-water stools (resembling cholera)
- Abdominal pain - burning, colicky, worsened by pressure; tenesmus and anal irritation
- Cardiovascular: tachycardia, hypotension, cold clammy skin, pallor - due to hypovolaemia and direct myocardial toxicity; ECG shows T-wave inversion and prolonged QT interval
- Dehydration: sunken eyes, shrunken face, cramps in calf muscles
- CNS: restlessness, hypoxia, convulsions and coma preceding death
- Death is usually due to irreversible circulatory insufficiency
Secondary effects (2-4 weeks post-exposure if not fatal):
- Hair loss (alopecia)
- Mee's lines (Aldrich-Mees lines) - white transverse lines on nail plate
- Sensorimotor peripheral neuropathy
- Skin changes resembling chronic poisoning
- Possible chronic renal failure
Chronic Arsenic Poisoning
Arises from repeated small doses - occupational exposure (orchardists, pesticide workers, semiconductor manufacturing), contaminated drinking water, or homicidal administration.
Skin (most characteristic features):
- Earliest sign: persistent erythematous flushing (capillary dilation)
- Raindrop pigmentation - finely mottled brown spots on skin flexures, temples, eyelids, neck

Raindrop pigmentation of palms in chronic arsenic poisoning

Raindrop pigmentation of soles in chronic arsenic poisoning
- Hyperkeratosis of palms and soles
- Mee's lines - transverse white streaks 1-2 mm wide on fingernails (appear ~5 weeks post-exposure; double lines if more than one exposure)
- Patchy/diffuse alopecia, brittle nails
- Bowen's disease (intraepidermal carcinoma) - a long-term complication indicating systemic neoplastic processes
Nervous system:
- Neuropathy is the hallmark - symmetrical sensorimotor polyneuropathy resembling Guillain-Barré syndrome
- Paresthesia, numbness, pain especially on soles of feet
- "Glove and stocking" distribution of sensory loss
- Distal weakness - wrist drop, inability to walk; muscle atrophy; ataxia
- Encephalopathy (severe headache, personality changes, convulsions, coma)
Other systems:
| System | Features |
|---|---|
| GI | Nausea, vomiting, diarrhoea, salivation, abdominal cramps |
| Eyes | Congestion, lacrimation, photophobia |
| CVS/Renal | Chronic nephritis, cardiac failure, dependent oedema |
| Hepatic | Hepatomegaly, jaundice, cirrhosis |
| Haematologic | Normochromic normocytic anaemia, leukopenia, thrombocytopenia, mild eosinophilia, karyorrhexis on bone marrow; can cause leukaemia |
| General | Weight loss, hair loss, brittle nails |
| Carcinogenic | Lung cancer, skin cancer, leukaemia (teratogenic as well) |
Arsine Gas Poisoning (AsH₃)
- Occurs in industrial settings (acid/water acting on arsenic-bearing metals)
- Acts as a direct haemolytic poison
- Features: cough, frothy sputum, pulmonary oedema, cyanosis, corneal ulcer, conjunctivitis, haemolysis, haemoglobinuria, renal failure
- Death can be almost instantaneous
- BAL is NOT effective for arsine gas poisoning
Diagnosis
- Blood arsenic: >1.5 mg/100 mL indicates serious poisoning (normal <4 mg/L)
- Urine arsenic: normal <0.03 mg/L; chelation can be stopped when 24-hr urine falls below 50 mg
- Hair and nails: analysed by ion emission spectroscopy / atomic absorption spectroscopy / neutron activation analysis - most useful for chronic poisoning (arsenic has predilection for keratin)
- Colorimetry, polarography for tissue levels
- X-ray abdomen: may show radio-opaque arsenic in GI tract
- Definitive diagnosis is difficult due to natural trace arsenic in the body and multi-systemic presentation
Differential Diagnosis: Arsenic Poisoning vs. Cholera
| Feature | Arsenic Poisoning | Cholera |
|---|---|---|
| Pain in throat | Before vomiting | After vomiting |
| Purging | After vomiting | Before vomiting |
| Stools | Initially dark/bloody, later rice-water | Rice-water from onset, not bloody |
| Tenesmus/anal irritation | Present | Absent |
| Vomit | Contains mucus, bile, blood | Watery, no mucus/bile/blood |
| Voice | Not affected | Rough/whistling |
| Conjunctivae | Inflamed | Not inflamed |
| Analysis | Arsenic present | Cholera vibrio present |
Treatment
Acute Poisoning:
- Gastric lavage with large amounts of warm water/milk; repeated at intervals (arsenic is re-secreted into GI tract)
- Whole bowel irrigation; nasogastric suction
- BAL (British Anti-Lewisite / Dimercaprol): 2.5-3 mg/kg IM - given 4-hourly for 2 days, 6-hourly for 1 day, then 12-hourly; total duration depends on clinical response and urine arsenic levels
- Stop BAL when 24-hr urine arsenic falls below 50 mg
- Stop if side effects: nausea, tachycardia, hypotension, burning mouth
- DMSA (Succimer) or DMPS: superior to BAL if available; can be used as alternative
- Oral D-Penicillamine: 100 mg/kg/day in 4 divided doses for 4-8 days, after initial 12-48 hours of BAL
- IV saline for dehydration; morphine for pain relief; castor oil/MgSO₄ to reduce intestinal absorption
- Greasy substances (butter, ghee) help prevent arsenic absorption; alkalis should not be given (increase arsenic solubility)
- Demulcents: ghee, barley water
Arsine Gas:
- Remove to fresh air; oxygen inhalation; exchange transfusion; haemodialysis; alkaline drinks
- BAL is ineffective
Chronic Poisoning:
- Remove from source of exposure
- BAL administration
Autopsy Findings
- Prolonged rigor mortis; generalised dehydration; shrunken eyeballs; cyanosis of hands and feet; jaundice
- Stomach: inflamed mucosa with "red velvet appearance" - lines of redness running along folds
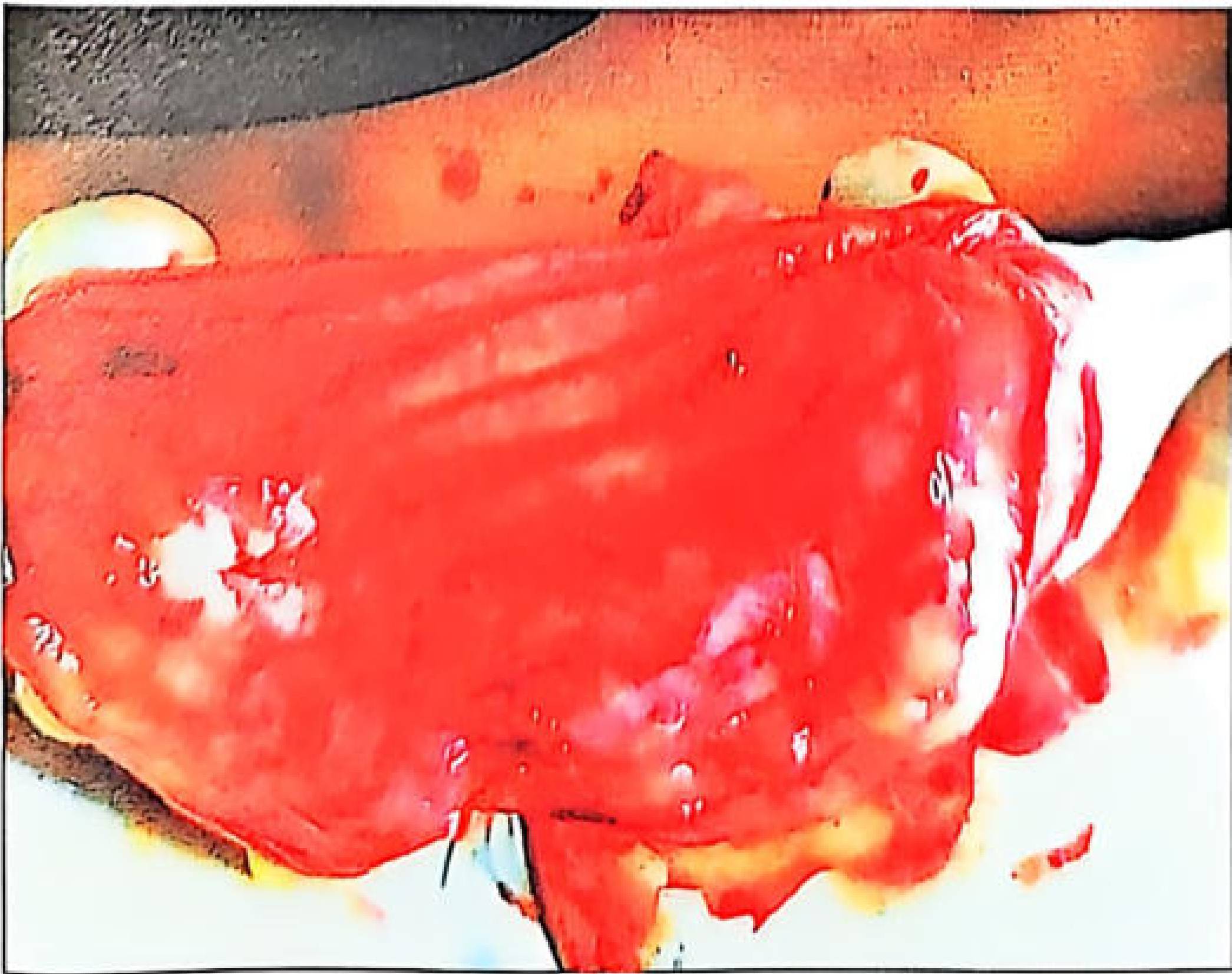
Gastric mucosa showing red velvet appearance with lines of redness - a characteristic autopsy finding
- Mucosal vesicle formation and sloughing in small intestine; chocolate/brown discolouration of intestinal contents
- Subendocardial petechial haemorrhages of the ventricle - pathognomonic finding (also seen in phosphorus, barium, mercury poisoning and heat stroke)
- Liver, spleen, kidneys: congested, enlarged, cloudy swelling, fatty change; kidneys show acute tubular necrosis
- Lungs: congested with subpleural ecchymoses
- Brain: oedema with patchy necrosis or haemorrhagic encephalitis; congested meninges
- Arsenic values in liver and blood >1 mg% in acute arsenic poisoning death
Sources: P C Dikshit Textbook of Forensic Medicine and Toxicology; The Essentials of Forensic Medicine and Toxicology 36th edition (2026); Katzung's Basic and Clinical Pharmacology, 16th ed; Henry's Clinical Diagnosis and Management by Laboratory Methods
This is a shared conversation. Sign in to Orris to start your own chat.