Tonsillectomy. Indications Contraindications describe the oropharyngeal findings, explain prevention
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Tonsillectomy
Oropharyngeal Anatomy — Tonsil Bed
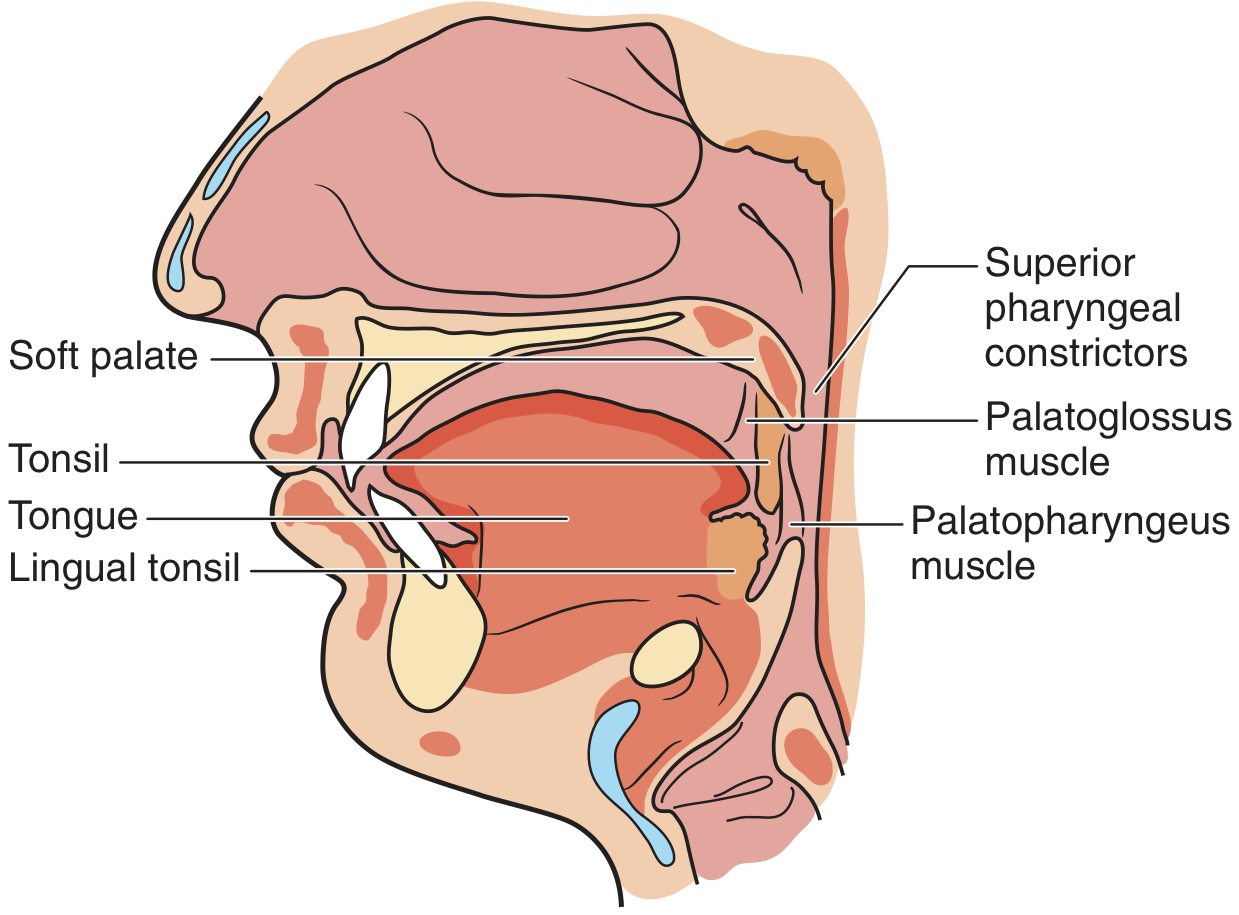
The palatine tonsils sit within the tonsillar fossa of the oropharynx. Key relationships:
| Border | Structure |
|---|---|
| Superior | Soft palate |
| Inferior | Lingual tonsil |
| Deep | Superior constrictor muscle |
| Anterior | Palatoglossus muscle (anterior pillar) |
| Posterior | Palatopharyngeus muscle (posterior pillar) |
Vascular supply:
- Superior pole — ascending pharyngeal artery, lesser palatine artery
- Inferior pole — tonsillar branches of the facial artery, dorsal lingual artery, ascending palatine artery
The inferior pole is the dominant vascular entry point; hemostatic effort directed here first controls most intraoperative bleeding.
Oropharyngeal Findings Warranting Tonsillectomy
On examination, findings that prompt surgical referral include:
- Tonsillar hypertrophy — enlargement that narrows the oropharyngeal airway; graded on the Brodsky scale (1–4+); 3+ to 4+ tonsils significantly reduce the airway lumen
- Asymmetric tonsil enlargement — raises concern for neoplasm (lymphoma, squamous cell carcinoma); requires biopsy
- Tonsillar exudate / cryptic debris — recurrent or chronic purulent exudates in the crypts suggest chronic bacterial tonsillitis (mixed flora, often with beta-lactamase-producing organisms in adults)
- Peritonsillar fullness or bulging — unilateral anterior displacement of the soft palate and tonsil with contralateral uvular deviation is classic for peritonsillar abscess
- Tonsillar surface irregularity or ulceration — hard, irregular, ulcerated, or fixed tonsil may represent malignancy
- Retrognathia / micrognathia or dental malocclusion — may be secondary to adenotonsillar hypertrophy causing craniofacial remodeling
— Pfenninger and Fowler's Procedures for Primary Care, 3e, p. 547–549
Indications for Tonsillectomy
Absolute Indications
- Tonsillar hypertrophy causing obstructive sleep symptoms (children or adults) leading to adverse pulmonary or cardiovascular consequences (cor pulmonale, pulmonary hypertension)
- Hypertrophy with airway obstruction leading to craniofacial bone malformation or dental malocclusion
- Hypertrophy causing dysphagia and poor weight gain
- Recurrent peritonsillar abscesses requiring drainage that fail to resolve with appropriately dosed antibiotics
- Febrile convulsions triggered by tonsillitis episodes
- Suspected malignancy — suspect growth or anatomic characteristics requiring biopsy to exclude neoplasm
Relative Indications
- Recurrent acute tonsillitis — 3 or more documented episodes per year causing missed work/school requiring medical treatment; some clinicians use the Paradise criteria (6–7 episodes in 1 year, 5/year × 2 years, or 3/year × 3 years) particularly in children
- Chronic tonsillitis
- Obstructive sleep apnea (OSA) — adenotonsillectomy is first-line in pediatric OSA
- Persistent halitosis or foul taste not responding to medical therapy (tonsillar crypt disease)
- Streptococcal carrier state with chronic bouts unresponsive to beta-lactamase–resistant antibiotics
- Nocturnal enuresis with coexistent obstructive sleep disorder from adenotonsillar hypertrophy
- ADHD resistant to treatment with coexistent upper airway obstructive sleep disorder
Acute "Quinsy" (Hot) Tonsillectomy Indications
- Recurrent peritonsillar abscess
- Massive tonsils causing acute airway obstruction
- Patient already under general anesthesia due to comfort/exposure issues
— Pfenninger and Fowler's Procedures for Primary Care, 3e; K. J. Lee's Essential Otolaryngology; Cummings Otolaryngology
Contraindications
| Contraindication | Notes |
|---|---|
| Poor anesthetic risk | ASA class IV or unstable cardiopulmonary disease |
| Uncontrolled systemic illness | Diabetes, cardiac failure, uncontrolled hypertension |
| Anemia | Correct pre-operatively before elective surgery |
| Active acute bilateral tonsillitis | Defer until infection resolves (increased bleeding risk) |
| Coagulopathy / anticoagulated patient | Reverse coagulopathy or anticoagulation first; consult otolaryngology |
Special caution groups (not absolute contraindications, but require close monitoring):
- Children < 3 years or with history of prematurity
- Seizure disorders, neuromuscular conditions, or asthma
- Severe obstructive sleep apnea (risk of post-obstructive pulmonary edema after removal of obstruction)
- Cardiovascular defects or heart murmurs (require perioperative antibiotic prophylaxis)
— Pfenninger and Fowler's Procedures for Primary Care, 3e, p. 548–549
Prevention (Post-tonsillectomy Hemorrhage Prevention)
Post-tonsillectomy hemorrhage is the primary serious complication. It occurs:
- Primarily — intraoperatively or immediately postoperatively
- Secondary — 5–7 days after surgery when eschar sloughs
Prevention strategies include:
- Antibiotic prophylaxis — intraoperative IV antibiotics (e.g., ampicillin) followed by a 1-week oral course have been shown to significantly reduce postoperative morbidity
- Local anesthetic injection — into the tonsillar bed at the start of surgery may decrease hemorrhage and improve postoperative recovery
- Directed hemostasis — controlling the superior and inferior poles first (primary vascular entry points) before addressing the tonsillar bed at large
- Surgical technique — gentle, careful removal of all tonsillar tissue reduces postoperative pain and recovery time; complete removal reduces risk of bleeding and recurrence (especially in intracapsular procedures)
- Pre-operative workup — CBC, PT/INR, and bleeding time when there is any suspicion of a bleeding disorder
- Avoid loose deciduous teeth — evaluate and remove extremely loose teeth that could be dislodged and threaten the airway intraoperatively
Types of Tonsillectomy and Prevention Implications
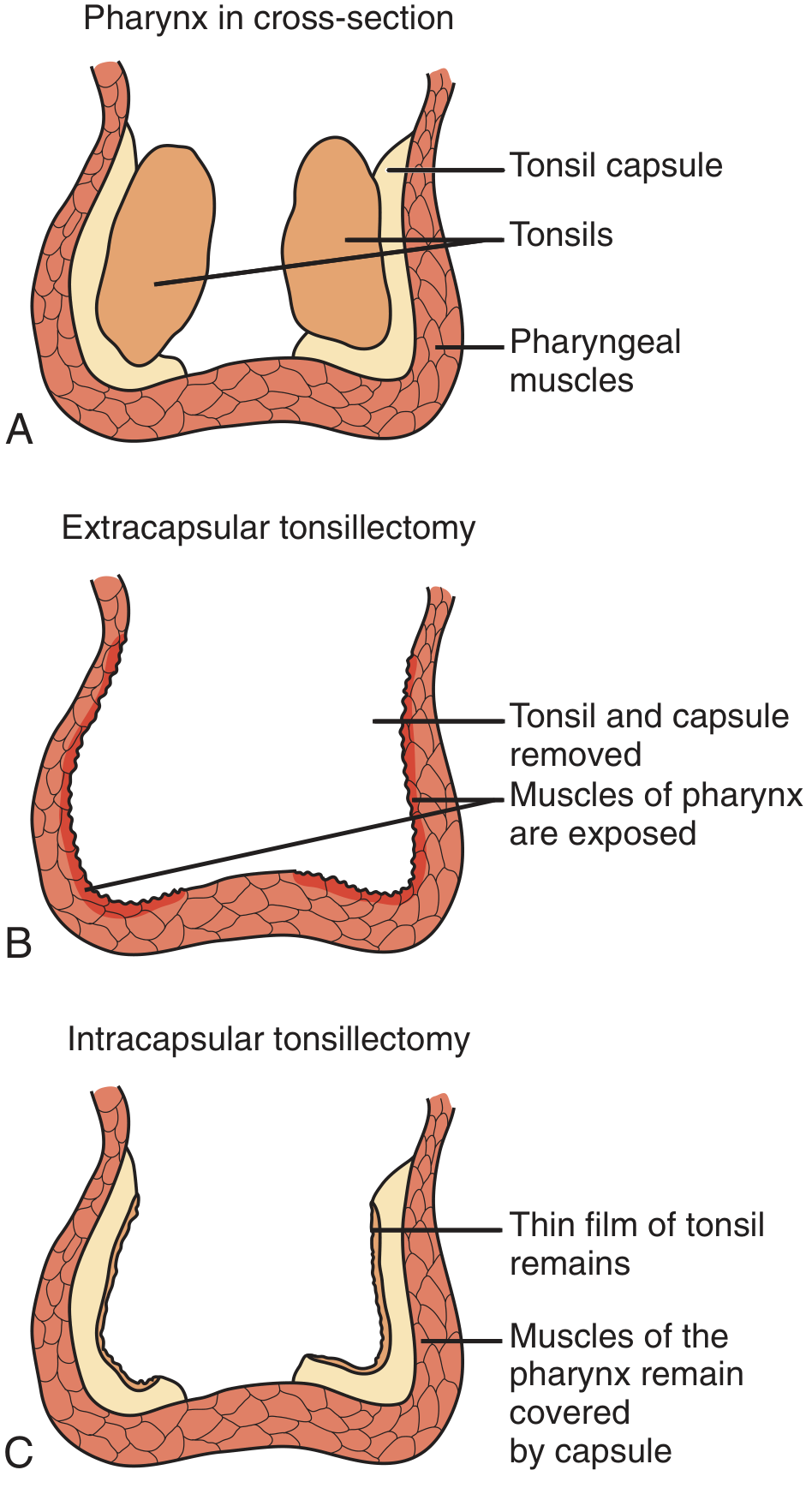
- Extracapsular (subcapsular) — removes tonsil and capsule entirely; pharyngeal muscles left to re-epithelialize; currently the favored technique
- Intracapsular (tonsillotomy) — removes tonsillar body only, capsule remains; theoretically less pain and faster recovery, but leaves residual tissue with risk of recurrence and bleeding if all tonsillar tissue is not removed
— Pfenninger and Fowler's Procedures for Primary Care, 3e, p. 549–550; Cummings Otolaryngology Head and Neck Surgery
Give me more detailed information
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
The response above covers the full detail across all four domains. Here is a brief orientation to what was added beyond the previous summary:
Oropharyngeal findings — expanded with the Brodsky grading scale image (0 to +4, measured as percentage of oropharyngeal width occupied), craniofacial sequelae of chronic obstruction, microbiology of adult tonsils, and detailed clinical signs distinguishing chronic tonsillitis from peritonsillar abscess from suspected malignancy.
Indications — added frequency thresholds table (Paradise-based), detailed OSA/OSAS pathophysiology through to cor pulmonale, STOP-BANG and STBUR screening tools, cardiac endocarditis as an absolute indication, and specific peritonsillar abscess timing (acute "quinsy" vs. delayed interval tonsillectomy).
Contraindications — expanded with OSA-specific admission thresholds (AAO-HNS: AHI ≥ 10 or SpO₂ < 80%; AAP: AHI ≥ 24 or EtCO₂ ≥ 60 mmHg), and a detailed high-risk groups table with rationale for each.
Prevention — stratified into pre-operative, intraoperative, and post-operative phases; added the "six hours or six days" hemorrhage guideline, full analgesic safety data (codeine FDA contraindication, ketorolac contraindication, NSAIDs safety, ondansetron dosing), post-operative antibiotic evidence summary (Cochrane: no benefit beyond fever reduction), and OSA cure rate evidence table from major trials.
Detailed information
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Tonsillectomy — Detailed Indications
I. Infection-Based Indications
A. Recurrent Acute Tonsillitis — Frequency Thresholds
The most widely cited benchmark for surgical candidacy is based on documented, clinically verified episodes:
| Frequency | Time Period |
|---|---|
| ≥ 7 episodes of acute tonsillitis | Within 1 year |
| ≥ 5 episodes per year | Over ≥ 2 consecutive years |
| ≥ 3 episodes per year | Over ≥ 3 consecutive years |
| ≥ 2 weeks of school or work missed | In 1 year, due to tonsillitis |
Episodes must be documented by a clinician and should involve objective signs (fever, tonsillar exudate, cervical adenopathy, or positive streptococcal test). Children with less severe or less frequent disease are unlikely to have long-term benefit from surgery.
Adenotonsillectomy decreases the number of episodes of sore throat and days with sore throat in children in the first year after surgery, but its value in adults is less clear. Many adults improve spontaneously, and the potential benefit must be weighed against risks including hemorrhage and pain, which is more severe in adults. — Goldman-Cecil Medicine, 2e
B. Chronic Tonsillitis
Patients develop deep tonsillar crypts that accumulate food debris and sloughed mucosa — an ideal anaerobic environment. Features:
- Whitish/yellow caseous material extruding from crypts (tonsilloliths)
- Foul taste and odor, chronic halitosis
- Chronic sore throat from persistent bacterial growth
Medical approach first:
- Frequent gargling with hydrogen peroxide mouthwash
- Manual expression of cryptic debris
- Long-term amoxicillin (500 mg TID × 21 days) or clindamycin (300 mg TID × 21 days)
When tonsillectomy is indicated:
- Presence of Actinomyces (commensal that colonizes tonsillar crypts) — even long-term antibiotics are unlikely to eradicate it
- Persistent symptoms despite maximal medical therapy
- Recurrent episodes with peritonsillar abscess
C. Peritonsillar Abscess (PTA / Quinsy)
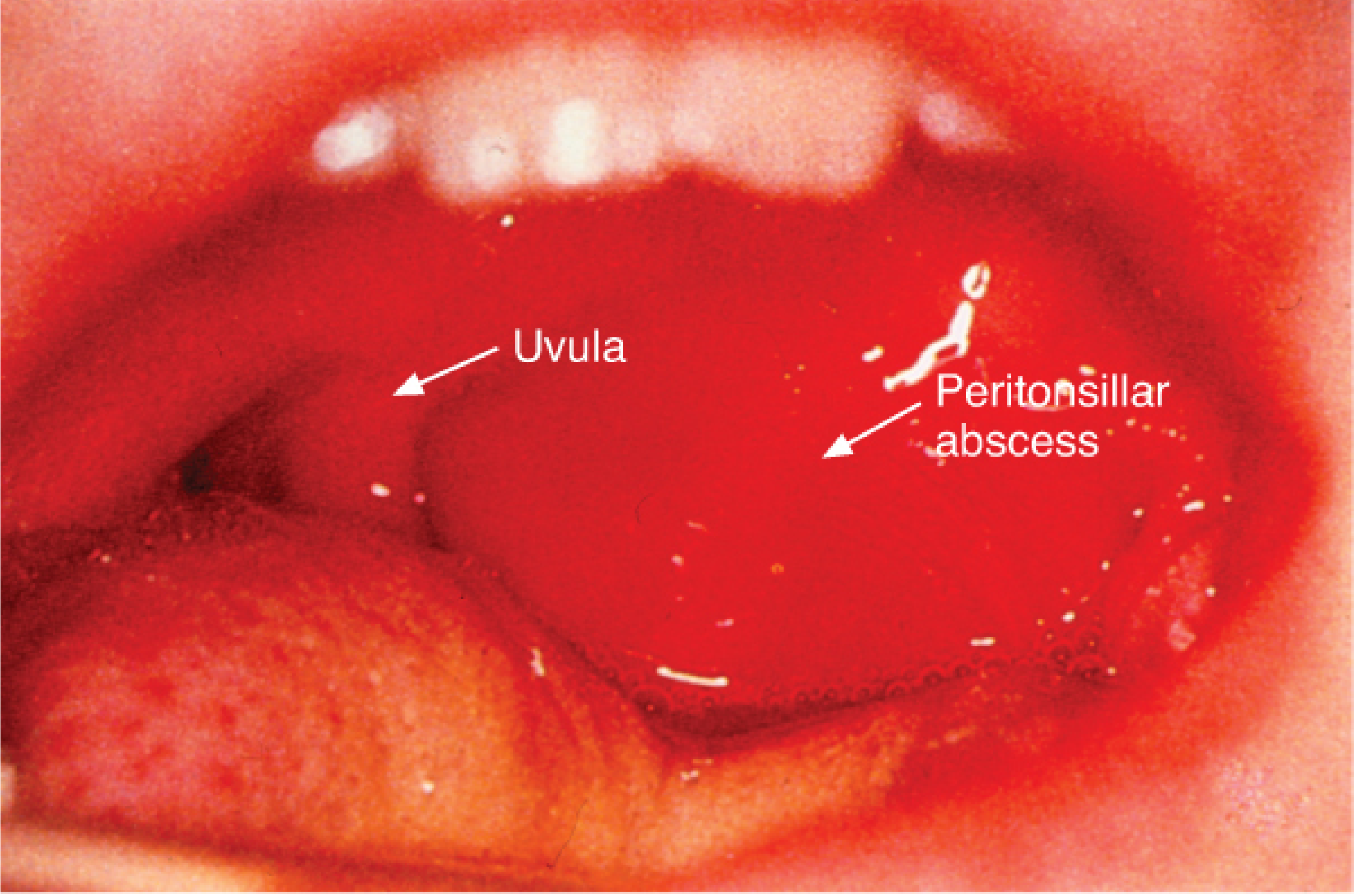
The classic oropharyngeal finding is anterior displacement of the soft palate and tonsil with contralateral uvular deviation. Approximately 90% of patients are successfully treated with incision and drainage ± antibiotics.
Tonsillectomy is indicated in two distinct settings:
1. Delayed (Interval) Tonsillectomy — after resolution of acute infection
- Recurrent peritonsillar abscess
- Recurrent/chronic tonsillitis
- Tonsillar hypertrophy with obstructive symptoms
2. Acute "Quinsy" Tonsillectomy — in the hot setting
- Recurrent PTA in a patient with strong indications (OSA, recurrent tonsillitis)
- Massive tonsils causing acute airway obstruction
- Patient already under general anesthesia (poor exposure or discomfort precludes adequate drainage)
"Quinsy tonsillectomy" should only be considered when patients have a strong independent indication for tonsillectomy, such as sleep apnea, recurrent tonsillitis, or recurrent peritonsillar abscess. — Tintinalli's Emergency Medicine
D. Streptococcal Carrier State
Patients who are carriers of Group A beta-hemolytic Streptococcus (GABHS) with chronic, recurrent episodes that do not respond to beta-lactamase–resistant antibiotics are surgical candidates. Important context:
- Adult tonsils harbor mixed flora, with three-fourths containing beta-lactamase–producing organisms — explaining why standard penicillin fails in 7–37% of cases
- Theories of penicillin failure include protective beta-lactamase produced by commensal bacteria, poor tissue penetration, and lack of GABHS-inhibiting flora
E. Diphtheria Carrier State
Corynebacterium diphtheriae carriers — particularly when culture reveals toxigenic strains — are a recognized surgical indication, especially relevant in areas where vaccination coverage is incomplete. — K. J. Lee's Essential Otolaryngology
II. Obstructive / Sleep-Disordered Breathing Indications
A. Pathophysiology Cascade — OSAS → Cor Pulmonale
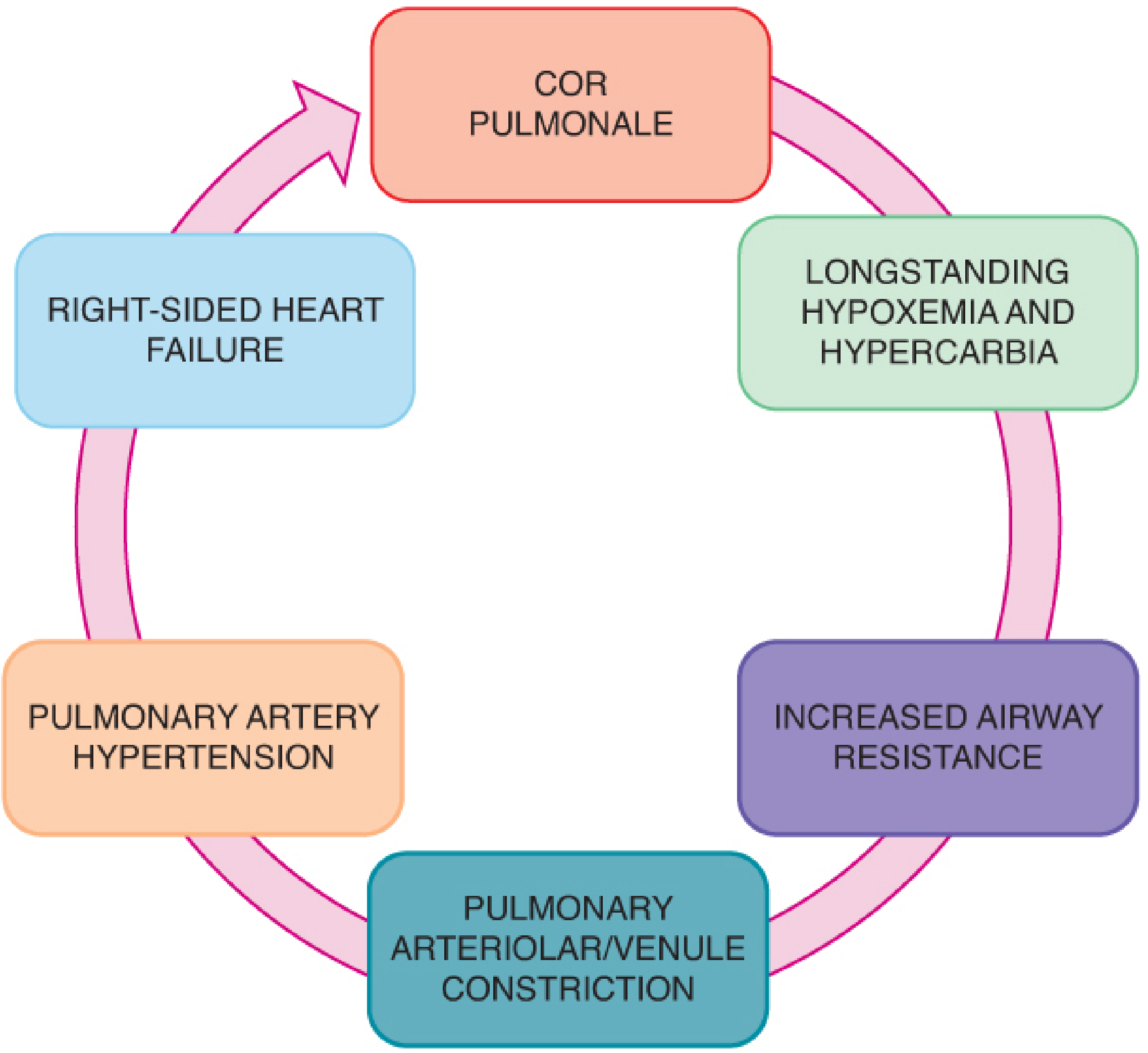
The pathway from untreated OSAS to end-organ damage:
- Tonsillar hypertrophy → increased upper airway resistance
- Repetitive obstruction → episodic hypoxemia + hypercarbia
- Hypoxic pulmonary arteriolar/venule constriction
- Sustained pulmonary artery hypertension
- Cor pulmonale — right ventricular hypertrophy, ECG changes, cardiomegaly
- Right-sided heart failure
Each apneic episode also causes significant systemic and pulmonary artery pressure spikes, ventricular dysfunction, and cardiac dysrhythmias. Cardiac enlargement is frequently reversible after adenotonsillectomy.
Long-term systemic effects of untreated OSAS beyond the airway:
- Neurobehavioral: OSAS duration correlates with irreversible prefrontal cortex neurochemical alteration; episodic hypoxia causes neuronal loss; hyperactivity and elevated C-reactive protein
- Metabolic: OSAS is a risk factor for metabolic syndrome (insulin resistance, dyslipidemia, hypertension) in obese children
- Cardiovascular: altered blood pressure regulation, endothelial dysfunction, systemic hypertension, changes in left ventricular geometry, systemic inflammation (interleukin elevation — reversed by tonsillectomy)
B. OSAS Classification and Types
| Type | Characteristics |
|---|---|
| Type 1 OSAS | Lymphoid hyperplasia without obesity — classic pediatric form |
| Type 2 OSAS | Obese patients with minimal lymphoid hyperplasia |
- SDB affects 10% of the population; only 1–4% progress to frank OSAS
- OSAS in children peaks in preschool and school age (~10% prevalence), thought to decline after age 9
- BMI ≥ 95th percentile for age is an independent predisposing factor
C. OSAS Screening
Adults — STOP-BANG Questionnaire:
| Letter | Domain |
|---|---|
| S | Snoring loud enough to be heard through closed doors |
| T | Tired/somnolent during the day |
| O | Observed apnea during sleep |
| P | Blood Pressure elevated or treated |
| B | BMI > 35 |
| A | Age > 50 |
| N | Neck circumference > 40 cm |
| G | Gender: male |
Children — STBUR Questionnaire:
- S: Snoring
- T: Trouble Breathing during sleep
- B/UR: Un-Refreshed after sleep
A reliable predictor of children at perioperative respiratory risk.
D. Role of Polysomnography (PSG) Before Surgery
The indications are debated between major guidelines:
| Organization | PSG Recommendation |
|---|---|
| AAP | Recommends PSG when alternative screening methods are inconclusive; acknowledges inadequate infrastructure for universal PSG |
| AAO-HNS | Recommends PSG only when there is discordance between tonsillar size and reported OSAS symptoms |
| Practice reality | Only 3.5% of pediatric otolaryngologists refer > 90% of children for PSG before adenotonsillectomy (2017 survey) |
E. Surgical Outcomes for OSAS
Adenotonsillectomy is first-line treatment for OSAS in otherwise healthy children, carrying a ~80% success rate in resolving OSAS overall.
| Study | Population | Cure Rate | AHI Threshold |
|---|---|---|---|
| Friedman meta-analysis (23 studies, 1079 pts) | Mixed | 66.3% | AHI < 1–5 |
| Friedman (strict definition) | Mixed | 59.8% | AHI < 1 |
| Bhattacharjee (578 children) | Pediatric | 27.2% | AHI < 1 |
| CHAT RCT (464 children, ages 5–9) | Pediatric | 79% at 7 months | AHI < 2 |
Predictors of residual/persistent SDB after surgery:
- Age > 7 years
- Obesity (obese children: 33–76% persistent OSA vs. 15–37% non-obese)
- Severe pre-operative OSA
- Chronic asthma
- Black race (CHAT trial)
- Craniofacial abnormalities
If adenotonsillectomy fails → CPAP is next-line. Additional surgical options for craniofacial/complex cases: expansion pharyngoplasty, supraglottoplasty, mandibular distraction osteogenesis (MDO — 92% improvement/resolution in Pierre Robin Sequence and Treacher Collins syndrome), uvulopharyngopalatoplasty.
F. Hypertrophy Causing Physical Deformity or Developmental Problems
- Craniofacial bone malformation or dental malocclusion from chronic open-mouth posture and abnormal muscular forces — requires tonsillectomy before orthodontic/dental correction
- Dysphagia and poor weight gain — especially in young children; surgical relief is associated with normalization of weight gain
- Speech abnormalities — hyponasality and muffled "hot potato" voice quality from oropharyngeal crowding
III. Neoplastic Indications
A. Suspicion of Tonsillar Malignancy
Oropharyngeal findings that mandate biopsy/tonsillectomy:
- Unilateral tonsillar enlargement without symptoms of infection — particularly in adults
- Asymmetric, indurated, firm, or fixed tonsil
- Surface ulceration or irregular mucosa
- Rapidly enlarging tonsil
- Ipsilateral cervical lymphadenopathy without infectious cause
Relevant malignancies:
- HPV-related oropharyngeal squamous cell carcinoma (HPV-16 and -18; high p16 expression; often in non-smokers; favorable prognosis relative to non-HPV OPSCC)
- Standard variant OPSCC (smokers/drinkers)
- Lymphoma (tonsil and base of tongue)
- Minor salivary gland tumors
B. Search for Unknown Primary
When a patient presents with cervical squamous cell carcinoma metastasis from an unknown primary, diagnostic tonsillectomy (often performed via Transoral Robotic Surgery — TORS) is performed to search for an occult tonsillar primary. This is a well-established otolaryngologic indication.
C. Treatment of Early-Stage Tonsillar Cancer
Tonsillectomy with adequate margins can serve as therapeutic resection for early-stage tonsillar carcinoma, increasingly performed with robotic assistance (TORS). — K. J. Lee's Essential Otolaryngology
IV. Miscellaneous / Special Indications
A. Febrile Convulsions
Tonsillitis-triggered febrile seizures in children constitute an absolute indication — recurrent febrile convulsions driven by tonsillar infection should prompt surgery.
B. PFAPA Syndrome (Periodic Fever, Aphthous Ulcers, Pharyngitis, Adenopathy)
- Characterized by cyclical fevers every 3–6 weeks
- Corticosteroids (e.g., prednisolone) resolve episodes within 24 hours for most patients but may shorten intervals between episodes
- Cimetidine (H₂ antagonist) effective for prophylaxis in a minority
- NSAIDs are generally ineffective
- Tonsillectomy — small-scale studies show success in resolving periodic fevers, though at similar rates to medical treatment/observation; relapse after tonsillectomy has been documented. Tonsillectomy offers symptomatic benefit for pharyngitis in PFAPA patients and may be considered when pharyngitis symptoms are severe
C. IgA Nephropathy
Tonsils serve as a source of aberrantly glycosylated IgA1 and tonsillar mucosal antigen stimulation drives the nephropathy. Tonsillectomy combined with steroid pulse therapy has been shown to significantly impact clinical remission and may delay progression to end-stage kidney disease in Asian populations; however, tonsillectomy alone does not consistently prevent progressive disease. It is not routinely recommended outside Japan/Asia by most guidelines.
D. Cardiac Valvular Disease with Recurrent Streptococcal Bacteremia
Patients with cardiac valvular disease at risk for infective endocarditis from chronically infected tonsils are candidates. These patients require perioperative antibiotic prophylaxis.
E. Nocturnal Enuresis with Adenotonsillar Hypertrophy
Disrupted sleep architecture from upper airway obstruction is associated with nocturnal enuresis; tonsillectomy addresses the underlying obstructive cause.
F. ADHD Resistant to Treatment with Coexistent OSAS
Neurobehavioral impairment driven by sleep fragmentation and episodic hypoxia may present as ADHD-like symptoms. When standard pharmacotherapy fails and obstructive sleep disorder is identified, adenotonsillectomy is a recognized option.
Sources: Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e | Cummings Otolaryngology Head and Neck Surgery | K. J. Lee's Essential Otolaryngology | Pfenninger and Fowler's Procedures for Primary Care, 3e | Goldman-Cecil Medicine, 2e | Tintinalli's Emergency Medicine | Miller's Anesthesia, 10e
Give prevention in detail
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Now I have comprehensive material. Let me compile the full, detailed prevention response.
Tonsillectomy — Prevention in Detail
Prevention spans five phases: pre-operative optimization, intraoperative technique, pharmacological prevention, post-operative management, and emergency management of complications.
I. Pre-operative Prevention
A. Hematological and Coagulation Screening
| Test | Indication |
|---|---|
| CBC (FBC) | Detect pre-existing anemia; baseline hemoglobin |
| PT / INR | Identify coagulopathy |
| Bleeding time / platelet function | Suspected platelet disorder or aspirin use |
These are not routine for all patients but are mandatory when:
- Personal or family history of abnormal bleeding
- Use of aspirin-containing OTC cold/allergy medications (many contain aspirin, which impairs platelet function — must be identified and stopped ≥ 7–10 days pre-operatively)
- Clinical suspicion of von Willebrand disease or other coagulopathy
B. Cardiac and Respiratory Pre-assessment
- Chest X-ray and ECG — not routine; indicated only with history of cor pulmonale, recent pneumonia, bronchitis, or URI
- Echocardiogram — children with history of cardiac abnormalities or suspected cor pulmonale from longstanding OSAS
- Polysomnography (PSG) — indicated when there is discordance between tonsillar size and severity of OSAS symptoms (AAO-HNS guideline), or when clinical screening is inconclusive (AAP guideline)
C. Airway Risk Assessment
A thorough physical examination before surgery must include:
- Observation for audible respirations, mouth breathing, chest retractions, nasal voice quality
- Inspection of the oropharynx for tonsillar size (Brodsky grade) — determines ease of mask ventilation and intubation
- Note elongated face, retrognathic mandible, high-arched palate — signs of craniofacial remodeling from chronic obstruction
- Inspiratory stridor or prolonged expiration — signals significant pre-existing partial airway obstruction
D. Medication Review
- Aspirin / NSAIDs — stop ≥ 7–10 days pre-operatively (platelet dysfunction increases intraoperative and post-operative bleeding)
- Anticoagulants — bridging strategy or temporary cessation discussed with prescribing clinician
- Antihistamines containing aspirin — common in OTC preparations; parents/patients must be specifically asked
- Antibiotics — if the patient is currently on antibiotics for active tonsillitis, defer elective surgery until infection fully resolves (inflamed, hyperemic tissue bleeds more)
E. Dental Assessment
Evaluate and potentially remove extremely loose deciduous teeth before surgery — intraoperative dislodgment can obstruct the airway. All teeth should be documented and checked at end of procedure.
F. Anaesthetic Pre-medication Caution
- Sedative premedication should be avoided in children with OSAS, intermittent airway obstruction, or very large tonsils — blunts pharyngeal dilator muscle tone and can precipitate complete obstruction
- Antisialagogue (e.g., glycopyrrolate) may be used to minimize secretions in the operative field
- IV access and hydration established before induction — vigorous intraoperative IV hydration offsets reduced postoperative oral intake
G. NPO (Nil Per Os) Fasting
- Solid foods: nil ≥ 8 hours before surgery
- Standard clear fluid fasting applies per anaesthetic guidelines
H. Pre-operative Antibiotic Prophylaxis
- Intraoperative IV antibiotics (e.g., ampicillin) followed by a 1-week oral antibiotic course have been shown to significantly reduce postoperative morbidity
- Children with cardiovascular defects or heart murmurs must receive appropriate perioperative antibiotic prophylaxis against infective endocarditis
II. Intraoperative Prevention
A. Anaesthetic Management — Key Preventive Steps
- Avoid sedative premedication in OSAS patients (see above)
- Induction: Volatile inhalation induction is standard in children; propofol can be used as an alternative to neuromuscular blockade by deepening anaesthesia
- Airway protection options:
- Cuffed endotracheal tube — provides best airway protection; cuff inflation pressure must be carefully monitored to prevent post-extubation croup
- Flexible LMA — increasingly used; protects vocal cords from blood/secretions; the standard rigid LMA does not fit under the mouth gag and is easily compressed
- Supraglottic packing with petroleum gauze OR use of a cuffed ETT — prevents blood from entering the trachea intraoperatively
- Throat pack with retrieval string — prevents swallowed blood from reaching the stomach; reduces post-operative nausea; string is taped to face with a small hemostat and must be documented and removed before extubation
- Orogastric tube decompression — decompresses the stomach of swallowed blood and insufflated air, reducing post-operative nausea and vomiting (PONV)
- Monitoring: precordial stethoscope, ECG, automated NIBP, pulse oximetry, end-tidal capnography (EtCO₂)
For patients with OSAS:
- Standard opioid doses reduced by 50% due to increased opioid sensitivity in OSAS patients
- Avoid sedative premedication and heavy opioid loading
- Dexmedetomidine 0.5–1 mcg/kg infused during the procedure — attenuates emergence delirium in toddlers; also useful in DISE procedures
B. Surgical Technique to Prevent Hemorrhage
Hemostatic principle — direct effort to the poles first:
The inferior pole receives the dominant blood supply (facial artery branches, dorsal lingual artery, ascending palatine artery). Directing hemostatic effort here first controls the majority of potential intraoperative bleeding. Only two minor branches enter the superior pole.
| Technique | Mechanism | Notes |
|---|---|---|
| Cold steel (knife and snare) | Mechanical dissection | Oldest method; bleeding controlled separately by cautery, packing, or suture |
| Monopolar electrocautery | Most popular; good hemostasis during dissection | Greater thermal injury; associated with more postoperative pain and longer healing |
| Bipolar cautery | Precise coagulation; less tissue injury | Used with operating microscope or bipolar scissors |
| Coblation (plasma excision) | Radiofrequency via saline field; breaks molecular bonds at low temperature (60°C vs. 400°C for monopolar) | Conflicting data on pain reduction; Cochrane review (9 trials) found no significant differences in pain or recovery speed. Higher delayed hemorrhage rate reported (up to 11.1%) |
| Harmonic Scalpel | Ultrasonic vibration at 55,500 Hz; breaks hydrogen bonds | Controls bleeding at poles; requires separate sharp component for tough tissue; conflicting results on pain benefit |
| PITA (Powered Intracapsular Tonsillectomy and Adenoidectomy / microdebrider) | Removes bulk of tonsil; preserves capsule as a biological dressing | Two large retrospective studies (4776 and 2943 patients) found significant reduction in delayed postoperative bleeding and dehydration readmission. Risk: tonsillar regrowth (6% in one study at 6 months) |
Technique choice principle: the best method is the one with which the surgeon has the most experience. All studies agree that gentle, careful removal of all tonsillar tissue reduces post-operative pain scores and recovery time. Incomplete removal → increased risk of bleeding and recurrence (especially relevant in intracapsular/tonsillotomy).
C. Local Anaesthetic Injection — Pre-incision
- Pre-incision peritonsillar infiltration with local anaesthetic + adrenaline/epinephrine:
- Reduces intraoperative blood loss
- Reduces bleeding through vasoconstrictive effect
- Shown to provide a more rapid return to activity compared with general anaesthesia alone
- Does not significantly decrease postoperative pain (post-hoc operative site anaesthesia has limited duration)
D. Emergence from Anaesthesia
- Emergence should be rapid — child should be alert and able to protect the recently instrumented airway before transfer to recovery
- Child must be awake and able to clear blood and secretions from the oropharynx before extubation
- Maintenance of pharyngeal and airway reflexes is essential to prevent aspiration, laryngospasm, and airway obstruction
- There is no difference in airway complication rates between awake vs. deep extubation — both acceptable
- Avoid stimulating the larynx during emergence
III. Pharmacological Prevention
A. Pain Prevention (Multimodal Analgesia)
The principle is multimodal analgesia — combining agents with different mechanisms to achieve additive/synergistic effects while minimising individual agent doses and side effects.
1. Acetaminophen (Paracetamol) — First-Line
Mechanism: Central COX inhibition, enhancement of descending serotonergic pathways, indirect CB1 receptor activation, nitric oxide/NMDA pathway inhibition.
- IV acetaminophen — faster onset than oral (analgesia within 15 minutes, fever reduction within 30 minutes); reduces need for rescue opioid after tonsillectomy; higher cost limits routine use
- Oral: effective for mild–moderate pain; give regularly (not PRN) for best results
- Rectal: 40 mg/kg rectal vs. 15 mg/kg IV — study showed median time to rescue analgesia of 10 and 7 hours respectively when combined with fentanyl 1–2 mcg/kg
- Safe in all age groups including children post-tonsillectomy
2. NSAIDs — Safe When Used Appropriately
- Cochrane meta-analysis (36 studies; 1747 children + 1446 adults): no increased risk of bleeding with NSAIDs after tonsillectomy — no increase in general bleeding, most severe bleeding, secondary hemorrhage, readmission, or re-operation for bleeding
- Results consistent across: single vs. multiple doses, pre- vs. post-operative administration, and different NSAID types
- Intraoperative NSAIDs should be avoided to decrease hemorrhage risk during surgery; safe and effective in the post-acute recovery period
- Recommended by both AAO-HNS and PROSPECT guidelines as part of standard analgesic regimen
Exception: Ketorolac is contraindicated — hemorrhage rates 4.4–18% in tonsillectomy patients.
3. Corticosteroids — Dexamethasone
- Single intraoperative dose of dexamethasone is recommended by AAO-HNSF for all children undergoing tonsillectomy
- Benefits: reduces oedema formation, reduces PONV, decreases postoperative discomfort, shortens time to oral intake
- Dose: 0.5 mg/kg IV (with or without ondansetron)
- Concern about increased bleeding risk has not been consistently confirmed — current guidelines support its use
- Post-operative oral dexamethasone: 0.03–0.3 mg/kg/day (children), 0.75–9 mg/day (adults), divided into two doses
- Greatest benefit when given on post-operative day 3 (when most patients experience peak discomfort)
- Instituting for 3–4 days at this point reduces pain and increases oral intake with minimal side effects
4. Codeine — Contraindicated in Children
- Codeine is metabolized by CYP2D6 to morphine (active metabolite)
- Two pharmacogenomic variants are dangerous:
- Poor metabolizer — codeine is ineffective (one polymorphism)
- Ultra-rapid metabolizer — dangerous morphine accumulation occurs (different polymorphism)
- FDA 2013 Black Box Warning: following review of 10 deaths and 3 overdoses (8 occurring after adenotonsillectomy, 1969–2012)
- FDA 2017: Codeine contraindicated in children < 12 years; warned against use in adolescents aged 12–18 with obesity or OSA
- AAO-HNS guidelines: codeine strictly contraindicated in pediatric tonsillectomy
- Acetaminophen with codeine has NOT been shown to be superior to acetaminophen alone in post-tonsillectomy pain
5. Gabapentinoids
- Gabapentin 600 mg twice daily on the day of surgery, then 600 mg three times daily for 5 subsequent days → significant opioid-sparing effect after tonsillectomy; potential adverse effects: sedation, dizziness, gait disturbance
- Gabapentin 1200 mg orally pre-operatively showed intraoperative and post-operative analgesic effects in head and neck surgery
- Pregabalin reduces early post-operative pain scores and opioid consumption after tonsillectomy
- Lower doses (300 mg BD) did not reduce opioid use but showed meaningful pain score reductions with comparable side-effect profiles
6. NMDA Receptor Antagonists — Ketamine
- Low-dose ketamine: acts as an antihyperalgesic (limits central sensitization) rather than a primary analgesic
- Cochrane review: IV ketamine reduces both post-operative analgesic requirement and pain intensity, with possible reduction in PONV, without significant CNS adverse effects at low doses
- Useful for severe post-operative pain and in opioid-tolerant patients
- Requires skilled supervision; safe use requires careful planning
7. Ondansetron — Prevention of PONV
- Ondansetron 0.10–0.15 mg/kg IV (with or without dexamethasone) — highly effective in reducing:
- Post-tonsillectomy nausea and vomiting
- Post-operative pain
- Time to first oral intake
- Adult dose: 6–8 mg IV every 6 hours
- Children: 0.15 mg/kg IV every 4–6 hours
- Promethazine is an alternative: 12.5–25 mg IV q4–6h (adults); 0.25–1 mg/kg IV q4–6h (children)
8. Sucralfate
- 1 teaspoon orally four times daily may benefit both children and adults in reducing mucosal pain during healing (topical mucosal protectant)
- Role is still debated but widely used as adjunct
IV. Post-operative Prevention and Management
A. Immediate Post-operative Care
| Action | Rationale |
|---|---|
| Continue IV fluids until tolerating oral fluids | Prevents dehydration; vigorous intraoperative IV hydration offsets poor post-operative intake |
| Start oral fluids when patient is awake and airway-protective | Avoid aspiration |
| Ice collars and cool mist vaporisers | Reduces swelling and local discomfort in children |
| Pulse oximetry monitoring | Detects occult hypoxaemia, especially in OSAS patients |
| Maintain sitting-upright position | Aids drainage; reduces aspiration risk if bleeding occurs |
B. Diet and Activity Restrictions
- Soft diet for 10–14 days — critical for preventing secondary (delayed) hemorrhage by avoiding disruption of the healing eschar
- Gradual return to normal activities over the same period
- Avoid strenuous physical activity during the healing period (Valsalva manoeuvre can dislodge eschar)
- Patients and carers must be counselled that a grayish-white eschar in the tonsillar fossa is normal — not a sign of infection
C. Post-operative Antibiotic Policy
| Evidence | Recommendation |
|---|---|
| Cochrane review: no impact on secondary hemorrhage rates, pain, analgesic use, or activity | Routine post-operative antibiotics not recommended by AAO-HNSF |
| Only significant benefit demonstrated: reduction of fever | May be justified in specific clinical contexts |
| Exception: Amoxicillin orally × 1 week has been shown to decrease overall morbidity | Some centres continue this practice |
D. Inpatient Admission Criteria (Prevention of Catastrophic Complications)
Children requiring post-operative inpatient monitoring (cardiorespiratory observation):
| Criterion | Organisation |
|---|---|
| AHI ≥ 10 events/hour or SpO₂ nadir < 80% | AAO-HNS |
| AHI ≥ 24 or SpO₂ nadir < 80% or peak EtCO₂ ≥ 60 mmHg | AAP |
Additional high-risk criteria warranting admission:
- Age < 8 years (higher respiratory complication risk)
- Pulmonary hypertension or other cardiac abnormalities
- Craniofacial syndromes
- Failure to thrive
- Hypotonia or neuromuscular disease
- Morbid obesity
- Severe pre-operative sleep study indices
In these patients:
- Narcotic analgesics should be avoided or severely limited
- May require: supplemental oxygen, steroids, nasopharyngeal airway, CPAP/BiPAP, or endotracheal intubation
- Neck pain after adenoidectomy persisting > 2 weeks → suspect C1–C2 subluxation (Grisel syndrome)
E. Prevention of Post-obstructive Pulmonary Oedema
This rare but life-threatening complication occurs when chronic upper airway obstruction is suddenly relieved:
Mechanism:
- Pre-operatively, inspiratory efforts against obstruction generate intrapleural pressures of −30 cmH₂O (vs. normal −2.5 to −10 cmH₂O)
- These negative pressures disrupt pulmonary microvascular capillary walls → fluid transudation into alveoli
- Concurrent expiratory "grunt" (similar to Valsalva) had been limiting pulmonary venous return — this protective mechanism is lost when obstruction is relieved
- Relief → increased venous return → pulmonary hydrostatic hyperaemia → frank pulmonary oedema
Prevention: anaesthesiologist may apply moderate positive end-expiratory pressure (PEEP) during induction
Treatment: oxygen, mechanical ventilation with PEEP, fluid restriction, diuretics, steroids
V. Emergency Management of Post-tonsillectomy Hemorrhage
Timing
| Hemorrhage Type | Timing | Aetiology |
|---|---|---|
| Primary | Within 24 hours | Related to surgical technique; 75% occurs within first 6 hours |
| Secondary (delayed) | Days 5–10 | Eschar separation; significantly higher in patients > 12 years |
"Six hours or six days" — the key clinical rule:
- 75% of post-operative tonsillar hemorrhage within 6 hours
- Remaining 25% within 24 hours
- Late bleeding possible up to post-operative day 6
- 67% bleeds from tonsillar fossa; 26% nasopharynx; 7% both
- Incidence: 0.1–8.1% overall; up to 11.1% with coblation technique
Immediate Emergency Steps
- Keep patient NPO — treat as full stomach (significant blood may have been swallowed)
- Sit patient upright with head forward — facilitates drainage and prevents aspiration
- Pulse oximetry and IV access — mandatory
- CBC, coagulation studies, type and cross-match blood
- Examine oropharynx — identify active bleeding site; note presence of normal gray-white eschar vs. active ooze/arterial jet
- Apply direct pressure to the bleeding tonsillar bed:
- Tonsillar pack or 4×4 gauze on a long clamp, moistened with thrombin or lidocaine with epinephrine
- Place a suture through the pack and tape to the face — prevents loss of pack into the airway
- Apply pressure to the lateral pharyngeal wall (avoid midline — stimulates gag reflex)
- Pressure alone can achieve control until otolaryngologist arrives
Pharmacological Haemostasis
| Agent | Route | Dose | Notes |
|---|---|---|---|
| Tranexamic acid (nebulised) | Inhaled | Adults: 1000 mg in 20 mL NS; Children: 250 mg if < 25 kg, 500 mg if > 25 kg | First-line pharmacological option for serious hemorrhage |
| Tranexamic acid | IV | Adults: 1000 mg (same as trauma dose) | For severe uncontrolled active bleeding; paediatric dosing not well validated |
| Silver nitrate | Topical | After local infiltration with 1% lidocaine + epinephrine | If discrete bleeding site is visible |
| Nebulised epinephrine | Inhaled | Standard dose | Alternative for temporising haemostasis |
Surgical and Advanced Management
- Cautery: if a specific bleeding point is visualised, cauterisation after local anaesthetic infiltration
- Return to OR: if initial measures fail — surgical haemostasis under general anaesthesia
- Treat as full stomach / rapid-sequence induction (blood swallowed; aspiration risk)
- Assess for orthostatic BP changes to estimate volume depletion
- Prepare duplicate laryngoscope blades, ETT sizes, and suction apparatus — blood may obscure cords and plug ETT
- Supraglottic airway (SGA/LMA) may serve as a rescue device if intubation is compromised
- In cases of massive bleeding where intubation is impossible: emergent cricothyrotomy must be planned before attempting intubation
- Endovascular embolisation: a definitive option for recurrent or surgically inaccessible bleeding
- Patients may suffer second or third hemorrhage — otolaryngology consultation in the ED is always required; discharge without specialist review is inappropriate
Sources: Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e | Cummings Otolaryngology Head and Neck Surgery | Pfenninger and Fowler's Procedures for Primary Care, 3e | Tintinalli's Emergency Medicine | Miller's Anesthesia, 10e | Goldman-Cecil Medicine, 2e
This is a shared conversation. Sign in to Orris to start your own chat.