P anca test significance in dermatology
Reading File
Finding Sources
Finding Sources
Searching PubMed
p-ANCA dermatology skin manifestations
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive information to provide a detailed, well-structured answer. Here it is:
P-ANCA (Perinuclear ANCA): Significance in Dermatology
What is P-ANCA?
Antineutrophil cytoplasmic antibodies (ANCAs) are autoantibodies directed against antigens in the cytoplasm of neutrophils. On indirect immunofluorescence (IIF), they produce two main patterns:
| Pattern | Target Antigen | IIF Appearance |
|---|---|---|
| c-ANCA | Proteinase 3 (PR3) | Cytoplasmic, granular |
| p-ANCA | Myeloperoxidase (MPO) | Perinuclear |
| Atypical ANCA | Neither PR3 nor MPO | Atypical |
Important: The specificity of the p-ANCA pattern alone is low. Anti-MPO antibodies confirmed by ELISA are required to make p-ANCA clinically meaningful for diagnosing vasculitis. A 2017 international consensus recommends high-quality immunoassays for PR3 and MPO without needing IIF as the initial screen.
ANCA-Associated Vasculitides (AAV) with Dermatological Relevance
The three primary ANCA-associated vasculitides (AAVs) are MPA, GPA, and EGPA. When used appropriately, ANCA testing achieves 85% sensitivity and 98% specificity for these conditions.
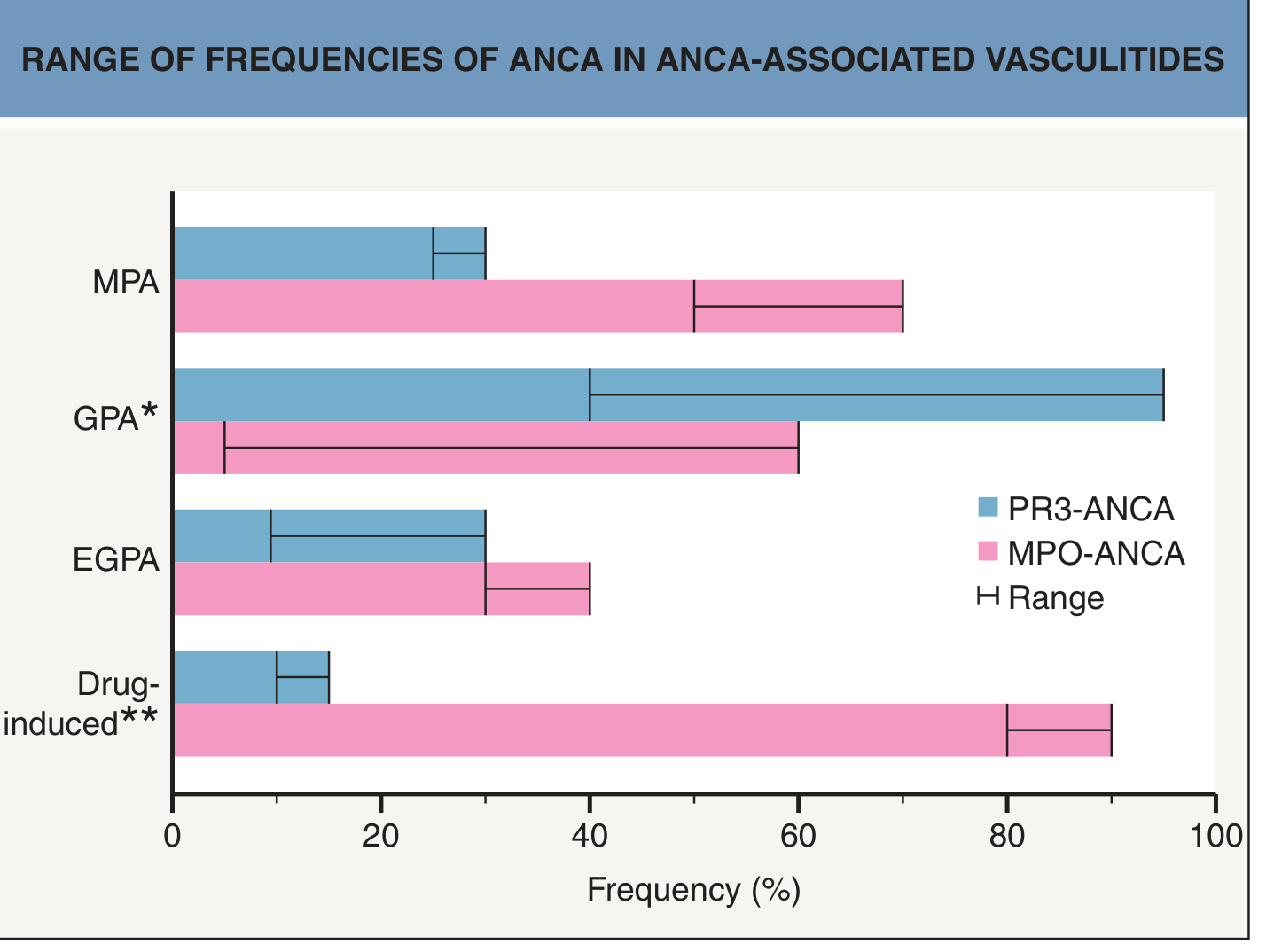
1. Microscopic Polyangiitis (MPA) — p-ANCA is the dominant pattern
- ANCA positivity: ~70% positive; p-ANCA (anti-MPO) more frequent than c-ANCA
- Skin involved in 44% — the skin may be the initial presenting feature
- Cutaneous findings:
- Purpuric papules and macules (most common)
- Livedo reticularis (in ~2/3 of those with skin-first presentation)
- Retiform purpura, cutaneous ulcers, digital ischemia
- Necrotizing leukocytoclastic vasculitis (LCV) in reticular dermis on biopsy
- Systemic: glomerulonephritis (80–90%), pulmonary capillaritis, vasculitic neuropathy (58%)
- Distinguishing feature from PAN: presence of GN, pulmonary symptoms; ANCA rarely positive in PAN
2. Granulomatosis with Polyangiitis (GPA) — c-ANCA dominant, but ~10% have p-ANCA
- ANCA positivity: ~90% in active generalized disease
- ~90% are c-ANCA (anti-PR3); the remainder are p-ANCA (anti-MPO)
- Skin involved in ~1/3 of patients at presentation; cutaneous involvement is a risk marker for severe systemic disease (GN, alveolar hemorrhage)
- Cutaneous findings:
- Purpuric papules/macules, petechiae
- Papulonecrotic lesions (especially extensor surfaces, elbows)
- Subcutaneous nodules, ulcerations resembling pyoderma gangrenosum
- "Strawberry gums" — hypertrophic gingivitis, characteristic and biopsy-accessible
- Saddle-nose deformity, nasal septal perforation (mucosal involvement)
- Livedo reticularis is rare in GPA
- Histology: LCV ± granulomatous inflammation; palisaded granulomas with multinucleated giant cells
3. Eosinophilic Granulomatosis with Polyangiitis (EGPA / Churg-Strauss)
- ANCA positivity: ~40–50%; predominantly p-ANCA (anti-MPO)
- Associated with asthma, peripheral eosinophilia (>1000 cells/μL) — helps differentiate from asthma/atopy
- Skin: purpura, papulonecrotic nodules ("Churg-Strauss nodules"), subcutaneous nodules
P-ANCA in Drug-Induced Vasculitis — Critical Dermatological Context
This is one of the most practically important applications:
- Drugs causing p-ANCA/MPO-ANCA-positive vasculitis:
- Propylthiouracil (PTU)
- Minocycline
- Hydralazine
- Allopurinol, sulfonamides, gold, thiazides, phenytoin
- Key clue: Both c-ANCA AND p-ANCA positive simultaneously → suspect drug-induced vasculitis, including levamisole-tainted cocaine
- Levamisole-adulterated cocaine (present in up to 70% of U.S. seized cocaine):
- Produces ecchymotic purpura/necrosis with predilection for ears, nose, thighs, buttocks
- Both c-ANCA and p-ANCA can be elevated
- c-ANCA reacts with human neutrophil elastase (HNE-ANCA) — patients with true GPA/MPA are HNE-ANCA negative — useful distinguishing test
- Also causes agranulocytosis (atypical for true AAV)
P-ANCA in Non-Vasculitic Dermatological Conditions
The p-ANCA pattern (without MPO specificity) can be found as a false-positive or non-specific finding in:
| Condition | Notes |
|---|---|
| Inflammatory bowel disease (IBD) | Atypical ANCA common in UC; does not indicate vasculitis |
| SLE | Can present with cutaneous vasculitis; ANCA testing part of pulmonary-renal workup |
| Rheumatoid arthritis | Low-titer, usually non-MPO specific |
| Cryoglobulinemia | Positive ANCAs can be found |
| Skin-limited vasculitis | Annual incidence of underlying AAV ~4 per million in biopsy-proven cutaneous small-vessel vasculitis (~10%) |
| Infectious diseases | TB, endocarditis, HIV |
Diagnostic Algorithm for Dermatologists
Skin vasculitis suspected
↓
Screen: IIF for ANCA pattern
↓
Positive p-ANCA pattern
↓
Confirm with ELISA: Anti-MPO antibody?
├─ YES → Strongly suggests MPA, EGPA, or drug-induced AAV
│ Assess: renal function, pulmonary symptoms, drug history
└─ NO → Atypical ANCA — consider IBD, SLE, infection
(low specificity for primary vasculitis)
Key Takeaways
- p-ANCA alone (by IIF) has low specificity — MPO confirmation by ELISA is essential
- p-ANCA/MPO-ANCA is the hallmark of MPA, and skin is involved in nearly half of MPA cases — often as the presenting feature
- ~10% of GPA patients have p-ANCA (not c-ANCA); these must be distinguished from MPA
- Dual positivity (p-ANCA + c-ANCA) should always raise suspicion for drug-induced vasculitis or levamisole-cocaine exposure
- HNE-ANCA is a useful differentiator: positive in cocaine/levamisole vasculitis, negative in true GPA/MPA
- ANCA testing does not replace clinical evaluation, histopathology, and organ-specific investigations
- ANCA positivity in skin-limited vasculitis warrants systemic workup (renal, pulmonary), since AAV underlies ~10% of such cases
Sources: Andrews' Diseases of the Skin, 13th ed.; Dermatology, 5th ed. (Elsevier); Fitzpatrick's Dermatology, 9th ed.
This is a shared conversation. Sign in to Orris to start your own chat.