Posterior Lumbar Interbody Fusion (PLIF)
Reading File
Finding Sources
Searching Images
posterior lumbar interbody fusion PLIF surgical technique
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Posterior Lumbar Interbody Fusion (PLIF) drawn from authoritative medical textbooks.
Posterior Lumbar Interbody Fusion (PLIF)
Definition & Concept
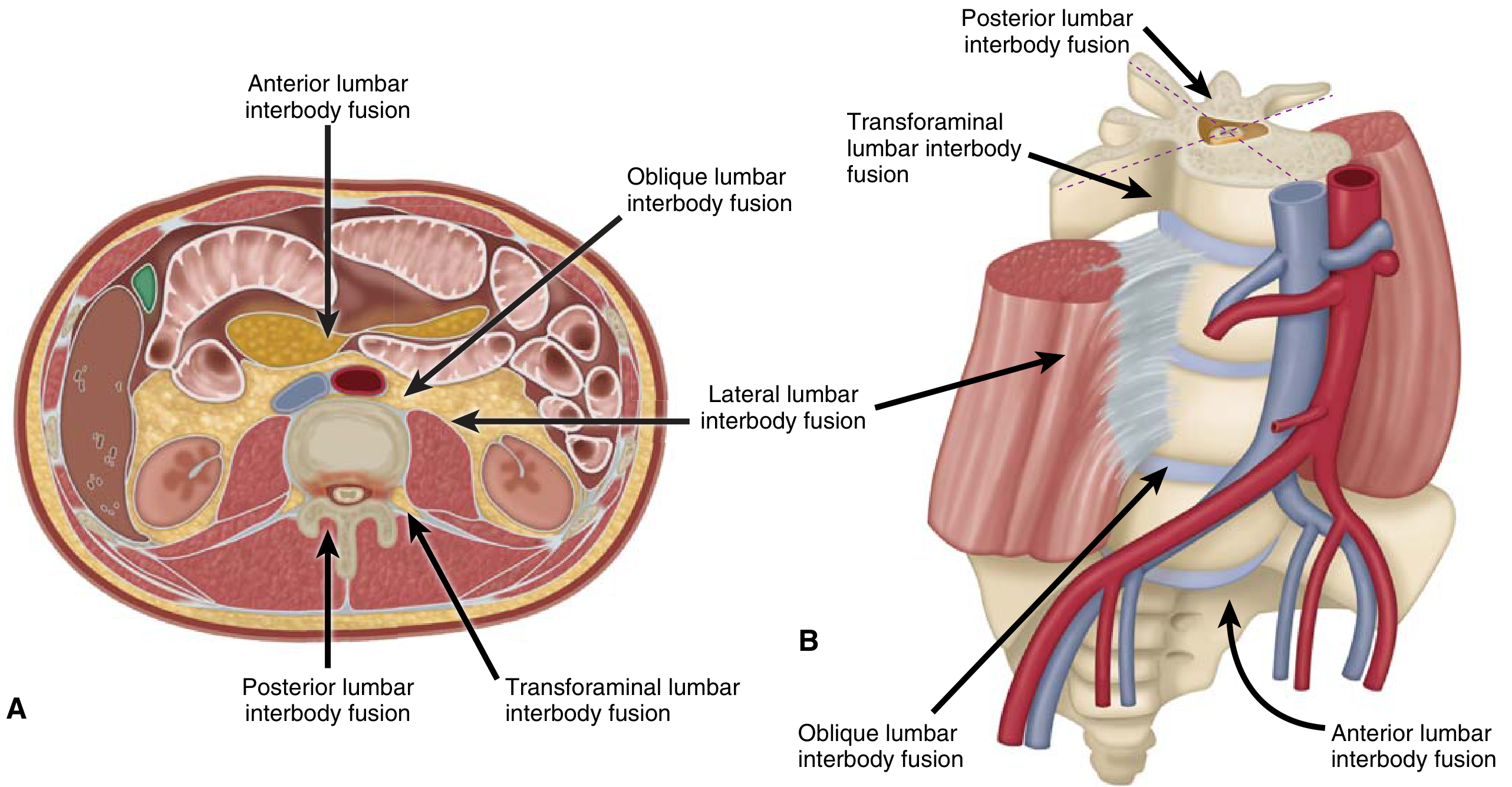
PLIF is a spinal fusion technique in which the intervertebral disc space is accessed and fused via a posterior midline approach. It achieves 360° stabilization of the lumbar spine through a single posterior corridor — combining neural decompression with anterior column support.
The diagram below shows how PLIF compares to other lumbar interbody fusion approaches by corridor:
Indications
PLIF is primarily indicated for conditions causing lumbar instability or refractory mechanical/discogenic pain:
- Degenerative disc disease (DDD) — after conservative measures are exhausted
- Spondylolisthesis (segmental or iatrogenic lumbar instability)
- Lumbar herniated disc with instability
- Spinal stenosis requiring decompression + stabilization
- Failed conservative management of low back pain
"Posterior lumbar fusion is used for treatment of low-back pain associated with segmental or iatrogenic lumbar instability and spondylolisthesis." — Miller's Anesthesia, 10th Ed.
Surgical Technique
Approach
- Posterior midline incision with the patient prone
- Paraspinal muscles are retracted bilaterally to expose the posterior elements
- Laminectomy or laminotomy is performed to access the spinal canal
- The ligamentum flavum and part of the facet joints are removed
Decompression
- The meningeal sac and nerve roots are gently retracted medially
- This exposes the disc space bilaterally
- The offending disc material is excised (discectomy)
Interbody Fusion
- The disc space is prepared (endplate decortication)
- Structural grafts or cages are inserted into the intervertebral space:
- Femoral ring allografts
- Interbody fusion cages — titanium, tantalum, PEEK (polyether ether ketone), carbon composite polymers, or bioabsorbable PLA
- Cages are packed with autologous cancellous bone, allograft, or synthetic bone substitute (BMP, demineralized bone matrix, ceramics)
- Cages provide immediate load-bearing capacity while biological fusion occurs
Posterior Fixation
- Pedicle screws and rods are placed bilaterally to stabilize the construct
- Supplementary fixation options: translaminar screws, transfacet screws
"Such implants provide immediate load-bearing capacity while fusion occurs in their core packed with autologous cancellous bone, allograft or synthetic bone substitute." — Grainger & Allison's Diagnostic Radiology
PLIF vs. Related Techniques
| Technique | Approach | Key Difference |
|---|---|---|
| PLIF | Posterior midline | Bilateral nerve root retraction; direct central access |
| TLIF | Posterior transforaminal | Unilateral approach through the foramen; less neural retraction |
| ALIF | Anterior retroperitoneal | No posterior neural exposure; larger cage possible |
| LLIF/OLIF | Lateral/oblique | Retroperitoneal lateral corridor; avoids posterior muscles |
PLIF and TLIF are both performed through a posterior incision, but TLIF accesses the disc obliquely through the foramen (unilateral), avoiding the bilateral nerve retraction required in PLIF.
Graft & Implant Materials
- Autograft: Iliac crest (gold standard for osteogenesis); morselized cancellous chips
- Allograft: Femoral rings, fibular struts, bone chips
- Synthetic cages: PEEK, titanium, tantalum — radiolucent with radiopaque markers for fluoroscopic confirmation
- Bone substitutes: Recombinant BMP, demineralized bone matrix (DBX), tricalcium phosphate, hydroxyapatite, calcium sulfate
Postoperative Imaging
| Modality | Role |
|---|---|
| Plain X-ray (AP + lateral) | Routine follow-up; hardware migration, loosening, breakage; flexion-extension for pseudarthrosis |
| CT | Precise implant position, cage alignment, fusion status; minimal artifact with titanium |
| MRI | Soft tissue and neural structures; infection, hematoma, dural leak, recurrent disc herniation |
Lateral radiograph post-PLIF will show radiopaque cage markers in the intervertebral space between pedicle screw constructs. — Grainger & Allison's Diagnostic Radiology
Complications
- Neurologic injury — from nerve root retraction, cage migration into canal, or pedicle screw misplacement
- Cage migration/subsidence
- Pseudarthrosis (failed fusion)
- Adjacent segment disease (ASD) — accelerated degeneration at levels adjacent to the fusion
- Infection / wound complications
- Dural tear / CSF leak
- Intraoperative blood loss — significant; antifibrinolytics (TXA) often used
Intraoperative neurophysiologic monitoring (IONM) with SSEPs, MEPs, and triggered EMG for pedicle screw verification is used during complex fusion procedures to guard against neurologic injury.
Key Points Summary
- PLIF achieves 360° fusion from a single posterior approach
- Requires bilateral facetectomy and nerve root retraction — higher neural manipulation than TLIF
- Provides simultaneous decompression and stabilization
- Fusion constructs combine an interbody cage/graft (anterior column) with pedicle screw-rod fixation (posterior column)
- Surgery is considered after failure of conservative treatment; outcomes for isolated discogenic pain are inconsistent
Sources: Miller's Review of Orthopaedics 9th Ed. | Miller's Anesthesia 10th Ed. | Grainger & Allison's Diagnostic Radiology | Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.