Clinical anatomy and physiology of the larynx
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching Images
larynx anatomy diagram cartilages muscles
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from Gray's Anatomy for Students and Cummings Otolaryngology. Let me compile a thorough, well-structured response.
Clinical Anatomy and Physiology of the Larynx
Overview
The larynx is a hollow musculoligamentous structure with a cartilaginous framework that caps the lower respiratory tract. It serves two principal functions: (1) a sphincteric valve protecting the lower airway, and (2) a sound-producing instrument for phonation. It is continuous inferiorly with the trachea and opens superiorly into the pharynx posterior to the tongue root.
It is suspended from the hyoid bone above and anchored to the trachea below, remaining highly mobile in the neck — moving dramatically upward and forward during swallowing to facilitate airway closure and esophageal opening.
Motor and sensory innervation is entirely via the vagus nerve [X].
— Gray's Anatomy for Students, p. 1192
Embryology (Clinically Relevant)
The larynx has a dual embryologic origin that directly governs patterns of cancer spread and lymphatic drainage:
| Region | Embryologic Origin | Blood & Lymph Supply |
|---|---|---|
| Supraglottis | Buccopharyngeal primordium (3rd & 4th branchial arches) | Superior laryngeal artery → bilateral deep cervical nodes (Levels II–III) |
| Glottis & Subglottis | Tracheobronchial primordium (6th branchial arch) | Inferior laryngeal artery → pretracheal/prelaryngeal nodes (Level VI) → Level IV |
Because the supraglottis forms without midline union, its lymphatics drain bilaterally — explaining the higher rate of bilateral nodal metastases in supraglottic carcinoma. The glottis forms by fusion of paired lateral structures; its sparse, unilateral lymphatics explain the low nodal metastasis rate of glottic squamous cell carcinoma.
— Cummings Otolaryngology, p. 1979
Cartilaginous Framework
Nine cartilages form the laryngeal skeleton: three large unpaired and three paired smaller ones.
Unpaired Cartilages
1. Cricoid Cartilage
- The most inferior laryngeal cartilage and the only complete cartilaginous ring in the airway
- Shaped like a signet ring: broad posterior lamina + narrow anterior arch
- Sits at the level of C6
- Provides articular facets for the arytenoid cartilages (on the superolateral lamina) and the inferior horns of the thyroid cartilage (lateral lamina)
- The posterior lamina bears two oval depressions (for posterior cricoarytenoid muscles) separated by a vertical ridge (esophageal attachment)
2. Thyroid Cartilage
- The largest laryngeal cartilage; supports most laryngeal soft tissues
- Two laminae fuse anteriorly to form the laryngeal prominence (Adam's apple) — more pronounced in males due to testosterone-driven growth
- The superior thyroid notch is a key landmark for percutaneous airway techniques and laryngeal nerve blocks
- Superior and inferior horns (cornua): inferior horns articulate with the cricoid at the cricothyroid joint
- The cricothyroid membrane (CTM) spans the gap between the thyroid and cricoid anteriorly — the target for emergency cricothyrotomy
3. Epiglottis
- A leaf-shaped fibroelastic cartilage that forms the anterior border of the laryngeal inlet
- Anterior surface attached to the hyoid bone via the hyoepiglottic ligament and to the thyroid cartilage via the thyroepiglottic ligament
- Deflects food bolus away from the airway during swallowing (though this function is not essential for aspiration prevention)
- The vallecula is the space between the base of tongue and the anterior epiglottis — the target for placement of a Macintosh laryngoscope blade
Paired Cartilages
Arytenoid cartilages — pyramid-shaped; articulate with the superolateral cricoid lamina. Each has:
- Vocal process (anterior): attachment of the vocal ligament
- Muscular process (lateral): attachment of the intrinsic muscles that rotate and glide the arytenoid
Corniculate cartilages — tiny, sit atop the arytenoids; form the corniculate tubercles visible at the posterior laryngeal inlet
Cuneiform cartilages — wedge-shaped; lie within the aryepiglottic folds
— Miller's Anesthesia 10e, p. 5841–5842; Gray's Anatomy for Students, p. 1192
Joints and Ligaments
Cricothyroid joints (synovial): Between the inferior horns of the thyroid cartilage and the lateral cricoid. Allow rotation of the thyroid cartilage forward/downward → increases the AP diameter of the glottis → tenses the vocal folds (key for pitch regulation).
Cricoarytenoid joints (synovial): Between the base of each arytenoid and the superolateral cricoid lamina. Allow rotation (abduction/adduction of vocal folds) and gliding (separation/approximation of arytenoids).
Key membranes and ligaments:
- Thyrohyoid membrane: connects the thyroid cartilage to the hyoid bone; pierced by the internal branch of the superior laryngeal nerve and superior laryngeal vessels
- Cricothyroid membrane: connects thyroid to cricoid anteriorly — clinically vital for emergency airways
- Conus elasticus (cricovocal membrane): extends from the superior surface of the cricoid arch upward, thickening medially to form the vocal ligament — the free upper edge of the membrane
- Quadrangular membrane: extends from the lateral epiglottis to the arytenoid; its free lower edge is the vestibular ligament (false cord)
Laryngeal Cavity: Three Compartments
Two pairs of mucosal folds divide the laryngeal cavity:
SUPRAGLOTTIS (Vestibule)
─ Laryngeal inlet
─ Aryepiglottic folds
─ False vocal cords (vestibular folds) ─ contain vestibular ligaments
↕ Laryngeal ventricles + saccules
GLOTTIS
─ True vocal cords (vocal folds) ─ contain vocal ligaments + vocalis muscle
─ Rima glottidis
↕ narrowest part of adult larynx (wider in children — subglottis is narrowest)
SUBGLOTTIS (Infraglottic cavity)
─ Inferior border of vocal folds → inferior border of cricoid
Rima glottidis — the triangular slit between the two vocal folds; its anterior tip is fixed at the thyroid angle, its posterior extent formed by the interarytenoid fold. It is the narrowest point of the adult airway.
Laryngeal ventricles — lateral outpouchings between false and true cords; each has an anterosuperior extension (saccule) with mucous glands that lubricate the vocal folds.
— Gray's Anatomy for Students, p. 1199
Intrinsic Muscles
All intrinsic muscles except the cricothyroid are innervated by the recurrent laryngeal nerve (RLN). The cricothyroid is innervated by the external branch of the superior laryngeal nerve (eSLN).
| Muscle | Action | Innervation |
|---|---|---|
| Posterior cricoarytenoid (PCA) | Abducts vocal folds (opens glottis) — only abductor | RLN |
| Lateral cricoarytenoid (LCA) | Adducts vocal folds (closes glottis) | RLN |
| Transverse arytenoid | Adducts arytenoids | RLN |
| Oblique arytenoid | Sphincter of laryngeal inlet | RLN |
| Thyroarytenoid | Shortens/relaxes vocal fold; sphincter of vestibule | RLN |
| Vocalis | Fine tension adjustment of vocal ligament | RLN |
| Cricothyroid | Rotates thyroid cartilage forward → tenses (lengthens) vocal fold → raises pitch | eSLN |
The posterior cricoarytenoid is the only abductor of the vocal folds. Bilateral RLN palsy paralyzes all intrinsic muscles except the cricothyroid, leaving the cords in a median/paramedian position with the glottis closed — causing inspiratory stridor and potential asphyxia.
— Gray's Anatomy for Students, p. 1201
Extrinsic Muscles
Elevators (suprahyoid group and stylopharyngeus): pull larynx upward and forward during swallowing.
Depressors (infrahyoid/strap muscles: sternothyroid, sternohyoid, thyrohyoid): return larynx to resting position after swallowing.
Innervation
Both branches of the vagus nerve [X] supply the larynx:
Superior laryngeal nerve (SLN) — branches near the inferior ganglion of vagus:
- Internal branch (iSLN): sensory to the laryngeal mucosa above the vocal folds; pierces the thyrohyoid membrane with the superior laryngeal artery; mediates the cough and laryngospasm reflexes from supraglottic stimulation
- External branch (eSLN): motor to the cricothyroid muscle only; at risk during thyroid surgery
Recurrent laryngeal nerve (RLN):
- Motor to all intrinsic laryngeal muscles except cricothyroid
- Sensory to mucosa below the vocal folds
- Ascends in the tracheoesophageal groove; enters the larynx deep to the inferior pharyngeal constrictor
- Left RLN has a longer course (loops around the aortic arch) → more vulnerable to mediastinal pathology
- At risk in thyroid/parathyroid surgery, neck dissection, and thoracic procedures
Clinical correlates:
- Unilateral RLN palsy → hoarse, breathy voice (paralyzed cord in paramedian position)
- Bilateral RLN palsy → airway obstruction, stridor
- eSLN palsy → loss of high-pitch phonation (cricothyroid paralysis)
Blood Supply
| Artery | Origin | Territory |
|---|---|---|
| Superior laryngeal artery | Superior thyroid artery (from external carotid) | Supraglottis and glottis; enters via thyrohyoid membrane with iSLN |
| Inferior laryngeal artery | Inferior thyroid artery (from thyrocervical trunk) | Subglottis; enters with RLN deep to inferior constrictor |
Veins: Superior laryngeal veins → superior thyroid veins → internal jugular vein. Inferior laryngeal veins → inferior thyroid veins → left brachiocephalic vein.
Lymphatic Drainage
| Level | Drains | Destination |
|---|---|---|
| Above vocal folds (supraglottis) | Via superior laryngeal artery; bilateral drainage | Deep cervical nodes at common carotid bifurcation (Levels II–III) |
| Below vocal folds (subglottis) | Via inferior thyroid artery | Pretracheal/prelaryngeal nodes (Level VI) → Level IV |
| Vocal folds (glottis) | Sparse lymphatics, unilateral | Low metastatic risk |
— Gray's Anatomy for Students, p. 1205–1206; Cummings Otolaryngology, p. 1979
Physiology
1. Airway Protection
The larynx has three levels of sphincteric closure, activated sequentially during swallowing:
- Aryepiglottic folds (oblique arytenoids)
- False vocal folds (thyroarytenoid + quadrangular membrane)
- True vocal folds (lateral cricoarytenoids + transverse arytenoids)
Simultaneously, the larynx elevates and tilts posteriorly under the tongue base; the epiglottis is passively deflected posteriorly by the tongue to seal the inlet.
2. Phonation
- The vocal folds (vocalis muscle + vocal ligament + overlying mucosa) vibrate due to aerodynamic forces — the Bernoulli effect draws adducted folds together as air passes between them
- Pitch (fundamental frequency): determined by length and tension of vocal folds
- Cricothyroid elongates/tenses folds → higher pitch
- Vocalis shortens/slackens folds → lower pitch
- Males: vocal folds ~17–23 mm; pitch ~110 Hz
- Females: vocal folds ~12–17 mm; pitch ~220 Hz
- Testosterone increases vocal fold mass and length → lower pitch (relevant in transgender men on HRT)
- Loudness: determined by subglottic air pressure
- Quality/timbre: shaped by resonating chambers (pharynx, oral cavity, nasal cavity)
3. Cough Reflex
- Afferent: iSLN (above cords) and RLN (below cords) → vagus → nucleus tractus solitarius
- Deep inspiration → tight glottic closure (adduction) → buildup of intrathoracic pressure → sudden explosive glottic opening → airflow >12 L/s clears the airway
4. Valsalva Maneuver
Sustained glottic closure against forced expiration — raises intrathoracic/intraabdominal pressure; important in defecation, parturition, and weight-lifting.
5. Fixation of the Thorax
Glottic closure fixes the chest wall for upper limb exertion.
Anatomical Diagrams
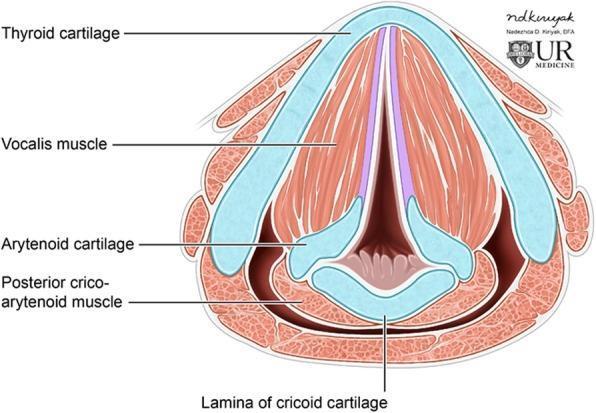
Axial cross-section at the glottis: thyroid cartilage (anterior V), cricoid lamina (posterior), arytenoids, vocal folds, vocalis muscle, and posterior cricoarytenoid muscle.
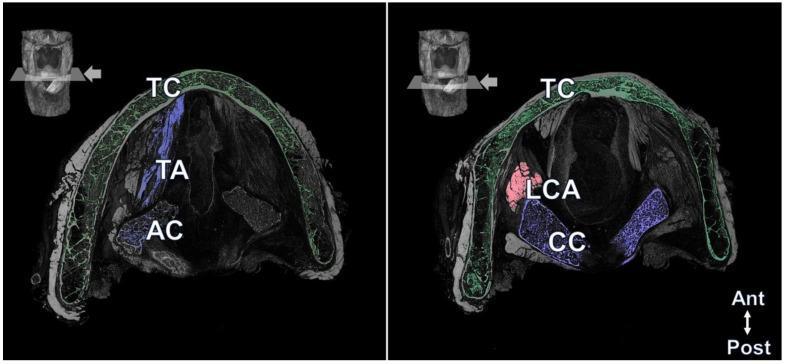
Cross-sections comparing superior level (thyroid cartilage + thyroarytenoid muscle) and inferior level (cricoid cartilage + lateral cricoarytenoid muscle).
Key Clinical Correlations
| Scenario | Anatomical Basis |
|---|---|
| Emergency cricothyrotomy | CTM is the avascular anterior space between thyroid and cricoid cartilages |
| Thyroid surgery RLN injury | RLN runs in the tracheoesophageal groove; vulnerable during inferior thyroid artery ligation |
| eSLN injury (thyroid surgery) | Loss of cricothyroid function → voice fatigue, cannot reach high pitches |
| Subglottic stenosis in children | Subglottis is the narrowest airway segment in children (vs. glottis in adults) |
| Supraglottic laryngeal cancer | Bilateral lymph node spread (embryologically no midline fusion) |
| Glottic cancer | Rarely spreads to nodes early (sparse glottic lymphatics) |
| Bilateral RLN palsy | Cords adducted → inspiratory stridor → emergency airway |
| Laryngospasm | Sustained glottic closure triggered by secretions/stimulation of iSLN afferents |
Sources: Gray's Anatomy for Students, pp. 1192–1206 | Cummings Otolaryngology Head and Neck Surgery, pp. 1979–1980 | Miller's Anesthesia 10e, pp. 5841–5844
Acute and chronic tonsillitis, Classification. Etiology. pathogenesis, symptoms, diagnostics, treatment, differential diagnosis, complications, prevention
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from multiple authoritative sources. Let me compile the full structured answer.
Acute and Chronic Tonsillitis
Anatomy — Brief Review
The palatine tonsils reside in the tonsillar fossa on the lateral walls of the oropharynx, between the palatoglossal (anterior pillar) and palatopharyngeal (posterior pillar) arches. Their blood supply is principally from the tonsillar artery (branch of the facial artery), with contributions from the ascending pharyngeal, lingual, ascending palatine, and greater palatine arteries. Venous drainage flows through tonsillar venae comitantes into the pharyngeal venous plexus. The external palatine (paratonsillar) vein, lying between the tonsil and the superior constrictor muscle, is the key vessel injured in tonsillectomy hemorrhage.
The tonsil surface is covered in stratified squamous epithelium that invaginates to form crypts — these are the nidus of infection in both acute and chronic disease.
— Gray's Anatomy for Students, p. 1296
Classification
I. Acute Tonsillitis
- Viral (majority of cases)
- Bacterial
- Membranous (e.g., diphtheria, EBV with pseudomembrane)
II. Chronic Tonsillitis
- Recurrent acute tonsillitis — repeated discrete episodes with full recovery between attacks
- Chronic follicular/crypt tonsillitis — deep crypts with retained debris (tonsilloliths), chronic bacterial colonisation, persistent symptoms
- Chronic hypertrophic tonsillitis — enlarged tonsils causing obstructive symptoms (OSA, dysphagia)
Etiology
Acute Tonsillitis
Viral causes (predominant):
- Adenovirus, rhinovirus, echovirus, coxsackievirus, RSV, influenza, parainfluenza
- Epstein-Barr virus (EBV, HHV-4) — causes infectious mononucleosis; the most important viral cause to distinguish clinically
Bacterial causes:
- Group A β-hemolytic Streptococcus (GABHS / S. pyogenes) — most common bacterial pathogen; peak incidence ages 5–6 years
- Haemophilus influenzae, Streptococcus pneumoniae, Staphylococcus aureus
- Diphtheria (Corynebacterium diphtheriae) — in unimmunized populations
- Mixed anaerobes — particularly in peritonsillar abscess
- Mycobacterium tuberculosis — rare, in immunocompromised patients
Chronic Tonsillitis
- Polymicrobial including anaerobes; Actinomyces species is a key organism — its presence in crypt debris indicates established chronic infection that is unlikely to resolve with antibiotics alone
- Biofilm formation within tonsillar crypts
- Predisposing factors: recurrent acute episodes, smoking, poor dental hygiene, gastroesophageal/laryngopharyngeal reflux, chronic mouth breathing
— K.J. Lee's Essential Otolaryngology; Goldman-Cecil Medicine
Pathogenesis
Acute Tonsillitis
The palatine tonsils are part of Waldeyer's ring — the pharyngeal lymphoid tissue that forms the first immunological barrier to inhaled and ingested antigens. In acute infection:
- Viral or bacterial pathogens colonise the tonsillar crypts
- Acute inflammatory response: mucosal invasion → neutrophil infiltration → oedema, hyperaemia, and crypt exudate
- GABHS produces multiple virulence factors: streptolysins (O and S), erythrogenic toxin (causing the rash of scarlet fever), streptokinase, hyaluronidase, and M-protein (antiphagocytic), enabling tissue invasion and immune evasion
- M-protein shares structural similarity with cardiac sarcomeric proteins → molecular mimicry → rheumatic fever if untreated
- Streptococcal antigens activate complement and form immune complexes → post-streptococcal glomerulonephritis
Chronic Tonsillitis
- Deep tonsillar crypts accumulate desquamated epithelial cells, food debris, and bacteria
- This provides an anaerobic microenvironment ideal for bacterial persistence and biofilm formation
- Repeated cycles of subclinical infection → progressive scarring and fibrosis of tonsillar tissue
- Crypts widen and become obstructed → tonsilloliths (calcified debris) → halitosis, foreign body sensation
- Persistent antigen stimulation → reactive cervical lymphadenopathy
— Goldman-Cecil Medicine; Cummings Otolaryngology
Clinical Features
Acute Viral Tonsillitis
- Gradual onset of sore throat, low-grade or no fever
- Pharyngeal erythema without exudate
- Rhinorrhoea, nasal congestion, hoarseness, oral ulcers (features suggesting viral aetiology)
- Mild to moderate sore throat severity
Acute Bacterial (GABHS) Tonsillitis
- Sudden onset fever, severe sore throat, odynophagia
- Associated: malaise, dysphagia, otalgia, headache, nausea, abdominal pain
- Physical findings:
- Oropharyngeal erythema with tonsillar enlargement ± creamy/yellow exudate
- Palatal petechiae
- Swollen uvula
- Tender anterior cervical lymphadenopathy
- Scarlatiniform rash (in scarlet fever) — descending erythematous rash from neck to trunk, fading in ~1 week
- Strawberry tongue (enlarged papillae ± white membrane)
EBV Infectious Mononucleosis (key differential)
- High fever, severe malaise, headache
- Severe pharyngitis ± green/gray tonsillar exudate (indistinguishable from streptococcal on exam)
- Palatal petechiae at the hard-soft palate junction
- Large, tender cervical lymphadenopathy (may be bilateral)
- Hepatosplenomegaly
- Characteristic rash developing after amoxicillin/ampicillin exposure (morbilliform, mainly truncal)
- Risk of upper airway obstruction (tonsillar hypertrophy + oedema)
- Rare: splenic rupture, haematologic/neurologic/cardiac complications
Chronic Tonsillitis
- Recurrent sore throats, persistent low-grade throat discomfort
- Halitosis (foul odour from crypt debris)
- Tonsilloliths — white/yellow semisolid debris extruding from crypts; foul taste
- Foreign body sensation in the throat
- Chronic cough, irritability
- Tonsillar asymmetry (may suggest malignancy — requires evaluation)
- Recurrent febrile episodes
PFAPA Syndrome (Periodic Fever, Aphthous stomatitis, Pharyngitis, Cervical Adenitis):
- Each episode lasts ~3 days
- ≥3 episodes recurring every ~3 weeks
- Symptom-free intervals
- Must exclude cyclical neutropenia
— Cummings Otolaryngology, p. 3795–3796; K.J. Lee's Essential Otolaryngology
Diagnostics
Clinical Scoring — Centor/McIsaac Score for GABHS
| Criterion | Points |
|---|---|
| Tonsillar exudate | +1 |
| Tender anterior cervical lymph nodes | +1 |
| Fever >38°C | +1 |
| Absence of cough | +1 |
| Age 3–14 years | +1 |
Score ≥3: test or treat; Score 0–1: no test or antibiotics needed.
Laboratory Investigations
Rapid Antigen Detection Test (RADT)
- Detects GABHS group-A carbohydrate antigen
- Highly specific; if negative, confirm with throat culture (gold standard for GABHS)
- Culture on blood agar; ASO titres not recommended for diagnosis — they only indicate prior infection, not active disease
Complete Blood Count (CBC)
- Bacterial: leukocytosis with neutrophilia
- EBV: lymphocytosis (>50% lymphocytes), >10% atypical lymphocytes; ESR more likely elevated in EBV than bacterial infection
Heterophile Antibody Test (Monospot)
- Sensitivity: 85% overall; less sensitive in the first two weeks; 100% specific
- Repeat weekly for 6 weeks if initial negative and EBV suspected
- Commercial tests: sensitivity 81–95%, positive predictive value >95%
EBV-specific serology (if monospot negative after 6 weeks):
- IgM anti-VCA: acute infection
- IgG anti-VCA + IgG anti-EBNA: past infection
- PCR for EBV DNA: used in suspected EBV encephalitis
Diphtheria: Culture on tellurite media — in unimmunized patients with thick pharyngeal membrane
Throat culture: For GABHS confirmation when RADT negative; remains the gold standard
— Cummings Otolaryngology, p. 3796; K.J. Lee's Essential Otolaryngology
Differential Diagnosis
| Condition | Distinguishing Features |
|---|---|
| Viral pharyngitis | Slow onset, low/no fever, rhinorrhoea, hoarseness, no exudate |
| GABHS tonsillitis | Rapid onset, high fever, exudate, petechiae, tender nodes, no cough |
| EBV mononucleosis | Atypical lymphocytes, monospot +ve, splenomegaly, rash with ampicillin |
| Diphtheria | Thick adherent pharyngeal grey membrane, unimmunized, severe toxicity, bull-neck lymphadenopathy |
| Herpangina (Coxsackie A) | Vesicles/ulcers on anterior tonsillar pillars and soft palate |
| Vincent angina | Unilateral ulcerative tonsillitis, mixed fusospirochaetal anaerobes, fetor oris |
| Peritonsillar abscess | Trismus, unilateral palatal bulge, uvular deviation, "hot potato" voice |
| Ludwig angina | Floor-of-mouth induration, submandibular swelling, airway emergency |
| Epiglottitis | "Hot potato" voice, severe odynophagia, anterior neck tenderness, drooling, "thumb sign" on lateral neck X-ray |
| Retropharyngeal abscess | Children <6 yrs, neck rigidity, dysphagia, widened prevertebral shadow on lateral neck X-ray |
| Tonsillar lymphoma | Unilateral painless tonsillar enlargement, B symptoms, no acute infection |
| Agranulocytosis | Tonsillar ulceration/necrosis, absent fever response, drug history |
Treatment
Acute Viral Tonsillitis
- Supportive care: analgesia (NSAIDs preferred — ibuprofen), hydration, rest
- Antibiotics not indicated
- EBV mononucleosis: NSAIDs for pain; avoid β-lactams (amoxicillin/ampicillin → morbilliform rash in ~30%); oral/parenteral corticosteroids for moderate-to-severe tonsillopharyngitis and mild airway obstruction
- Severe airway obstruction: nasopharyngeal airway; rarely tonsillectomy, intubation, or tracheotomy
Acute Bacterial (GABHS) Tonsillitis
First-line:
- Penicillin V (oral, 10 days) or amoxicillin — drug of choice; targets GABHS to prevent rheumatic fever
- Full 10-day course is essential to eradicate GABHS and prevent complications
Penicillin allergy:
- Azithromycin (5 days) or clarithromycin
- Clindamycin (for recurrent/penicillin-tolerant strains)
- Cephalosporins if allergy is not anaphylactic
Adjuncts:
- NSAIDs/paracetamol for analgesia and antipyresis
- Single dose of dexamethasone — reduces symptom severity and duration in severe cases
Chronic Tonsillitis
Medical:
- Frequent gargling with hydrogen peroxide mouthwash
- Manual expression of tonsillar debris
- Prolonged antibiotics: amoxicillin 500 mg TDS × 21 days, or clindamycin 300 mg TDS × 21 days
- Note: Presence of Actinomyces indicates long-term antibiotics will likely fail → surgery required
Surgical — Tonsillectomy Indications (Paradise Criteria):
- ≥7 episodes in 1 year
- ≥5 episodes per year for 2 consecutive years
- ≥3 episodes per year for 3 consecutive years
-
2 weeks of school/work lost per year
- Peritonsillar abscess (on same side)
- Tonsillar hypertrophy causing upper airway obstruction (OSA) or swallowing difficulty
- Recurrent tonsillitis causing febrile seizures
- Suspicion of malignancy (unilateral enlargement; unknown primary)
- Diphtheria carrier state
- PFAPA unresponsive to medical treatment
Tonsillectomy morbidity:
- Post-operative haemorrhage: 2–4% (primary within 24 h; secondary at days 5–10)
- Mortality: ~1 in 25,000 (haemorrhage, airway obstruction, anaesthesia)
— K.J. Lee's Essential Otolaryngology, p. 686; Goldman-Cecil Medicine; Cummings Otolaryngology
Complications
Local/Regional Complications
| Complication | Key Features |
|---|---|
| Peritonsillar abscess (Quinsy) | Most common complication; pus in Weber glands potential space between tonsil capsule and superior constrictor; trismus (best indicator), uvular deviation to contralateral side, "hot potato" voice, odynophagia; Tx: needle aspiration or I&D + antibiotics |
| Parapharyngeal abscess | Extension through superior constrictor; swelling of lateral neck, trismus, medial displacement of lateral pharyngeal wall |
| Retropharyngeal abscess | Posterior extension; posterior pharyngeal wall bulge, neck stiffness, dysphagia, airway risk |
| Lemierre syndrome | Internal jugular vein thrombophlebitis (Fusobacterium necrophorum); septic emboli to lungs |
| Mediastinitis | Deep cervical space infection tracking inferiorly; life-threatening |
| Tonsillar hypertrophy/OSA | Chronic hypertrophy → obstructive sleep apnoea, cor pulmonale |
| Tonsillolith | Calcified crypt debris → halitosis, foreign body sensation, cough |
| Quincke disease | Uvular oedema in association with acute bacterial tonsillitis; can cause airway embarrassment |
Systemic (Non-Suppurative) Complications of GABHS
| Complication | Mechanism | Onset |
|---|---|---|
| Acute Rheumatic Fever (ARF) | Molecular mimicry: M-protein antibodies cross-react with cardiac sarcomeric proteins (myosin, tropomyosin) → pancarditis, polyarthritis, Sydenham chorea, erythema marginatum, subcutaneous nodules | 2–4 weeks post-infection |
| Post-streptococcal Glomerulonephritis (PSGN) | Immune complex deposition in glomeruli → complement activation → nephritis | 1–3 weeks post-pharyngitis; 3–6 weeks post-skin infection |
| PANDAS | Paediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infection; OCD, tics | |
| Scarlet fever | Erythrogenic (pyrogenic) exotoxin A, B, C from lysogenic strains; rash + strawberry tongue | During acute pharyngitis |
Critical point: Antibiotic treatment of GABHS pharyngitis prevents rheumatic fever but does not reliably prevent PSGN.
— Cummings Otolaryngology; K.J. Lee's Essential Otolaryngology, p. 606
Prevention
Primary Prevention
- Prompt treatment of GABHS tonsillitis with a full 10-day course of penicillin (eradicates GABHS, preventing ARF)
- Avoiding close contact during acute illness (droplet precautions)
- Hand hygiene; avoid sharing utensils
- Vaccination: diphtheria toxoid (DPT/Td) — prevents membranous tonsillitis
- H. influenzae type b (Hib) vaccination — prevents epiglottitis, reduces one complication pathway
- Smoking cessation (reduces chronic tonsillar irritation)
- Treatment of gastro-oesophageal/laryngopharyngeal reflux
Secondary Prevention
- Benzathine penicillin G IM monthly (for patients with documented rheumatic fever or ARF risk) — long-term secondary prophylaxis to prevent recurrent GABHS and further cardiac damage
- Duration: at least 5 years after last episode or until age 21 (longer if carditis present)
Tertiary Prevention
- Tonsillectomy in patients meeting criteria — removes the nidus of recurrent infection
Summary Table: Acute vs. Chronic Tonsillitis
| Feature | Acute Tonsillitis | Chronic Tonsillitis |
|---|---|---|
| Onset | Sudden | Insidious/recurrent |
| Predominant pathogen | Viral (majority); GABHS (bacterial) | Mixed anaerobes, Actinomyces |
| Main symptom | Severe sore throat, fever | Halitosis, mild chronic throat discomfort, tonsilloliths |
| Tonsillar appearance | Erythematous ± exudate | Scarred, irregular crypts, debris-laden |
| Fever | Prominent (bacterial) | Low-grade or absent |
| Lymphadenopathy | Tender anterior cervical nodes | Chronic, less tender |
| Diagnostics | RADT, throat culture, monospot | Clinical; Actinomyces on culture/histology |
| Treatment | Penicillin/amoxicillin (bacterial); supportive (viral) | Prolonged antibiotics; tonsillectomy |
| Key complication | Peritonsillar abscess, ARF, PSGN | OSA, tonsillolith, malignancy concern |
Sources: Cummings Otolaryngology Head and Neck Surgery, pp. 3794–3800 | K.J. Lee's Essential Otolaryngology, pp. 592, 686, 1022 | Goldman-Cecil Medicine, p. 3849 | Gray's Anatomy for Students, p. 1296
This is a shared conversation. Sign in to Orris to start your own chat.