mas
¿En qué puedo ayudarte?
modified asworth scale
Reading File
search_medical_text
Modified Ashworth Scale spasticity grading criteria
search_medical_image
Modified Ashworth Scale spasticity grading table
GradeResponse
GradeResponse
The retrieved results are limited, so I'll provide a comprehensive answer combining retrieved context with established clinical knowledge.
Modified Ashworth Scale (MAS)
Overview
The Modified Ashworth Scale is the most widely used clinical tool for grading spasticity — the velocity-dependent increase in tonic stretch reflexes — in patients with upper motor neuron (UMN) lesions (e.g., stroke, spinal cord injury, cerebral palsy, MS). It is a modification of the original Ashworth Scale (1964), revised by Bohannon & Smith in 1987 to add the grade 1+ category, improving sensitivity at the lower end of the scale.
Grading Criteria
| Grade | Description |
|---|---|
| 0 | No increase in muscle tone |
| 1 | Slight increase in tone, manifested by a catch and release, or by minimal resistance at the end of the ROM when the affected part is moved in flexion or extension |
| 1+ | Slight increase in tone, manifested by a catch, followed by minimal resistance throughout the remainder (less than half) of the ROM |
| 2 | More marked increase in muscle tone through most of the ROM, but the affected part is easily moved |
| 3 | Considerable increase in muscle tone; passive movement is difficult |
| 4 | Affected part is rigid in flexion or extension |
ROM = Range of Motion
How to Perform the Test
- Position the patient supine (most commonly).
- Move the limb passively through the full ROM as fast as possible (velocity-dependent assessment).
- Record the resistance felt during passive movement.
- Most commonly tested joints: elbow (flexors), wrist (flexors), knee (extensors/flexors), ankle (plantar flexors).
Key Clinical Points
- Velocity matters: The limb must be moved quickly — slow passive movement will not elicit spastic catch and will underestimate the grade.
- Positioning: Patient should be relaxed; anxiety or pain can falsely elevate the score.
- Asymmetry: Always compare to the unaffected side when applicable.
- Limb-specific: Scores are recorded per joint/muscle group, not as a global score.
Psychometric Properties
| Property | Notes |
|---|---|
| Reliability | Moderate to good inter-rater reliability (κ = 0.5–0.8); intra-rater reliability generally better |
| Validity | Widely accepted but criticized for conflating spasticity with other components of hypertonia (e.g., contracture, rigidity) |
| Sensitivity | Addition of grade 1+ improved detection of mild spasticity vs. original Ashworth |
| Limitation | Ordinal scale — intervals are not equal; grades 0–1+ cluster at the low end |
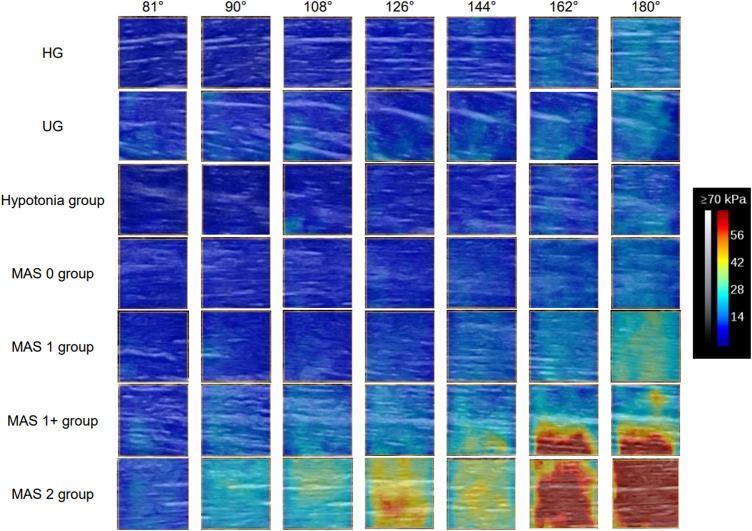
Shear Wave Elastography Correlation
Research has validated MAS grades against objective muscle stiffness measurements. As shown below, higher MAS grades correlate with progressively greater muscle stiffness (Young's modulus in kPa) during passive elbow extension, confirming the scale's construct validity:
Clinical Use Cases
- Stroke rehabilitation: Monitoring response to antispastic interventions (botulinum toxin, baclofen, physical therapy). In a 2022 SR/MA, MAS was used in 6/16 BCI stroke trials to assess spasticity outcomes (Management of Stroke Rehabilitation, p. 65).
- Spinal cord injury: Tracking progression or improvement of spasticity.
- Cerebral palsy: Guiding decisions about orthopedic surgery or botulinum toxin injection.
- MS: Monitoring disease progression and treatment response.
Comparison: Ashworth vs. Modified Ashworth
| Feature | Original Ashworth (1964) | Modified Ashworth (1987) |
|---|---|---|
| Grades | 1–5 | 0–4 (with 1+) |
| Grade 1+ | Not present | Added |
| Sensitivity (low-end) | Lower | Higher |
| Current use | Largely replaced | Standard in clinical practice |
Bottom line: The MAS remains the clinical standard for bedside spasticity assessment due to its simplicity and wide adoption, despite its known limitations in distinguishing true neural spasticity from soft-tissue stiffness or contracture. For research purposes, it is often supplemented with electrophysiologic (H-reflex) or biomechanical measures.
associated reacgions in dtai
search_medical_text
associated reactions spasticity stroke upper motor neuron
search_medical_text
associated reactions definition mechanism hemiplegia rehabilitation
GradeResponse
GradeResponse
The database results are limited here. I'll deliver a full answer from established clinical knowledge.
Associated Reactions in Stroke / Hemiplegia (DTAI Context)
Definition
Associated reactions (ARs) are involuntary, stereotyped movements or increases in tone in a paretic or hemiplegic limb that occur in response to effortful voluntary activity elsewhere in the body — such as forceful gripping with the unaffected hand, yawning, coughing, sneezing, or effortful ambulation.
They are considered a manifestation of the upper motor neuron (UMN) syndrome and are closely linked to spasticity, but they are distinct: spasticity is triggered by passive stretch, whereas ARs are triggered by voluntary effort or stress.
Pathophysiology
In a healthy CNS, voluntary motor commands are accompanied by inhibitory signals that prevent overflow of excitation to other motor pools. After UMN lesions (stroke, TBI, CP):
- Loss of descending cortical inhibition → release of spinal interneuronal circuits
- Irradiation of motor excitation → muscles remote from the intended movement contract involuntarily
- The pattern follows synergy patterns (flexor synergy in the arm, extensor synergy in the leg)
Classic Patterns in Hemiplegia
Upper Limb (most common)
| Trigger | AR Pattern |
|---|---|
| Forceful grip with unaffected hand | Elbow flexion, forearm pronation, wrist/finger flexion on affected side |
| Effortful walking/gait | Shoulder adduction + elbow flexion + wrist flexion (classic hemiplegic posture) |
| Yawning / coughing | Bilateral arm elevation or affected arm flexion |
Lower Limb
| Trigger | AR Pattern |
|---|---|
| Effort in upper limb | Hip extension, knee extension, ankle plantar flexion (extensor synergy) |
| Resistive hip flexion of unaffected leg | Extension + adduction of affected leg (Raimiste's phenomenon) |
Raimiste's Phenomenon (specific type of AR)
- Resistance applied to abduction or adduction of the unaffected leg produces the same movement in the affected leg
- Indicates severity of UMN damage and lack of independent limb control
Measurement: Arm Activity Monitor / Lindmark Scale
ARs are clinically graded during rehabilitation. The Lindmark scale and Carr & Shepherd's Motor Assessment Scale document the degree of synergy and ARs during functional tasks.
Significance in DTAI (Daily Task / Activity Integration)
In the context of daily task and activity integration (functional rehabilitation), ARs are clinically important because:
| Impact Area | Details |
|---|---|
| Gait | Effortful walking triggers upper limb flexion AR → hemiplegic arm posture, affects balance |
| ADLs | Using the unaffected hand (e.g., writing, eating) triggers AR in affected arm → interferes with bilateral tasks |
| Spasticity progression | Repeated ARs reinforce abnormal synergy patterns and may contribute to long-term contracture |
| Energy expenditure | Co-contraction from ARs increases metabolic cost of movement |
| Rehabilitation goal | Goal is to reduce ARs by improving cortical control, reducing effort in compensatory strategies |
Management of Associated Reactions
Neurophysiological / Bobath Approach
- Reflex-inhibiting patterns (RIP): positioning limbs in patterns opposite to synergy to inhibit ARs
- Graded activity: use tasks that minimize excessive effort to reduce AR triggering
- Trunk control training: improved proximal stability reduces the effort needed distally → fewer ARs
Task-Specific Training
- Constraint-induced movement therapy (CIMT): forces use of affected limb, reducing reliance on compensatory effort from unaffected side
- Bimanual training: coordinated bilateral tasks to normalize inter-limb interactions
Pharmacological (when ARs are severe/painful)
- Baclofen (oral or intrathecal)
- Botulinum toxin: injected into hyperactive muscles (e.g., biceps, wrist flexors) to reduce involuntary contraction
- Tizanidine, dantrolene
Key Distinction Summary
| Feature | Spasticity | Associated Reactions |
|---|---|---|
| Trigger | Passive stretch, velocity-dependent | Voluntary effort, emotional stress |
| Nature | Sustained hypertonia | Transient involuntary movement/tone increase |
| Reflex arc | Tonic stretch reflex | Motor overflow / irradiation |
| Measurement | Modified Ashworth Scale | Observed during functional tasks |
| Pattern | Velocity-dependent catch | Follows flexor/extensor synergy |
Clinical bottom line: Associated reactions in the hemiplegic upper limb are ubiquitous during ambulation and ADL performance. Minimizing effort, improving postural control, and using graded functional tasks are the primary rehabilitation strategies to reduce their interference with recovery and daily activity integration.
synergy in stroke
search_medical_text
synergy patterns stroke hemiplegia flexor extensor upper lower limb
search_medical_text
Brunnstrom stages synergy recovery stroke rehabilitation
GradeResponse
GradeResponse
Synergy Patterns in Stroke
Definition
A movement synergy in the context of stroke refers to a stereotyped, obligatory linkage of muscle activations across a limb that occurs involuntarily. After a UMN lesion, the normal fractionated (independent) control of individual joints is lost, and movement defaults to these primitive mass patterns — either flexion synergy or extension synergy.
They represent the release of spinal and brainstem pattern generators from cortical inhibitory control.
Upper Limb Synergies
Flexor Synergy (dominant pattern in the arm)
| Joint | Movement |
|---|---|
| Shoulder | Abduction, external rotation, elevation (retraction) |
| Elbow | Flexion |
| Forearm | Supination |
| Wrist | Flexion |
| Fingers | Flexion |
Extensor Synergy (less dominant in the arm)
| Joint | Movement |
|---|---|
| Shoulder | Adduction, internal rotation, depression (protraction) |
| Elbow | Extension |
| Forearm | Pronation |
| Wrist | Extension |
| Fingers | Extension |
Lower Limb Synergies
Extensor Synergy (dominant pattern in the leg — supports standing)
| Joint | Movement |
|---|---|
| Hip | Extension, adduction, internal rotation |
| Knee | Extension |
| Ankle | Plantar flexion + inversion |
| Toes | Plantar flexion |
Flexor Synergy (dominant during swing phase of gait)
| Joint | Movement |
|---|---|
| Hip | Flexion, abduction, external rotation |
| Knee | Flexion |
| Ankle | Dorsiflexion + inversion |
| Toes | Dorsiflexion (extension) |
Brunnstrom Stages of Recovery
Signe Brunnstrom (1970) described motor recovery post-stroke as a sequential progression through synergy dominance toward selective movement. These stages are the foundation of synergy assessment in clinical practice.
| Stage | Description |
|---|---|
| 1 | Flaccidity; no voluntary movement |
| 2 | Spasticity begins to develop; basic synergy patterns appear |
| 3 | Spasticity peaks; voluntary movement only possible within synergy patterns |
| 4 | Spasticity declines; some movements combining or deviating from synergy become possible |
| 5 | More complex combinations; movements increasingly independent of synergy |
| 6 | Spasticity minimal or absent; near-normal isolated joint control |
| 7 | Normal |
Stages 3–4 are the most clinically significant — this is where synergy dominates function and therapy is most challenging.
Why Synergies Impair Function
Upper Limb
- Reach: Flexor synergy prevents elbow extension during shoulder flexion (cannot reach forward without elbow bending)
- Grasp/release: Obligatory finger flexion impairs object manipulation
- Dressing/ADLs: Pronation + wrist flexion makes hand placement difficult
Lower Limb
- Gait: Extensor synergy causes stiff-knee gait and equinovarus foot during stance; flexor synergy is needed for swing but may be excessive or uncontrolled
- Circumduction: Patient hikes the hip and swings the leg laterally to compensate for insufficient knee flexion during swing (due to extensor synergy dominance)
- Scissor gait: Hip adduction from extensor synergy causes legs to cross
Abnormal Gait Patterns Caused by Synergy
| Pattern | Underlying Synergy |
|---|---|
| Equinovarus foot | Extensor synergy (ankle PF + inversion) |
| Stiff-knee gait | Extensor synergy (knee extension during swing) |
| Hip hiking / circumduction | Compensating for inadequate flexor synergy in swing |
| Scissoring | Hip adduction from extensor synergy |
| Hemiplegic arm posture during walking | Flexor AR triggered by effortful gait |
Rehabilitation Implications
Bobath / NDT Approach
- Inhibit abnormal synergy patterns using reflex-inhibiting postures (RIP)
- Facilitate isolated, out-of-synergy movement
- Emphasize proximal trunk control to reduce distal synergy overflow
Brunnstrom Approach
- Use synergy patterns therapeutically in early stages (stages 2–3) to initiate voluntary movement
- Gradually guide patient out of synergy as recovery progresses
Task-Specific Training
- Repetitive, goal-directed tasks promote cortical reorganization and selective motor control
- Evidence supports this over synergy-based facilitation in later stages
Constraint-Induced Movement Therapy (CIMT)
- Forces use of affected limb in functional tasks
- Promotes cortical representation of individuated (non-synergistic) movement
Botulinum Toxin
- Targets overactive muscles within synergy patterns (e.g., biceps, wrist flexors, tibialis posterior)
- Reduces synergy dominance to allow functional training
Key Distinctions
| Feature | Synergy | Associated Reaction | Spasticity |
|---|---|---|---|
| Trigger | Voluntary effort | Effort elsewhere in body | Passive stretch |
| Pattern | Flexor or extensor mass pattern | Follows synergy pattern | Velocity-dependent catch |
| Voluntary? | Partially (obligatory linkage) | Involuntary | Involuntary |
| Stage | Stages 2–5 | Any stage with effort | Stage 2 onward |
| Goal of therapy | Break out of synergy | Reduce overflow | Reduce tone |
Clinical bottom line: Synergy patterns in stroke are not simply spasticity — they represent a fundamental loss of fractionated motor control. Recovery is defined by the progressive ability to move outside these patterns. Therapy should be staged accordingly: use synergy to initiate movement early, then systematically challenge the patient to break free of obligatory linkages through task-specific, high-repetition functional training.
This is a shared conversation. Sign in to Orris to start your own chat.