If a patient take telvas 40 for b.p but even she can't control her b.p after it what will u prefer her
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
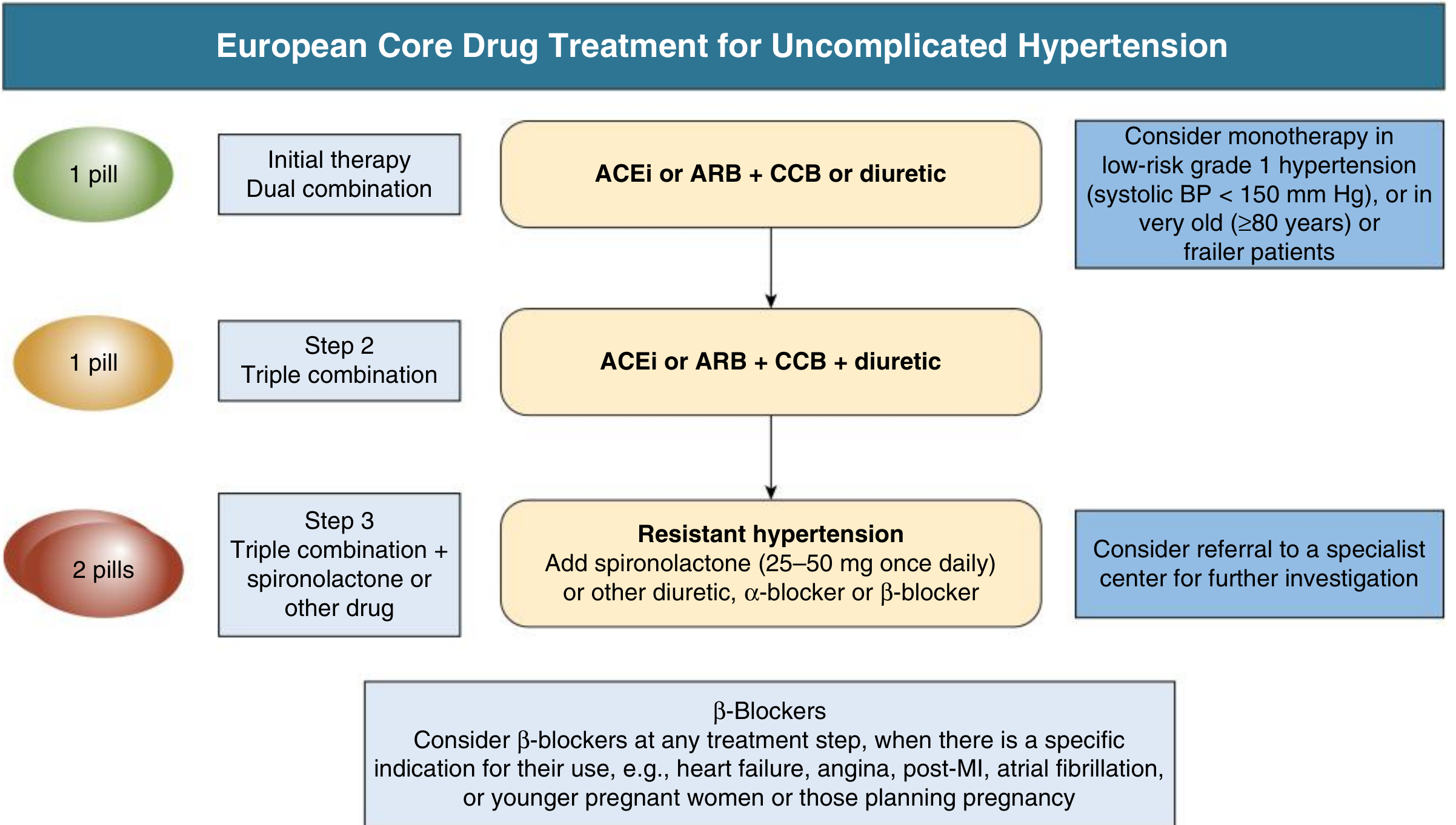
Telvas 40 = Telmisartan 40 mg, which is an ARB (Angiotensin Receptor Blocker). If BP is still not controlled on it, here is the stepwise approach backed by guidelines:
Step 1 — Optimize the current drug first
Before adding a new drug, check:
- Is she taking it regularly (compliance)?
- Is she on a low-salt diet?
- Any lifestyle factors (obesity, smoking, alcohol, stress)?
- Is 40 mg the maximum dose? Telmisartan can be uptitrated to 80 mg/day — this is often the first move.
Step 2 — Add a Second Drug (Combination Therapy)
If BP remains uncontrolled even at 80 mg telmisartan, add a second agent. The preferred combinations with an ARB are:
| Add-on Drug | Why preferred |
|---|---|
| Amlodipine 5–10 mg (Calcium Channel Blocker) | Most evidence, well-tolerated, synergistic BP lowering |
| Hydrochlorothiazide (HCTZ) 12.5–25 mg or Chlorthalidone (thiazide diuretic) | Good add-on, especially if fluid retention |
Fixed-dose combinations are available: Telmisartan + Amlodipine (e.g., Telma AM) or Telmisartan + HCTZ (e.g., Telma H) — improves compliance.
Do NOT combine ARB + ACE inhibitor — this is dangerous due to risk of hyperkalemia and acute kidney injury. — Harrison's Principles of Internal Medicine 22E
Step 3 — Triple Therapy
If still uncontrolled on dual therapy:
ARB + CCB + Thiazide diuretic (all three together)
This is the recommended triple combination per European and US guidelines. — Comprehensive Clinical Nephrology, 7th Edition
Step 4 — Resistant Hypertension
If BP is uncontrolled on 3 drugs at optimal doses (including a diuretic):
- Add Spironolactone 25–50 mg once daily — most effective 4th agent
- Alternatively: α-blocker (e.g., doxazosin) or β-blocker (e.g., bisoprolol, especially if heart failure/angina/AF co-exist)
- Refer to a specialist for further workup
Special Considerations (in Women)
| Condition | Preferred addition |
|---|---|
| Diabetes | Keep ARB (renoprotective), add CCB or diuretic |
| CKD/Proteinuria | Maximize ARB dose first |
| Angina/Ischemia | Add CCB (amlodipine) |
| Heart failure | Add ACE inhibitor instead of ARB, plus beta-blocker |
| Pregnancy | ARB is contraindicated — switch to methyldopa, labetalol, or nifedipine |
Practical bottom line for most patients:
Telmisartan 80 mg → add Amlodipine 5–10 mg → add Chlorthalidone/HCTZ → add Spironolactone if still resistant.
Always rule out secondary hypertension (renal artery stenosis, primary aldosteronism, pheochromocytoma, thyroid disease) if response to multiple drugs is poor.
Is patient can leaves the all drugs
Finding Sources
Finding Sources
Finding Sources
Reading File
The short answer is: No, in most cases she cannot simply stop all drugs. Here is why:
Can a Hypertension Patient Stop All Medications?
The General Rule
"Most patients with hypertension require lifelong therapy." — Comprehensive Clinical Nephrology, 7th Edition
Hypertension is a chronic condition. The drugs control BP — they do not cure the underlying problem. Stopping them usually causes BP to rise again, sometimes to dangerously high levels.
When Stopping Drugs MAY Be Possible
Only in a very narrow group of patients — all conditions below must be met:
| Condition | Requirement |
|---|---|
| Mild hypertension only | Grade 1 (BP was mildly elevated, not severely high) |
| Major lifestyle changes made | Significant weight loss, strict salt restriction, regular exercise, quit smoking/alcohol |
| No target organ damage | No heart enlargement, no kidney damage, no previous stroke or heart attack |
| Low cardiovascular risk | Young, no diabetes, no family history of heart disease |
| On monotherapy only | Was on just one drug at a low dose |
Even in this group, stopping must be done gradually and under doctor supervision, not abruptly.
What Happens If She Stops Abruptly?
Stopping antihypertensives suddenly — especially when BP is already uncontrolled — is dangerous:
- BP will rebound — often higher than before
- Risk of stroke
- Risk of heart attack
- Risk of kidney damage
- Risk of hypertensive emergency (BP crisis)
What She SHOULD Do Instead
Since her BP is already uncontrolled on Telvas 40, stopping drugs is the wrong direction. The right approach:
- Never stop on her own — always consult her doctor first
- Optimize lifestyle (weight loss, low-salt diet, exercise, stress reduction) — this can reduce drug doses needed
- Work with the doctor to adjust or add medications until BP is controlled
- Continue regular BP monitoring at home
Bottom line: She cannot leave all drugs on her own. Doing so — especially with uncontrolled hypertension — puts her at serious risk of stroke, heart attack, and organ damage. Any changes to medication must only be made under medical supervision.
This is a shared conversation. Sign in to Orris to start your own chat.