Note on pre implantation techniques
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have comprehensive content. Let me compile the full structured note.
Pre-Implantation Techniques - Clinical Notes
Overview
Pre-implantation techniques encompass all procedures performed on embryos (and supporting assessments) prior to embryo transfer in the context of in vitro fertilization (IVF). The umbrella term Preimplantation Genetic Testing (PGT) has replaced the older "Preimplantation Genetic Diagnosis (PGD)" to more accurately reflect the range of testing indications.
1. The IVF Framework (Prerequisite)
All pre-implantation techniques require IVF:
- Ovarian stimulation - to retrieve approximately 10 or fewer oocytes per cycle
- In vitro fertilization of retrieved oocytes
- Embryo culture for 5-6 days until the blastocyst stage (day 5 or 6)
- Embryo biopsy, genetic analysis, then transfer (fresh or frozen-thaw cycle)
2. Biopsy Techniques - How Cells Are Sampled
A. Polar Body Biopsy
- Timing: At the oocyte stage, before or after fertilization (very early)
- Method: The first and/or second polar body is removed and analyzed; the genetic status of the oocyte is inferred indirectly
- Limitation: Crossing over during meiosis can cause erroneous diagnosis. Critically, it only reveals the maternal contribution - it cannot differentiate a carrier from an affected embryo for recessive disorders
B. Blastomere Biopsy (Day 3 / Cleavage Stage)
- Timing: Eight-cell stage (day 3 embryo)
- Method: One or two blastomeres are mechanically removed and analyzed by PCR
- Limitations:
- Only 1-2 cells available = very limited DNA
- Risk of allele dropout - preferential amplification of one allele over the other
- Sperm DNA contamination from zona pellucida can cause false-negatives
- High rate of mosaicism at cleavage stage means a single blastomere may not represent the whole embryo's karyotype (trisomic rescue means aneuploid cells at this stage may not persist)
- This method underperformed in a large multicenter RCT (2003-2007, n=408): PGT-A using FISH on cleavage-stage blastomeres gave a lower pregnancy rate (25% vs 37%) compared to standard IVF - Creasy & Resnik's Maternal-Fetal Medicine
C. Trophectoderm Biopsy (Blastocyst Stage - Current Standard)
- Timing: Day 5 or 6, at blastocyst stage
- Method: 5-10 cells are removed from the trophectoderm (which becomes the placenta) without disturbing the inner cell mass (ICM, which becomes the fetus)
- Advantages over blastomere biopsy:
- More DNA available (5-10 cells vs 1-2 cells) = greater diagnostic accuracy
- Less damaging to the embryo
- Less mosaicism overall at this stage compared to cleavage stage
- ICM is left entirely intact
- Limitation: Either rapid genetic testing within 24 hours is needed OR embryos must be cryopreserved for a frozen-thaw transfer (freeze-all strategy)
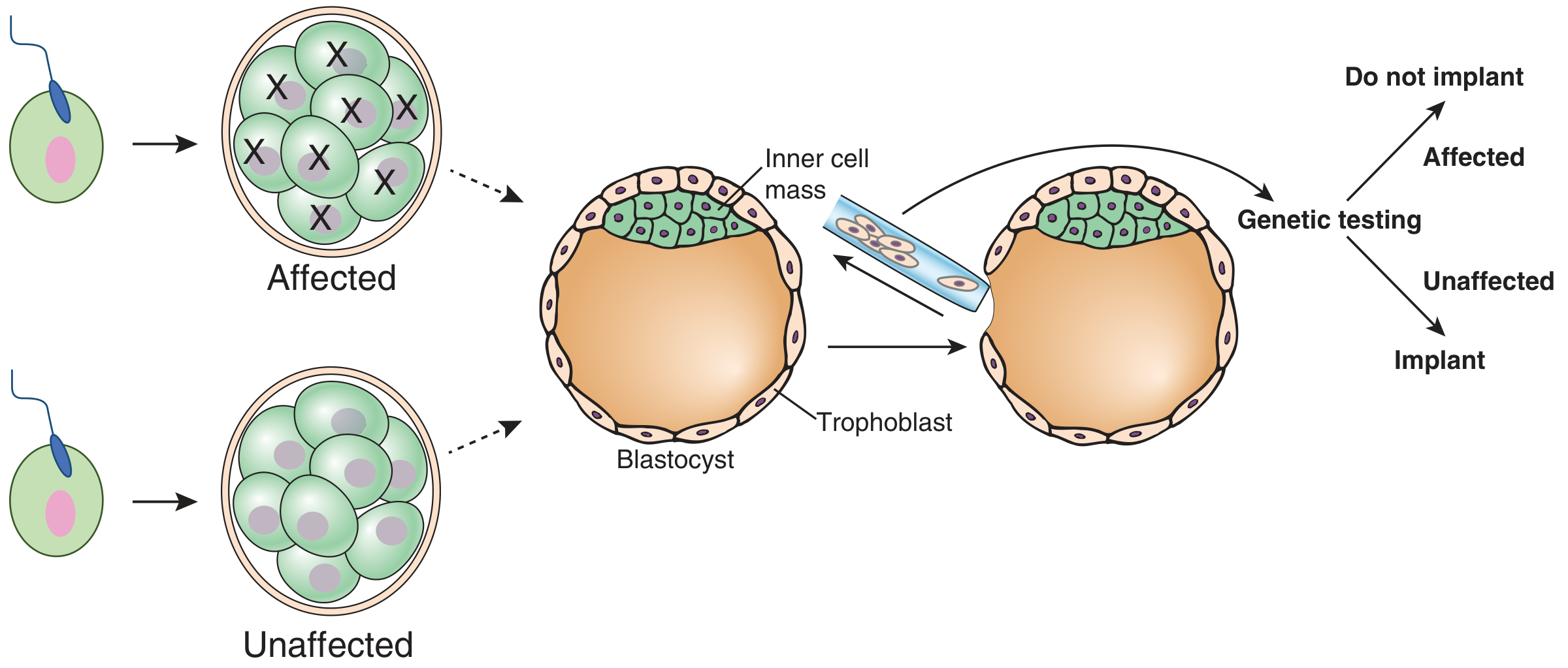
Figure: Preimplantation Genetic Testing - trophectoderm biopsy at blastocyst stage. Affected embryos (X) are not transferred; only unaffected (euploid) embryos are implanted. (Thompson & Thompson Genetics and Genomics in Medicine, 9th ed.)
3. The Three Types of PGT
| Type | Full Name | Target | Main Indication |
|---|---|---|---|
| PGT-A | PGT for Aneuploidy | Whole chromosome gain/loss | Improve IVF success rates, advanced maternal age, recurrent pregnancy loss |
| PGT-M | PGT for Monogenic conditions | Known pathogenic single-gene variants | Mendelian disease risk (e.g., CF, sickle cell, HD) |
| PGT-SR | PGT for Structural Rearrangements | Balanced/unbalanced chromosomal rearrangements (e.g., translocations) | Carrier parents with structural rearrangements |
4. PGT-A (Aneuploidy Testing)
Rationale
- Women >35 years have >30% aneuploid embryos; this rises to ~60% by age 40
- Selecting euploid embryos theoretically improves implantation and live birth rates
Evolution of Technology (Version 1.0 → 2.0)
- PGT-A 1.0: FISH probes on cleavage-stage blastomeres - tested only a limited set of chromosomes; no longer used due to poor clinical outcomes
- PGT-A 2.0 (current): Trophectoderm biopsy + genome-wide methods:
- Array CGH (comparative genomic hybridization) - previously the gold standard
- Quantitative PCR
- Massive Parallel Sequencing (Next Generation Sequencing / NGS) - now the most common; same principle as exome/genome sequencing; early evidence it may also detect clinically significant mosaicism
ASRM Position
The American Society of Reproductive Medicine (ASRM) recommends offering PGT-A to all infertile women undergoing IVF, though research to fully establish clinical utility is ongoing. - Thompson & Thompson Genetics, 9th ed.
Limitations of PGT-A
- Cannot detect subchromosomal deletions/duplications (only whole chromosome)
- Cannot detect whole chromosome mosaicism, triploidy, or single-gene disorders
- False-negative rate for microarray PGT-A: <1%
- False-positive/negative overall: ~2-3% - confirmatory prenatal testing (CVS or amniocentesis) still recommended
- Does not replace standard prenatal screening; cfDNA screening should still be offered
- The biopsy site (trophectoderm) may not perfectly represent the ICM karyotype
- Sources of error: sample mislabeling, DNA contamination, amplification failure, array noise, trophectoderm-ICM karyotype discordance
5. PGT-M (Monogenic Testing)
Indications: Known pathogenic variant in the family (e.g., autosomal dominant, autosomal recessive carrier couples, X-linked conditions, BRCA1/2, Huntington disease, fragile X, etc.)
Method:
- PCR amplification of the specific variant
- Analysis of linked polymorphic markers (STRs, SNPs) is included alongside direct variant detection to:
- Improve accuracy
- Detect allele dropout
- Minimize misdiagnosis from sperm contamination
- SNP microarrays after whole genome amplification (WGA) can overcome allele dropout
- Confirmatory CVS or amniocentesis is recommended after successful transfer because of the ~2-3% false result rate
Safety: No increased risk of birth defects or growth disorders in infants born after PGT-M compared to other ART-conceived infants. - Creasy & Resnik's Maternal-Fetal Medicine
6. PGT-SR (Structural Rearrangements)
- Used when one or both parents carry a balanced chromosomal translocation or other structural rearrangement
- Detects unbalanced rearrangements in embryos
- Uses the same NGS/array platforms as PGT-A; SNP arrays also allow detection of unbalanced translocations
- Prevents implantation of embryos with unbalanced chromosomal products, which often lead to miscarriage or affected offspring
7. Special Consideration - Mosaicism
- Mosaicism: Some cells in an embryo are euploid, others are aneuploid (due to mitotic errors during early development)
- A significant challenge because the trophectoderm biopsy sample may not represent the ICM
- Mosaic embryos can be considered potentially viable but are deprioritized for transfer compared to non-mosaic euploid embryos
- Prioritization for mosaic embryo transfer:
- Single mosaic chromosome involvement > two or more chromosomes
- Lower degree of aneuploidy (fewer affected cells) is preferred over higher degree
- Approximately 100 documented live births after mosaic embryo transfer with no significant adverse events reported (as of available data) - Creasy & Resnik
8. Genetic Technologies Used in PGT
| Technology | What it Detects | Used In |
|---|---|---|
| FISH (fluorescence in situ hybridization) | Limited set of chromosomes only | Historical PGT-A v1.0 - no longer preferred |
| Microarray / Array CGH | All chromosomes - copy number variations (CNVs) | PGT-A, PGT-SR (was gold standard) |
| SNP microarray | CNVs + allele information; can detect mosaicism, UPD | PGT-A, PGT-SR, PGT-M |
| NGS / Massive Parallel Sequencing | Whole genome CNV; potentially mosaicism; low-pass sequencing | PGT-A v2.0 (now standard), PGT-SR |
| PCR + STR/SNP linkage | Single-gene mutations with linked markers | PGT-M |
9. Summary of Biopsy Methods Comparison
| Feature | Polar Body | Blastomere (Day 3) | Trophectoderm (Day 5-6) |
|---|---|---|---|
| Stage | Pre-fertilization / zygote | 8-cell cleavage | Blastocyst |
| Cells sampled | 1-2 polar bodies | 1-2 cells | 5-10 cells |
| DNA quantity | Low | Very low | Adequate |
| Damage to embryo | Minimal | Moderate | Minimal |
| Mosaicism concern | N/A | High | Lower |
| Currently preferred | No | No | Yes |
| ICM preserved | Yes | Yes | Yes |
10. Clinical Indications for PGT
- Advanced maternal age (>35 years) - PGT-A
- Recurrent pregnancy loss (RPL) - PGT-A
- Repeated IVF implantation failure - PGT-A
- Known carrier of Mendelian disorder (CF, SMA, sickle cell, thalassemia, BRCA, etc.) - PGT-M
- Carrier of chromosomal translocation or inversion - PGT-SR
- Sex-linked disorders (X-linked recessive conditions) - PGT-M or sex selection
- Neuropsychiatric disorders: Fragile X, Huntington disease, Alzheimer disease risk - PGT-M (Kaplan & Sadock's Comprehensive Textbook of Psychiatry)
- Mitochondrial DNA disorders (selective cases)
Sources:
- Creasy & Resnik's Maternal-Fetal Medicine: Principles and Practice, blocks covering PGT sections
- Thompson & Thompson Genetics and Genomics in Medicine, 9th ed.
- Berek & Novak's Gynecology
- Emery's Elements of Medical Genetics and Genomics
This is a shared conversation. Sign in to Orris to start your own chat.