Refraction surgery from opthalmology books
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from both books. Let me compile the full response.
Refractive Surgery
Based on Kanski's Clinical Ophthalmology (10th ed.) and The Wills Eye Manual
1. Introduction
Refractive surgery encompasses procedures aimed at changing the refraction of the eye by altering the cornea or lens - the principal refracting components. Myopia, hypermetropia, and astigmatism can all be addressed, though consistent correction of presbyopia remains elusive.
The basic principle of corneal refractive surgery is to induce a change in corneal curvature to correct a pre-existing refractive error. The patient population consists of people with stable refractive error who desire improved uncorrected vision.
2. Preoperative Assessment & Patient Selection
A thorough preoperative assessment is mandatory. Not all candidates are suitable.
Contraindications:
- Unacceptably high expectations
- Dry eye syndrome
- Non-stable refractive error
- Systemic disease: SLE, rheumatoid arthritis, immunocompromise
- Ocular disease: chronic blepharitis, previous herpes simplex, glaucoma, macular degeneration
Special counselling is required for those needing high-quality vision due to occupation or hobbies (pilots, air traffic controllers, truck drivers, contact sport athletes, marksmen). Common adverse effects to discuss include under/over-correction, dry eye, and eventual presbyopia.
Preoperative workup for LASIK specifically:
- Complete ocular examination
- Tear film osmolarity (to exclude dry eye)
- Corneal pachymetry (for residual stromal bed thickness; exclude mild keratoconus)
- Corneal topography (to exclude irregular astigmatism, keratoconus, forme fruste keratoconus)
- Corneal OCT (epithelial map)
- Corneal and whole-eye wavefront aberrometry
- Contact lens wearers: discontinue soft lenses for 2 weeks, hard/RGP lenses for at least 3 weeks before definitive keratometry
3. Categories of Refractive Procedures
3A. Laser Corneal Procedures
LASIK (Laser In Situ Keratomileusis)
The most common refractive procedure. An excimer laser ablates corneal stroma exposed by a superficial flap (created by a microkeratome or femtosecond laser). The flap remains attached by a hinge.
- Myopia correction: Central ablative flattening
- Hypermetropia correction: Mid-peripheral ablation (steepens centre)
Range: Hypermetropia up to 3-4 D, astigmatism up to 5 D, myopia up to 6-8 D (limited by corneal thickness). A residual stromal bed of at least 250 μm must remain to prevent ectasia.
Advantages over surface ablation:
- Greater postoperative comfort
- Faster visual rehabilitation
- More rapid refraction stabilization
- Milder stromal haze
Major disadvantage: Potential for flap-related complications.
PRK (Photorefractive Keratectomy) - Surface Ablation
Excimer laser ablates corneal stroma after epithelial removal (no flap). Epithelium removed by blade, spatula, brush, excimer laser, or dilute alcohol.
- Corrects myopia up to 6 D, astigmatism up to ~3 D, low-moderate hypermetropia
- Preferred in patients at higher risk of eye trauma (no flap to dislocate)
- Suitable for thin corneas
- Depth of stromal exposure: Bowman membrane
Disadvantages vs LASIK: Lower degrees correctable; slower healing; unpredictable postoperative discomfort; more subepithelial haze.
LASEK (Laser Subepithelial Keratomileusis)
Epithelium is chemically separated from Bowman layer using 20% absolute alcohol confined by a marker well, pushed to the side, stromal ablation performed, epithelium then replaced. Same refractive range as PRK (~8.0 D to +3.0 D, cylinder up to 3.0 D).
Epi-LASIK (Epithelial LASIK)
Epithelium is mechanically separated from Bowman layer using a blunt epi-keratome, moved aside for ablation, then replaced (epi-on) or discarded (epi-off). Same refractive range as PRK.
SMILE (Small Incision Lenticule Extraction)
A flapless technique. A femtosecond laser creates a thin disc of intrastromal tissue (lenticule), which is then mechanically extracted through a small stromal incision.
- No flap whatsoever
- Corrects myopia and myopic astigmatism
- Range: spherical ~10.0 D to ~1.0 D, cylinder up to 3.0 D
- Transient light sensitivity syndrome incidence ~1% (vs 5-9% for LASIK)
Comparison Table (from Wills Eye Manual)
| Feature | PRK | LASEK | Epi-LASIK | LASIK | SMILE |
|---|---|---|---|---|---|
| Stromal exposure | No flap; epithelium removed | Epithelial flap (alcohol) | Epithelial flap (epi-keratome) | Epithelial + stromal flap | No flap; lenticule extracted |
| Depth | Bowman membrane | Bowman membrane | Bowman membrane | Anterior stroma | Anterior stroma |
| Myopia range | up to ~8.0 D | up to ~8.0 D | up to ~8.0 D | up to ~10.0 D | up to ~10.0 D |
| Key advantage | Good for thin corneas; no flap | Similar to PRK | Similar to PRK | Wider range; faster recovery | Flapless; less dry eye |
3B. Intraocular Refractive Procedures (for high refractive errors)
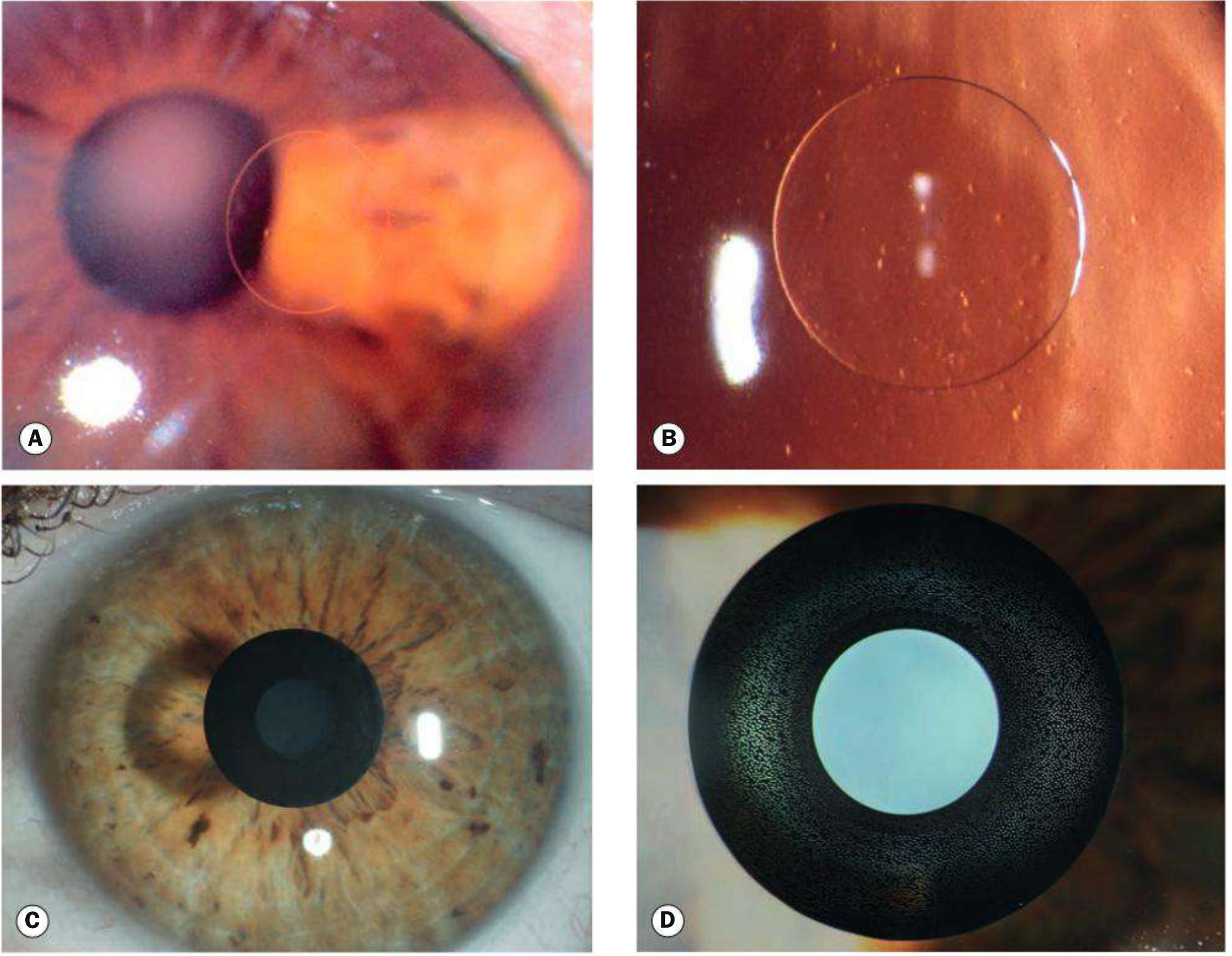
Phakic Intraocular Lenses (IOLs)
Used when refractive error exceeds limits for laser surgery. Two types:
-
Iris clip ("lobster claw") implant - attached to iris (Artisan/Verisyse)
- Complications: subluxation, dislocation, oval pupil, progressive endothelial cell loss, cataract, raised IOP, angle-closure glaucoma
-
Posterior chamber phakic IOL (e.g., ICL - implantable collamer lens) - placed between iris and crystalline lens
- Complications: pupil block glaucoma, cataract formation, incorrect power
Retinal detachment and endophthalmitis occur at ~3% per patient year.
Clear Lens Exchange (Refractive Lens Exchange)
Removal of the crystalline lens and insertion of an IOL. Gives excellent visual results but carries risk of cataract surgery complications, particularly retinal detachment in high myopia.
3C. Presbyopia Correction
Intracorneal Inlays
Two main types:
- Refractive inlay - alters corneal curvature
- Small aperture inlay - uses the pinhole effect for extended depth of focus
4. Correction by Refractive Error
| Refractive Error | Suitable Procedures |
|---|---|
| Low-moderate myopia | PRK, LASEK, Epi-LASIK, LASIK, SMILE |
| Moderate-high myopia | LASIK, SMILE |
| Very high myopia | Phakic IOL, Clear lens exchange |
| Hypermetropia (up to 3-4 D) | LASIK (PRK for lower degrees) |
| Astigmatism (up to 5 D) | LASIK, surface ablation (up to 3 D) |
| Presbyopia | Intracorneal inlays, multifocal IOLs, monovision |
5. Complications
Complications of Surface Ablation (PRK / LASEK / Epi-LASIK)
Early (days to weeks):
- Epithelial defect (usual - takes days to heal; bandage contact lens used)
- Pain (from induced epithelial defect)
- Dislocated or poorly fitting bandage lens
- Non-healing epithelial defect
- Bacterial keratitis / corneal ulcer
- HSV reactivation
Late (weeks to months):
- Corneal haze (scarring in anterior stroma) - causing decreased vision, glare, monocular diplopia
- Treatment: increase steroid frequency; severe cases - excimer PTK with mitomycin C
- Undercorrection or overcorrection
- Irregular astigmatism (central island, decentered ablation)
- Regression of refractive error
- Steroid-induced glaucoma / ocular hypertension
Complications of LASIK
Early (days to 1 week):
- Dry eye / neurotrophic keratopathy - by far the most common early complication; reduced corneal sensation for at least 3 months (returns to normal in 6-12 months)
- Folding, dislocation, or loss of corneal flap
- Large epithelial defect
- Diffuse lamellar keratitis (DLK) - "sands of the Sahara" - multiple fine inflammatory infiltrates at the flap interface within 5 days; treat with intensive topical antibiotic + steroids
- Infection in flap interface (bacterial keratitis)
- Central toxic keratopathy (CTK) - central stromal opacification/consolidation of unknown etiology; tends to improve over 6-12 months
Late:
- Epithelial ingrowth under flap (1-2%) - treat by lifting flap and scraping cells; ethanol or mitomycin C application possible
- Corneal haze (less common than after surface ablation)
- Irregular astigmatism (decentered ablation, flap irregularity, ectasia)
- Regression/progression of refractive error
- Chronic dry eye syndrome
- Pressure-induced stromal keratitis (PISK) - high IOP (often steroid-induced) causes fluid in the interface; IOP falsely low on central measurement, so measure peripheral to flap edge with Tono-Pen
- Corneal ectasia (0.2-0.6%) - most devastating complication
- Risk factors: abnormal preoperative topography (forme fruste keratoconus, pellucid marginal degeneration), low preoperative corneal thickness, low residual stromal bed, high myopia, young age, high percentage of corneal tissue altered
Transient light sensitivity syndrome: Occurs 2-8 weeks post-op; more common after hyperopic LASIK (9%) than myopic LASIK (5%) or SMILE (1%); responds to topical steroids.
Dry eye and tear film instability: Up to 70% of patients; usually improves spontaneously.
Workup for Post-Refractive Surgery Problems
- Complete slit lamp examination with fluorescein staining + IOP (Tono-Pen + applanation)
- Note: IOP may be underestimated due to reduced corneal thickness after ablation
- Refraction - hard contact lens overrefraction corrects irregular astigmatism
- Corneal topography/tomography if irregular astigmatism suspected
- Corneal OCT for epithelial thickness mapping
6. Key Tips (Kanski)
- LASIK may cause transient dry eye and glare from subepithelial haze
- Patients at occupational/recreational risk of eye trauma should be counselled for surface ablation (PRK) over LASIK
- Residual stromal bed must be ≥250 μm after ablation to prevent ectasia
- Refractive stability should be present for at least 1 year before LASIK
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., Chapter 8 (Corneal and Refractive Surgery) | The Wills Eye Manual, Section 4.29 (Corneal Refractive Surgery Complications)
Eyelid
Asking for Preferences
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Here is the complete eyelid chapter summary from Kanski's Clinical Ophthalmology (10th ed.) and The Wills Eye Manual, organized by topic:
The Eyelid - Comprehensive Ophthalmology Review
1. Blepharitis
Chronic marginal blepharitis is extremely common. Divided into anterior and posterior forms (mixed is most frequent).
Anterior blepharitis affects lash bases:
- Staphylococcal - abnormal immune response to S. aureus; associated with atopic dermatitis; causes peripheral corneal infiltrates
- Seborrhoeic - linked to generalized seborrhoeic dermatitis (scalp, nasolabial folds)
Posterior blepharitis (MGD):
- Meibomian gland dysfunction → bacterial lipases produce free fatty acids → raised meibum melting point → gland obstruction → increased tear evaporation and instability
- Strongly associated with acne rosacea
Demodex blepharitis:
- D. folliculorum longus (anterior) and D. folliculorum brevis (posterior)
- Collarettes at lash bases = pathognomonic of Demodex infestation
Symptoms: Burning, grittiness, photophobia, crusting (poor symptom-sign correlation)
Treatment: Lid hygiene (warm compresses + lid scrubs), topical antibiotics, oral doxycycline for MGD/rosacea, tea tree oil for Demodex, artificial tears.
2. Ptosis
Classification
| Type | Mechanism | Examples |
|---|---|---|
| Neurogenic | Innervational defect | 3rd nerve palsy, Horner syndrome |
| Myogenic | Levator myopathy or NMJ defect | Myasthenia gravis, myotonic dystrophy, CPEO |
| Aponeurotic (involutional) | Levator aponeurosis dehiscence | Most common acquired type; age-related |
| Mechanical | Mass or scarring | Tumour, oedema, dermatochalasis |
| Congenital | Levator dysgenesis | Simple congenital, Marcus Gunn jaw-winking |
Pseudoptosis - Causes
- Lack of globe support (artificial eye, enophthalmos, microphthalmos)
- Contralateral lid retraction (upper lid normally covers superior 2 mm of cornea)
- Ipsilateral hypotropia (lid follows globe downward; disappears on covering fellow eye)
- Brow ptosis (VII nerve palsy - diagnose by manually lifting brow)
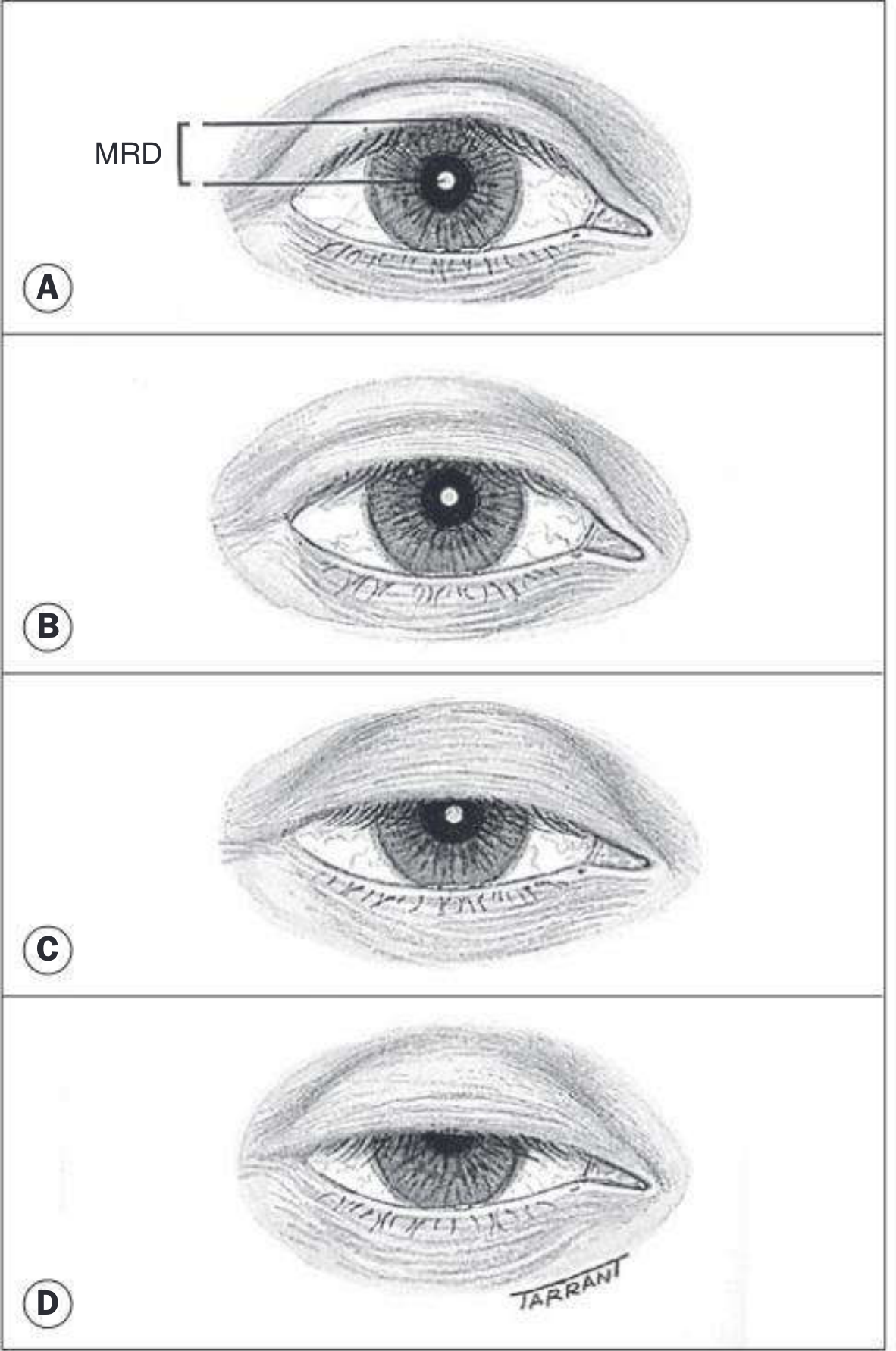
Clinical Measurements
- MRD (margin-reflex distance): Normal ~4-5 mm; reduced in ptosis
- Ptosis grading: Mild ≤2 mm, Moderate 3 mm, Severe ≥4 mm
- Palpebral fissure height: Males 7-10 mm, Females 8-12 mm
- Levator function: Normal ≥15 mm | Good 12-14 mm | Fair 5-11 mm | Poor ≤4 mm
- Lid crease height: Males ~8 mm, Females ~10 mm
- Absent crease → poor levator function (congenital)
- High crease → aponeurotic defect
Causes to Always Exclude (Wills Eye Manual)
- Horner syndrome | 2. CN III palsy | 3. Myasthenia gravis | 4. Orbital tumour | 5. Lid/conjunctival tumour | 6. CPEO (Kearns-Sayre)
Ptosis Surgery
- Levator resection - for myogenic/congenital with fair-good levator function
- Levator aponeurosis advancement - for involutional/aponeurotic ptosis
- Fasanella-Servat - for mild Horner or small aponeurotic ptosis
- Frontalis sling - for severe ptosis with poor levator function (≤4 mm)
3. Ectropion (Lid turned outward)
Most commonly affects the lower lid in the elderly. Causes epiphora, conjunctival keratinization.
Types & Treatment
Involutional (most common):
- Horizontal lid laxity (>8 mm pull-distraction; no snap-back)
- Lateral canthal laxity (rounded canthus; lid moves >2 mm medially)
- Medial canthal laxity (punctum displaced; severe = reaches pupil)
- Treatment: Lateral tarsal strip procedure; medial spindle for medial ectropion
Cicatricial: Vertical anterior lamellar shortening (burns, skin disease) → skin graft / Z-plasty
Paralytic (VII nerve palsy): Orbicularis weakness → lagophthalmos, exposure keratopathy → lubricants, taping, lateral tarsorrhaphy, eyelid weighting (gold/platinum implant)
Mechanical: Mass effect pulling lid from globe
4. Entropion (Lid turned inward)
Lash-to-cornea contact → irritation, punctate erosions, pannus, ulceration.
Types
Involutional (most common - lower lid):
Mechanisms:
- Horizontal lid laxity
- Lower lid retractor attenuation (reduced lid excursion in downgaze)
- Over-riding of pre-tarsal by preseptal orbicularis → tips lid inward
- Orbital septum laxity + fat prolapse
Treatment:
- Temporary: lubricants, taping, bandage lens, botulinum toxin to orbicularis
- Surgical: Everting sutures, Wies procedure (full-thickness lid split + sutures), lower lid retractor reinsertion, tarsal strip for laxity
Cicatricial (upper or lower lid):
- Causes: trachoma, cicatrizing conjunctivitis, chemical burns, Stevens-Johnson syndrome, MMP
- Treatment: posterior lamellar lengthening with mucous membrane or hard palate graft
Congenital - Epiblepharon:
- Common in Asian children
- Extra skin fold pushes lashes toward cornea
- Usually resolves spontaneously; surgery if persistent corneal staining
Trichiasis (misdirected lashes from otherwise normal lid): Treated by epilation, electrolysis, cryotherapy, or argon laser ablation.
5. Chalazion & Hordeolum
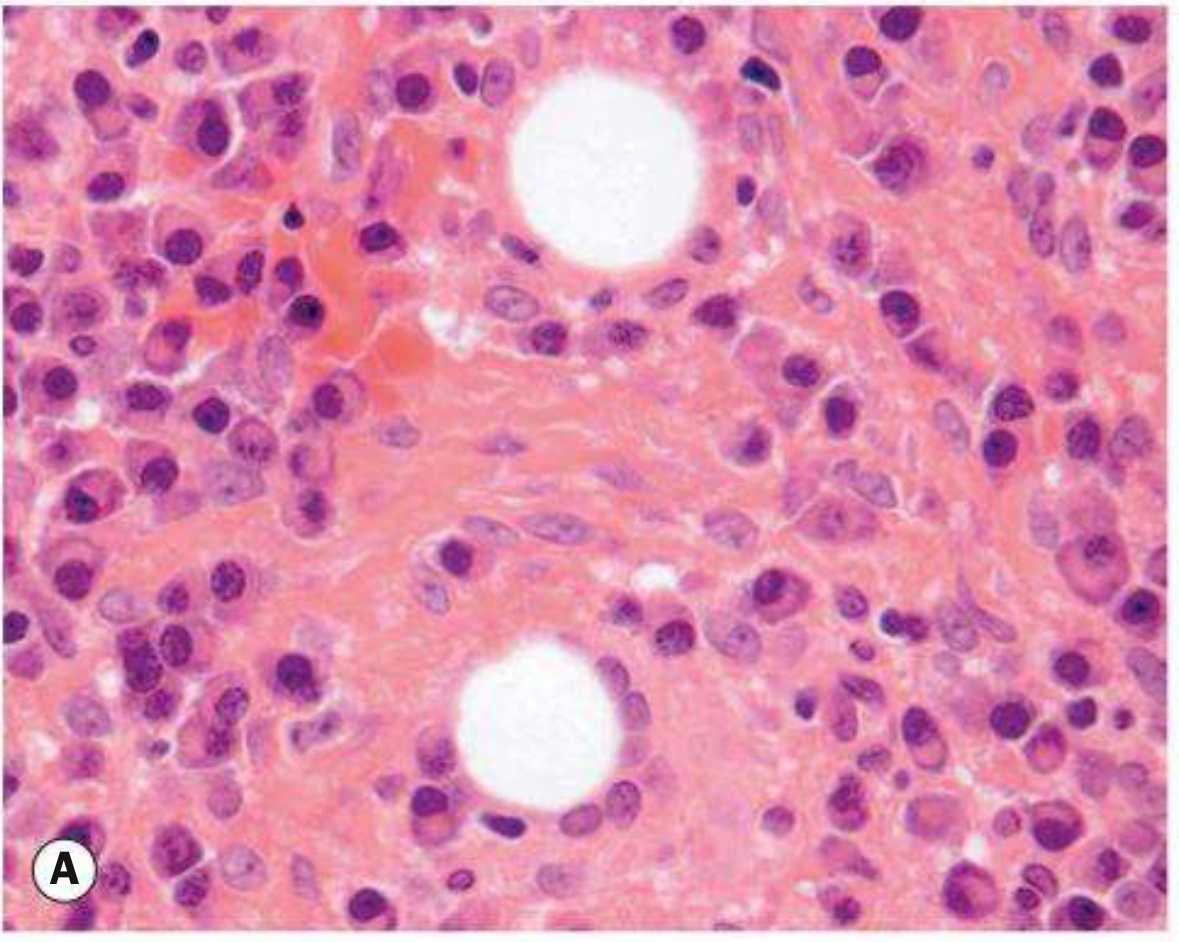
Chalazion: Sterile chronic lipogranuloma of meibomian (or Zeis) gland; caused by retained sebaceous secretions → giant cell reaction.
- Histopathology: lipid-laden epithelioid cells, multinucleated giant cells, lymphocytes
Hordeolum: Acute staphylococcal infection
- External (stye) = glands of Zeis/Moll on lid margin
- Internal = meibomian gland abscess
Associations: Blepharitis, acne rosacea, bortezomib therapy
Treatment:
- Warm compresses QID + massage
- Topical antibiotic (hordeolum) or antibiotic-steroid ointment (chalazion)
- Oral doxycycline 20-50 mg daily-BID for recurrent/rosacea
- After 3-4 weeks if persistent: incision and curettage or intralesional triamcinolone (0.2-1.0 mL of 40 mg/mL mixed 1:1 with lidocaine/epi)
- Send all excised tissue for histopathology
KEY: Recurrent chalazion at the same site in an older patient = biopsy to exclude sebaceous gland carcinoma.
6. Eyelid Tumors
Benign
| Tumor | Notes |
|---|---|
| Squamous papilloma | Most common benign lid tumor |
| Seborrhoeic keratosis | Waxy, stuck-on; elderly |
| Xanthelasma | Yellow medial canthal plaques; ~50% have hyperlipidaemia |
| Capillary haemangioma | Children; causes amblyopia from ptosis |
| Molluscum contagiosum | Umbilicated; causes follicular conjunctivitis near lid margin |
Malignant
Basal Cell Carcinoma (BCC) - 90% of all eyelid malignancies
- Lower lid > medial canthus > upper lid > lateral canthus
- Medial canthal BCC = most dangerous (orbital/sinus invasion; highest recurrence)
- Locally invasive, never metastasizes
- Features: madarosis, telangiectasia, slow growth
| Pattern | Description |
|---|---|
| Nodular | Pearly, shiny nodule with telangiectasia |
| Nodulo-ulcerative (rodent ulcer) | Central ulcer + pearly rolled edges |
| Morphoeic (sclerosing) | Flat, waxy, indurated; ill-defined; most aggressive |
| Pigmented | May mimic melanoma |
Histology: Basophilic cells with peripheral palisading of nuclei at lobule edges
Treatment: Complete excision with clear margins; Mohs surgery for high-risk (medial canthal, morphoeic, recurrent).
Sebaceous Gland Carcinoma (SGC)
- Upper eyelid predominant (more meibomian glands)
- Masquerades as chalazion (nodular type) or blepharitis (spreading type)
- Yellow discolouration within tumour is highly suggestive
- Pagetoid spread (intraepithelial extension) - may be extensive
- Mortality 5-10%; worse prognosis: upper lid, size ≥10 mm, symptoms >6 months
- Histology: foamy vacuolated lipid-containing cytoplasm + hyperchromatic nuclei
SCC: Second most common (~5%); can metastasize; may arise from actinic keratoses.
Melanoma: Rare but lethal; 50% amelanotic (no pigment); suspect any changing/irregular lid lesion >6 mm.
7. Miscellaneous & Congenital
Dermatochalasis: Excess skin from ageing → visual field loss → treat by blepharoplasty.
Floppy Eyelid Syndrome: Lax lids evert during sleep; associated with obstructive sleep apnoea and obesity; causes papillary conjunctivitis.
Blepharochalasis: Recurrent episodic eyelid oedema (young women) → atrophic thin skin + ptosis.
Upper lid retraction: Lid margin above superior limbus; most common cause = thyroid eye disease (Dalrymple's sign).
Blepharophimosis-Ptosis-Epicanthus Inversus (BPES): Autosomal dominant (FOXL2 gene); small horizontal fissure + bilateral ptosis + telecanthus + epicanthus inversus.
Epiblepharon: Common in Asian children; extra skin fold pushes lashes toward cornea; usually resolves spontaneously.
Coloboma: Full-thickness lid defect; upper lid; associated with Goldenhar syndrome.
Eyelid Malignancy Red Flags
| Finding | Suspect |
|---|---|
| Recurrent chalazion at same site (elderly) | Sebaceous gland carcinoma |
| Unilateral chronic "blepharitis" not responding to treatment | Sebaceous gland carcinoma |
| Madarosis (lash loss) with lid lesion | Malignancy (BCC, SGC, SCC) |
| Pearly nodule + rolled edges + central ulcer | BCC (rodent ulcer) |
| New/changing pigmented lid lesion >6 mm | Melanoma |
| Upper lid thickening with yellow tinge | SGC |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., Chapter 2 | The Wills Eye Manual, Sections 6.1-6.3
Orbit opthalmology
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content across all orbital topics. Let me compile the full response.
The Orbit - Ophthalmology
Kanski's Clinical Ophthalmology 10th ed. & The Wills Eye Manual
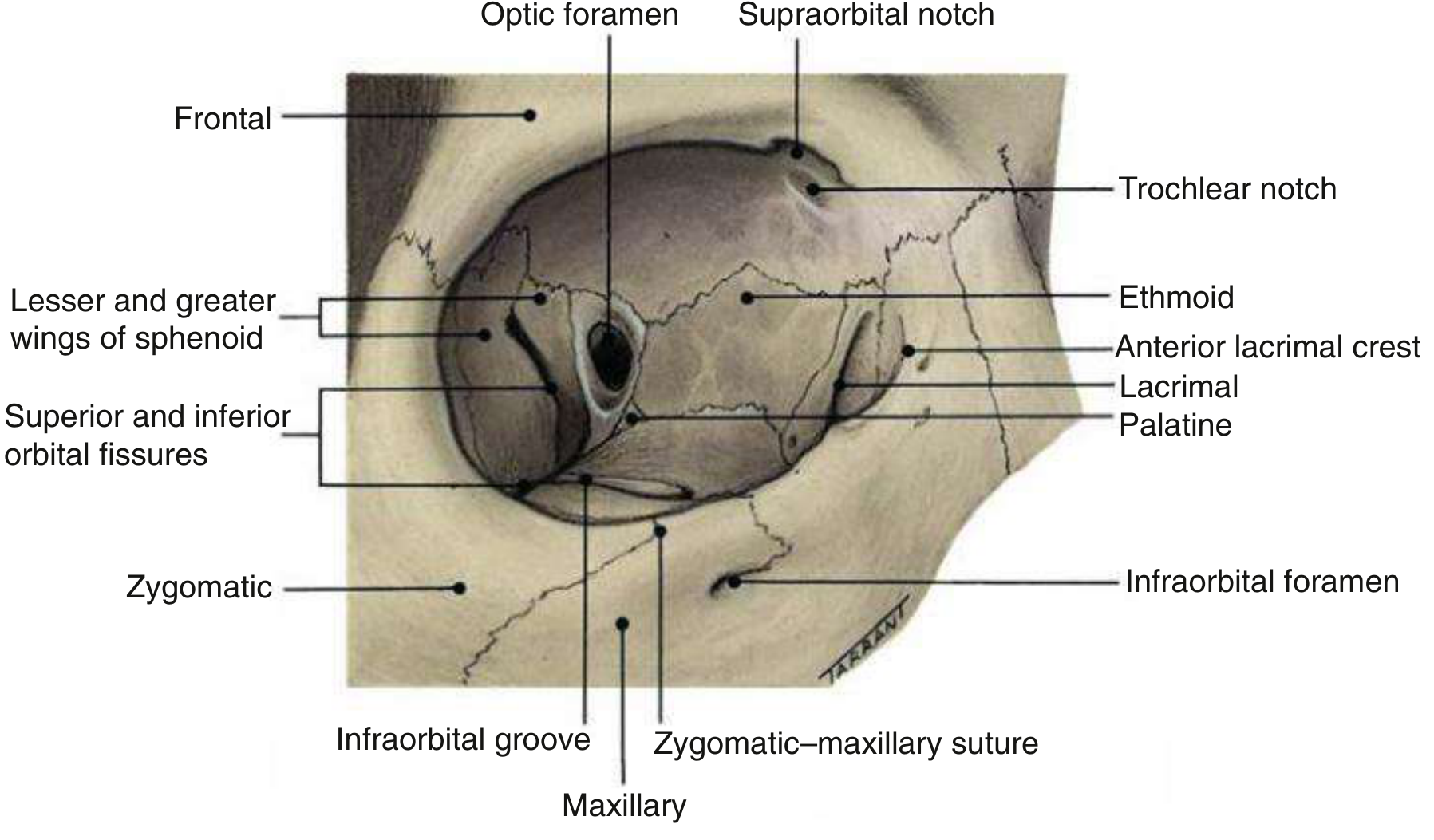
1. Orbital Anatomy
The orbit is a pear-shaped bony cavity containing the eyeball, extraocular muscles, lacrimal gland, blood vessels, nerves, and fat. Key anatomical facts:
- The intraorbital optic nerve is 25 mm long, while the distance from the back of the globe to the optic canal is only 18 mm - this slack allows forward displacement of the globe (proptosis) without excessive nerve stretch
- Walls: roof (frontal bone/lesser sphenoid wing), lateral wall (zygomatic/greater sphenoid wing), floor (maxilla/zygoma/palatine), medial wall (ethmoid/lacrimal/maxilla/sphenoid) - the medial wall and floor are thinnest, most prone to fracture
2. Approach to the Orbit: Proptosis
Proptosis = abnormal protrusion of the globe. Exophthalmos = proptosis specific to the eyeball. Measured by Hertel exophthalmometry.
Assessment of Proptosis
Direction of displacement:
- Axial (straight forward) → intraconal mass (within the muscle cone), e.g. cavernous haemangioma, optic nerve tumour, TED
- Non-axial (dystopia/eccentric) → extraconal mass, e.g. lacrimal gland tumour (inferomedial displacement), dermoid (superolateral), rhabdomyosarcoma (superior)
Key examination steps:
- Asymmetrical proptosis - best detected by looking down at the patient from above and behind
- Resistance to retropulsion (pushback of globe) - indicates firm/infiltrative mass
- Pulsatile proptosis - suggests carotico-cavernous fistula or orbital encephalocele
- Fundoscopy - look for optic disc swelling, choroidal folds, optociliary vessels
Differential diagnosis of proptosis (from Wills Eye Manual):
| Category | Examples |
|---|---|
| Thyroid | TED (most common adult cause - bilateral AND unilateral) |
| Vascular | Carotico-cavernous fistula, varix, orbital haemorrhage |
| Inflammatory | Orbital pseudotumour (IOID), orbital myositis, sarcoidosis, GPA |
| Infectious | Bacterial/fungal cellulitis, mucormycosis |
| Benign tumour | Cavernous haemangioma (most common adult orbital tumour), lacrimal gland adenoma, dermoid |
| Malignant tumour | Rhabdomyosarcoma (children), lymphoma, metastasis, lacrimal gland carcinoma |
| Bony | Fibrous dysplasia, Paget's disease, sphenoid wing meningioma |
| Congenital | Encephalocele, dermoid, capillary haemangioma |
Enophthalmos (posterior displacement of globe): causes include orbital floor fracture (blowout), silent sinus syndrome, scirrhous metastasis (breast), phthisis bulbi, Horner syndrome (mild), post-enucleation.
3. Thyroid Eye Disease (TED)
Also called thyroid-associated orbitopathy (TAO) or Graves' ophthalmopathy.
Key Facts
- Most common cause of both unilateral and bilateral proptosis in adults
- 5x more common in women (reflects Graves' disease prevalence)
- Smoking is the major modifiable risk factor - dose-dependent; cessation reduces risk
- Radioiodine therapy for hyperthyroidism can worsen TED (give oral steroids prophylactically)
- Can occur in euthyroid and hypothyroid patients
Pathogenesis
Anti-thyrotropin receptor antibodies (TRAb) react against thyroid cells AND orbital fibroblasts. IGF-1R and TSHR are upregulated on orbital fibroblasts → inflammation, glycosaminoglycan deposition → osmotic water imbibition → muscles swell up to 8× normal size → secondary lipogenesis (orbital fat enlargement) → raised intraorbital pressure → optic nerve compression. Eventual fibrosis → restrictive myopathy.
Clinical Course
- Congestive (inflammatory) stage: Red, painful eyes; lasts 1-3 years
- Fibrotic (quiescent) stage: White eyes, fixed motility defect
Only ~10% develop serious long-term ocular problems.
Clinical Features
EUGOGO (2021) Activity Score (1 point each):
- Spontaneous retrobulbar pain
- Pain on attempted upgaze or downgaze
- Redness of eyelids
- Redness of conjunctiva
- Swelling of conjunctiva or plica
- Swelling of eyelid
- Chemosis
Score ≥3/7 = active disease → consider immunosuppression
EUGOGO Severity:
- Mild: Minor impact on daily life
- Moderate-severe: ≥1 of: moderate-severe soft tissue involvement, lid retraction ≥2 mm, diplopia, proptosis ≥3 mm above normal
- Sight-threatening: Optic neuropathy or corneal breakdown
Five Clinical Categories
(1) Soft Tissue Involvement
- Grittiness, red eyes, lacrimation, photophobia, puffy lids, retrobulbar discomfort
- Epibulbar hyperaemia (especially over horizontal rectus insertions) - sensitive activity marker
- Periorbital oedema + chemosis + retroseptal fat prolapse into lids
- Tear insufficiency and instability
(2) Lid Retraction
Affects ~50% of Graves' disease patients.
- Upper lid: Müller muscle overaction (sympathetic overstimulation from high thyroid hormones); levator fibrosis
- Lower lid: Inferior rectus fibrosis pulls lower lid down
- Signs: Dalrymple's sign (upper lid retraction - above superior limbus), von Graefe's sign (lid lag on downgaze), lagophthalmos
- Lateral flare of upper lid retraction is highly specific for TED
(3) Proptosis
- Axial, bilateral (but often asymmetric) or unilateral
- Resistance to retropulsion is characteristic
- Caused by enlarged extraocular muscles + increased orbital fat volume

(4) Restrictive Myopathy (Ophthalmoplegia)
Occurs in 30-50% of TED patients. May be permanent.
| Muscle affected (fibrosis) | Resulting deficit | Mimics |
|---|---|---|
| Inferior rectus (most common) | Defective elevation | Superior rectus palsy |
| Medial rectus (2nd most common) | Defective abduction | VI nerve palsy |
| Superior rectus | Defective depression | - |
| Lateral rectus | Defective adduction | - |
Diagnosis confirmed by forced duction testing (resistance to passive globe movement).
IOP significantly elevated in upgaze is characteristic of TED.
EOM imaging pattern: Thickening of muscle bellies with sparing of tendons (contrast to myositis, where tendons are involved). Order of frequency: inferior > medial > superior > lateral rectus (mnemonic: "I'M SLow").
Isolated lateral rectus enlargement = atypical for TED → requires biopsy.
(5) Optic Neuropathy
Occurs in ~5-7% of TED patients - caused by apical compression of the optic nerve by congested/enlarged rectus muscles.
Key pearl: Compressive optic neuropathy in TED often occurs without significant proptosis - enlarged muscles compress the apex without pushing the globe forward.
Signs: Reduced VA, reduced color vision (dyschromatopsia), RAPD, visual field loss, optic disc swelling or pallor.
Investigation: MRI/CT orbital apex views (apical crowding); this is a sight-threatening emergency.
Treatment of TED
All patients:
- Stop smoking (first measure)
- Optimize thyroid function
- If radioiodine therapy planned: give concurrent oral steroids
Mild active disease:
- Lubricants, topical anti-inflammatories
- Selenium 200 μg/day for 6 months (in selenium-deficient areas)
- Head elevation to reduce periorbital oedema
- Eyelid taping for mild exposure
Moderate-severe active disease (CAS ≥3):
- IV methylprednisolone - regimen: 0.5 g weekly ×6 weeks, then 0.25 g weekly ×6 weeks. Superior outcomes and better tolerability than oral. Avoid in significant hepatic, cardiovascular, hypertensive, or diabetic disease.
- IV corticosteroids + mycophenolate sodium 0.72 g/day ×24 weeks = superior to IV steroid monotherapy (preferred at specialist centres)
- Low-dose fractionated orbital radiotherapy - second-line; maximal response by 4 months; ~40% non-responders; avoid in young patients and diabetics
- Teprotumumab (IGF-1R monoclonal antibody) - highly effective; reduces proptosis and CAS
Sight-threatening disease (optic neuropathy):
- Urgent IV methylprednisolone (1 g/day ×3 days)
- If no response in 1-2 weeks → emergency orbital decompression surgery
- Canthotomy/cantholysis for acute pressure rise
Surgical rehabilitation (quiescent disease, in order):
- Orbital decompression (for proptosis/corneal exposure) - removes orbital wall and/or fat
- Squint surgery (for diplopia from restrictive myopathy) - after proptosis stable
- Eyelid surgery (for retraction/lagophthalmos) - last step
4. Orbital Cellulitis
Key Distinction: Preseptal vs Orbital (Postseptal)
| Feature | Preseptal (periorbital) | Orbital (postseptal) |
|---|---|---|
| Septum involvement | Anterior to septum | Posterior to orbital septum |
| Proptosis | Absent | Present |
| Ophthalmoplegia | Absent | Present (painful) |
| Vision | Normal | May be reduced |
| RAPD | Absent | May be present |
| CT | No orbital fat involvement | Orbital fat stranding ± abscess |
Orbital Cellulitis
A serious, sight- and life-threatening infection. More common in children.
Common organisms:
- Adults: S. aureus, Streptococcus spp., anaerobes
- Children: S. pneumoniae, S. aureus, S. pyogenes, H. influenzae (rare if vaccinated)
- Post-trauma: Gram-negative rods
- Dental source: mixed aggressive aerobes + anaerobes
- Immunocompromised (diabetics, HIV, chemo): Mucor/Rhizopus (zygomycosis/mucormycosis), Aspergillus
Source: Most commonly ethmoid sinusitis (paranasal sinuses in children). Other sources: dacryocystitis, dacryoadenitis, dental infection, trauma, orbital surgery.
Chandler-Hubert Classification
| Stage | Description |
|---|---|
| I | Inflammatory oedema (preseptal) |
| II | Orbital cellulitis (fat stranding, no abscess) |
| III | Subperiosteal abscess (most common: medial wall) |
| IV | Orbital abscess |
| V | Cavernous sinus thrombosis |
Clinical Features
- Rapid onset: pain exacerbated by eye movement, lid swelling, proptosis, malaise
- Pyrexia (often marked)
- Painful ophthalmoplegia
- Conjunctival chemosis and injection
- Proptosis (often non-axial if abscess present)
- Reduced VA, colour vision, RAPD → suggests optic nerve compression (emergency)
- History of recent nasal/sinus/respiratory illness


Complications
- Ocular: Optic neuropathy, exposure keratopathy, raised IOP, CRAO/CRVO, endophthalmitis
- Subperiosteal abscess (medial wall most common)
- Intracranial (3-4%): Meningitis, brain abscess, cavernous sinus thrombosis
Investigation & Management
Investigations:
- CT orbits + paranasal sinuses + brain (with contrast) - mandatory
- CBC with differential, blood cultures, culture of nasal discharge
- Check tetanus status in trauma
Treatment:
- Hospital admission mandatory
- IV antibiotics until apyrexial for 4 days, then 1-3 weeks oral
- Community: ampicillin-sulbactam (adults); supplement with metronidazole for anaerobic cover
- Hospital/MRSA risk: add vancomycin
- Monitor optic nerve function every 4 hours (VA, colour vision, brightness comparison, pupil reactions)
- ORL (ENT) assessment for sinus drainage
- Surgical drainage of orbital/subperiosteal abscess at early stage if identified
- Deteriorating optic nerve → emergency canthotomy/cantholysis
Mucormycosis (Zygomycosis):
- Occurs in diabetics (especially in DKA) and immunocompromised
- Severe pain, external ophthalmoplegia, black eschar on nasal turbinates
- Profound visual loss may occur rapidly
- Treatment: aggressive surgical debridement + IV amphotericin B (urgent)
5. Idiopathic Orbital Inflammatory Disease (IOID / Orbital Pseudotumour)
Non-neoplastic, non-infective space-occupying orbital infiltration. Any orbital soft tissue may be involved; the process may be targeted (dacryoadenitis, myositis, anterior, posterior) or diffuse.
Histopathology: Pleomorphic inflammatory cellular infiltration → reactive fibrosis.
Epidemiology: Unilateral in adults; bilateral involvement may occur in children.
Clinical features:
- Acute or subacute ocular and periorbital redness, swelling, and pain
- Proptosis (congestive)
- Ophthalmoplegia (mild to severe)
- Optic nerve dysfunction (posterior orbit involvement)
- Choroidal folds
- Pyrexia in up to 50% of children (rare in adults)
Natural history:
- Spontaneous remission after a few weeks (best case)
- Intermittent episodes with eventual remission
- Severe prolonged disease → progressive fibrosis → "frozen orbit" (fixed ophthalmoplegia + ptosis + optic nerve involvement)
Subtypes:
- Orbital myositis - targets one or more extraocular muscles (unlike TED: tendons are also enlarged)
- Dacryoadenitis - lacrimal gland involvement
- Tolosa-Hunt syndrome - painful ophthalmoplegia from granulomatous inflammation at superior orbital fissure/cavernous sinus
Investigation:
- CT: ill-defined orbital opacification, loss of definition of contents
- MRI: better soft tissue characterization
- Biopsy: required in persistent cases to exclude lymphoma, sarcoidosis, GPA, infection
Treatment:
- Observation for mild disease
- NSAIDs alone (ibuprofen) - mild disease; add PPI
- Oral prednisolone 1.0-1.5 mg/kg/day - hallmark rapid dramatic response within 24-48 hrs (if no response, reconsider diagnosis)
- Orbital depot steroid injection - selected cases
- Radiotherapy - if no improvement after 2 weeks of adequate steroids
6. Orbital Tumours
Benign
Cavernous Haemangioma (Cavernous Venous Malformation)
- Most common primary orbital tumour in adults
- Female preponderance (70%); middle-aged; growth accelerated by pregnancy
- Vascular malformation (not a true neoplasm); low-flow AVM
- Located within the muscle cone, lateral to optic nerve
- Histology: Endothelial-lined vascular channels of varying size separated by fibrous septa
- Presentation: Slowly progressive axial proptosis, diplopia; often incidental
- Imaging: Well-defined, hyperdense on CT; "progressive fill" on dynamic contrast MRI
- Treatment: Observation if asymptomatic. Surgical excision if symptomatic - well-encapsulated, relatively easy to remove
Capillary Haemangioma
- Most common orbital tumour in children/infants
- Appears shortly after birth; grows rapidly in the first year; involutes by age 5-7
- Strawberry-red, compressible; increases with crying (Valsalva)
- Can cause amblyopia (from ptosis, astigmatism, or anisometropia)
- Treatment: Oral/topical propranolol (first line); systemic steroids if propranolol contraindicated; intralesional steroid injection
Dermoid Cyst
- Choristoma derived from trapped ectoderm along embryonic fusion lines
- Superolateral orbit (frontozygomatic suture) most common site
- Smooth, non-tender, non-pulsatile; may be anchored to bone
- CT: well-defined cyst with fat density; bone remodelling
- Treatment: surgical excision (rupture causes severe granulomatous inflammation)
Pleomorphic Lacrimal Gland Adenoma (Benign Mixed-Cell Tumour)
- Most common epithelial lacrimal gland tumour
- Young to middle-aged adults; painless slow progressive proptosis (>1 year)
- Superolateral orbit → inferomedial globe displacement
- CT: well-defined mass in lacrimal gland fossa + smooth bony remodelling (not erosion)
- Treatment: Complete excision with intact pseudocapsule (biopsy/incomplete excision risks malignant transformation → adenoid cystic carcinoma)
Malignant
Rhabdomyosarcoma (RMS) - Most Common Primary Orbital Malignancy in Children
- Most common soft tissue sarcoma of childhood; 40% in head and neck
- Mean age of onset: 7 years; 90% in children under 16
- Derived from undifferentiated mesenchymal cells
- Subtypes: Embryonal (85% of orbital RMS - best prognosis), Alveolar (worse prognosis, characteristic chromosomal translocations), Botyroid (4%), Pleomorphic
Key tip: RMS can mimic orbital cellulitis in a child - skin redness and swelling but skin is not warm.
Clinical features:
- Rapidly progressive unilateral proptosis (days to weeks)
- Most common location: superonasal or superior orbit
- Diplopia common; pain less common; no fever
- Swelling and redness of overlying skin (not warm)
Imaging:
- CT: poorly-defined homogeneous mass, often with adjacent bony destruction
- MRI: poorly-defined mass
Investigation:
- Incisional biopsy to confirm diagnosis + histological subtype + cytogenetic analysis
- Systemic staging: chest (lung metastases), bone scan (bone metastases are common)
Treatment: Combined radiotherapy + chemotherapy ± surgical debulking (IRSG staging guidelines). Good prognosis for orbital embryonal RMS when localized.
Orbital Lymphoma
- Most common orbital malignancy in adults (>60 years)
- MALT-type (extranodal marginal zone) B-cell lymphoma most common
- Salmon-pink "fish-flesh" conjunctival lesion
- Painless proptosis, diplopia
- Treatment: orbital radiotherapy for localized disease; systemic chemotherapy for disseminated
Lacrimal Gland Carcinoma (Adenoid Cystic Carcinoma - ACC)
- Most common malignant lacrimal gland tumour
- Pain is a key distinguishing feature from benign adenoma (perineural invasion)
- Bone erosion on CT (not smooth remodelling as in adenoma)
- Treatment: radical surgery + radiotherapy; poor prognosis
Orbital Metastases
- Adults: breast (most common, may cause enophthalmos from scirrhous reaction), lung, prostate, melanoma
- Children: neuroblastoma (bilateral orbital metastases with ecchymosis = "raccoon eyes"), Ewing's sarcoma, Wilms' tumour
7. Orbital Trauma
Orbital Floor Fracture (Blowout Fracture)
- Mechanism: blunt trauma to orbit → sudden rise in intraorbital pressure → thin orbital floor fractures (trapdoor or open book)
- Features:
- Enophthalmos (fat herniation into maxillary sinus)
- Diplopia (especially on upward gaze - inferior rectus/oblique entrapment)
- Infraorbital hypoesthesia (infraorbital nerve damage)
- Restricted upgaze (positive forced duction)
- Globe may appear sunken
- CT: best imaging - shows floor defect, soft tissue herniation, haemosinus
- Treatment: surgical repair if enophthalmos >2 mm, diplopia in primary or reading gaze, or large defect (>50% floor); wait 2 weeks for oedema to resolve before deciding
Orbital Haemorrhage
- Can be retrobulbar (sight-threatening); causes rapid rise in intraorbital pressure
- Presents with pain, proptosis, restricted EOM, raised IOP, visual loss, RAPD
- Emergency treatment: Lateral canthotomy + cantholysis to decompress the orbit
Summary: Key "Most Common" Facts in Orbital Disease
| Statement | Answer |
|---|---|
| Most common cause of bilateral and unilateral proptosis in adults | Thyroid Eye Disease |
| Most common primary orbital tumour in adults | Cavernous haemangioma |
| Most common primary orbital malignancy in children | Rhabdomyosarcoma |
| Most common orbital malignancy in adults | Lymphoma |
| Most common source of orbital cellulitis (from sinus) | Ethmoid sinus |
| Most common site of subperiosteal abscess | Medial orbital wall |
| Most common malignant lacrimal gland tumour | Adenoid cystic carcinoma |
| Most common benign lacrimal gland tumour | Pleomorphic adenoma |
| EOM most commonly affected in TED | Inferior rectus (defective elevation) |
| Restricted myopathy causing defective abduction - mimics | Fibrosis of medial rectus (mimics VI nerve palsy) |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., Chapter 4 (Orbit) | The Wills Eye Manual, Sections 7.1, 7.2.1 (TED), 7.3.1 (Orbital Cellulitis)
Cunjuctiva opthalmology
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I have rich content. Let me compile the comprehensive conjunctiva review now.
The Conjunctiva - Comprehensive Ophthalmology Review
Kanski's Clinical Ophthalmology 10th ed. & The Wills Eye Manual
1. Anatomy & Histology
The conjunctiva is a transparent mucous membrane lining the inner surface of the eyelids and the anterior globe surface, terminating at the corneoscleral limbus. Richly vascular, supplied by the anterior ciliary and palpebral arteries. Dense lymphatic network drains to preauricular and submandibular nodes.
Anatomical Divisions
| Region | Description |
|---|---|
| Palpebral conjunctiva | Starts at mucocutaneous junction of lid margins; firmly attached to posterior tarsal plates; vessels are vertically orientated |
| Fornical conjunctiva | Loose and redundant; allows free globe movement |
| Bulbar conjunctiva | Covers anterior sclera; continuous with corneal epithelium at limbus; loosely attached to Tenon capsule (except at limbus, where they fuse) |
Special structures:
- Palisades of Vogt - radial ridges at the limbus; reservoir of corneal stem cells (limbal stem cells)
- Plica semilunaris - semilunar fold nasally; vestigial third eyelid
- Caruncle - fleshy nodule medial to plica; modified cutaneous tissue
Histology
- Epithelium: Non-keratinizing, ~5 cell layers deep; basal cuboidal → superficial polyhedral cells
- Goblet cells (mucus-secreting): within epithelium; most dense inferotemporally and in the fornices; secrete mucin (innermost layer of tear film)
- Stroma (substantia propria): Richly vascularized loose connective tissue; contains accessory lacrimal glands of Krause (fornices) and Wolfring (near superior tarsal border) - provide basal tear secretion
- CALT (Conjunctiva-Associated Lymphoid Tissue): lymphocytes, lymphatics, and follicular aggregates; mediates ocular surface immunity
2. Clinical Signs of Conjunctival Inflammation
Symptoms
- Lacrimation, grittiness, stinging, burning
- Itching = hallmark of allergic disease
- Significant pain, photophobia, or marked foreign body sensation → suggests corneal involvement
- VA not usually affected in pure conjunctivitis
Discharge Types
| Type | Significance |
|---|---|
| Watery | Viral or acute allergic conjunctivitis |
| Mucoid | Chronic allergic conjunctivitis or dry eye |
| Mucopurulent | Bacterial conjunctivitis |
| Hyperacute purulent | Gonococcal or meningococcal (emergency) |
Conjunctival Reaction Patterns
Follicles:
- Discrete, slightly elevated, translucent, rice-grain lesions
- Most prominent in the fornices
- Blood vessels run around or across the lesion (not within)
- Contain germinal centres of lymphocytes (reactive lymphoid tissue)
- Causes: viral (adenovirus, EBV, HSV), chlamydial, molluscum contagiosum, toxic (topical medications - especially brimonidine, apraclonidine, idoxuridine)
Papillae:
- Raised, red, polygonal lesions with a central vascular core (blood vessels run through the centre)
- Non-specific response to inflammation
- Large (>1 mm) = "giant papillae"; found on upper tarsal conjunctiva in VKC and GPC
- Causes: bacterial, allergic, chlamydial, giant papillary conjunctivitis
Membranes and pseudomembranes:
- True membrane - involves superficial epithelial layers; removal causes bleeding; leaves scarring
- Pseudomembrane - loosely adherent fibrinous exudate; removal is easy, no bleeding
- Both can cause scarring
- Causes: severe adenoviral EKC, gonococcal, Streptococcus, Corynebacterium diphtheriae, Stevens-Johnson syndrome, ligneous conjunctivitis
Subconjunctival cicatrization (scarring): Trachoma, MMP, SJS, chemical burns, chronic conjunctivitis → loss of goblet cells/accessory lacrimal glands → dry eye, cicatricial entropion.
Symblepharon: Adhesion between bulbar and palpebral conjunctiva. Causes: MMP, SJS, chemical injury, severe adenoviral EKC, atopic conjunctivitis.
3. Bacterial Conjunctivitis
Acute Bacterial Conjunctivitis
Common organisms: S. pneumoniae, S. aureus, H. influenzae, Moraxella catarrhalis
Clinical features:
- Common, usually self-limiting
- Bilateral (one eye 1-2 days before the other)
- Lids stuck together on waking (mucopurulent discharge)
- Conjunctival injection; discharge initially watery, rapidly becomes mucopurulent
- Corneal punctate epithelial erosions common
- Lymphadenopathy usually absent (except with gonococcal/meningococcal)
Treatment: Usually self-limiting. Topical antibiotics (chloramphenicol, fusidic acid, or fluoroquinolone) speed resolution.
Gonococcal Conjunctivitis
Organism: Neisseria gonorrhoeae
Key feature: Hyperacute purulent discharge - copious, profuse, starts within hours.
Critical: N. gonorrhoeae can penetrate intact corneal epithelium → rapid corneal ulceration and perforation within 24-48 hrs.
Signs:
- Hyperacute purulent discharge (gross, "taps open")
- Marked lid oedema and erythema
- Conjunctival chemosis
- Preauricular lymphadenopathy (present, unlike simple bacterial conjunctivitis)
Treatment:
- Ceftriaxone 1 g IM single dose (adults) + saline irrigation
- Treat sexual contacts
- Screen for other STIs
- Neonates: ceftriaxone 25-50 mg/kg IV/IM
Adult Chlamydial (Inclusion) Conjunctivitis
Organism: C. trachomatis serovars D-K (oculogenital; distinct from trachoma serovars A-C)
Transmission: Autoinoculation from genital secretions (90%); eye-to-eye (10%). Incubation ~1 week.
Systemic associations:
- Males: non-gonococcal urethritis (NGU); trigger for Reiter syndrome
- Females: urethritis, PID, infertility; Fitz-Hugh-Curtis syndrome (perihepatitis) in 5-10% with PID
Signs:
- Subacute onset, unilateral or bilateral
- Watery or mucopurulent discharge
- Tender preauricular lymphadenopathy (characteristic)
- Large follicles prominent in inferior fornix and upper tarsal plate
- Superficial punctate keratitis
- Perilimbal subepithelial corneal infiltrates (2-3 weeks)
- Superior corneal pannus (chronic cases)
Investigations:
- Giemsa staining of conjunctival scrapings: basophilic intracytoplasmic inclusion bodies
- PCR (nucleic acid amplification) - most sensitive
- Direct immunofluorescence (~90% sensitivity)
Treatment: Systemic antibiotics mandatory
- Azithromycin 1 g single oral dose, OR
- Doxycycline 100 mg BD × 7 days
- Treat sexual partners
Trachoma
World's leading cause of preventable irreversible blindness. Associated with poverty, overcrowding, poor hygiene.
Organism: C. trachomatis serovars A, B, Ba, C
Pathogenesis: Single episode = relatively innocuous. Recurrent infections → chronic cell-mediated (type IV hypersensitivity) immune response → progressive conjunctival scarring → entropion → trichiasis → corneal scarring → blindness.
WHO SAFE Strategy:
- Surgery (for trichiasis/entropion - bilamellar tarsal rotation)
- Antibiotics (active disease and family members)
- Facial hygiene
- Environmental improvement
WHO Grading:
| Grade | Name | Description |
|---|---|---|
| TF | Trachomatous follicular inflammation | ≥5 follicles ≥0.5 mm in upper tarsal conjunctiva |
| TI | Trachomatous intense inflammation | Pronounced upper tarsal inflammation obscuring >50% of deep tarsal vessels |
| TS | Trachomatous scarring | Scarring of upper tarsal conjunctiva (white bands/lines) |
| TT | Trachomatous trichiasis | ≥1 eyelash rubbing the eyeball |
| CO | Corneal opacity | Corneal opacity over pupil |
Active trachoma signs:
- Mixed follicular/papillary conjunctivitis
- Mucopurulent discharge
- Herbert's pits - limbal follicles that scar → depressions at superior limbus (pathognomonic)
- Superior corneal pannus
Cicatricial trachoma signs:
- Arlt's line - horizontal scar in upper tarsal plate
- Trichiasis, entropion → corneal ulceration → opacity → blindness
Treatment:
- Azithromycin 20 mg/kg (max 1 g) single dose - treatment of choice
- Alternatives: erythromycin 500 mg BD × 14 days; doxycycline 100 mg BD × 10 days (not in pregnancy or children <12)
- Topical tetracycline 1% ointment - less effective than oral
Neonatal Conjunctivitis (Ophthalmia Neonatorum)
Definition: Conjunctival inflammation in the first month of life. Most common neonatal infection (up to 10%).
Timing of onset by organism:
| Timing | Cause |
|---|---|
| First 1-2 days | Chemical (silver nitrate, topical prophylaxis) |
| First week | Gonococcal (N. gonorrhoeae) |
| Days 3-10 | General bacteria (Staph, Strep, H. influenzae) |
| 5-14 days | Chlamydial (C. trachomatis - most common cause of moderate-severe) |
| Within days-2 weeks | HSV-2 (may have skin vesicles; systemic involvement) |
Most dangerous: Gonococcal (corneal perforation risk) and HSV (systemic dissemination).
Treatment:
- Gonococcal: ceftriaxone IM/IV + saline irrigation
- Chlamydial: systemic erythromycin (oral) × 14 days (topical alone inadequate; prevents chlamydial pneumonia)
- HSV: IV aciclovir
Prophylaxis: Topical antibiotic at delivery (erythromycin ointment most widely used; povidone-iodine also used)
4. Viral Conjunctivitis
Adenoviral Conjunctivitis (most common = 90% of viral conjunctivitis)
Highly contagious. Spreads by respiratory/ocular secretions and fomites; viral particles survive on dry surfaces for weeks. Viral shedding may precede symptoms.
Three main clinical forms:
Non-specific Acute Follicular Conjunctivitis
- Most common form; mild; various adenoviral serotypes
- Unilateral watery discharge, redness, irritation; fellow eye affected 1-2 days later
- Mild systemic symptoms (sore throat, common cold)
Pharyngoconjunctival Fever (PCF)
- Adenovirus serovars 3, 4, 7
- Spread by droplets; family outbreaks
- Prominent sore throat + conjunctivitis + fever
- Keratitis in ~30% but seldom severe
Epidemic Keratoconjunctivitis (EKC) - most severe
- Adenovirus serovars 8, 19, 37
- Keratitis in ~80% of cases - may be severe with marked photophobia
- Subepithelial infiltrates (SEI) develop weeks after onset - represent immune reaction - can persist months-years and impair vision
- May cause pseudomembranes, symblepharon, and long-term dry eye
Signs of adenoviral conjunctivitis:
- Follicular conjunctival reaction
- Preauricular lymphadenopathy
- Subconjunctival haemorrhages (especially EKC)
- Pseudomembrane formation (EKC)
- Subepithelial corneal infiltrates
Treatment:
- Supportive: cool compresses, lubricants
- Topical steroids/NSAIDs for severe cases (SEI, significant keratitis) - but steroids can prolong viral shedding
- Topical povidone-iodine (off-label) may shorten course
- Hand hygiene / isolate to prevent spread
Other Viral Causes
- HSV: Follicular conjunctivitis in primary infection; often unilateral; associated eyelid vesicles; treat with topical/oral aciclovir
- Molluscum contagiosum: Umbilicated lid margin lesions shed viral particles → chronic follicular conjunctivitis - treat by excision of lid lesion
- Acute haemorrhagic conjunctivitis: Enterovirus / Coxsackievirus; rapid onset; prominent subconjunctival haemorrhage; resolves in 1-2 weeks; tropical regions
- SARS-CoV-2 (COVID-19): Viral RNA in tears in ~25% of moderate-severe cases; mild follicular conjunctivitis; usually benign
5. Allergic Conjunctivitis
All forms are type I hypersensitivity (IgE-mediated mast cell degranulation); some have element of type IV as well.
Acute Allergic Conjunctivitis
- Usually in children after playing outdoors in spring/summer
- Trigger: pollen
- Acute itching + watering + dramatic chemosis (hallmark)
- Self-limiting; resolves within hours
- Treatment: cool compresses; single drop adrenaline 0.1% for extreme chemosis
Seasonal (SAC) and Perennial Allergic Conjunctivitis (PAC)
- SAC (hay fever eyes): spring/summer; tree and grass pollens
- PAC: year-round; house dust mites, animal dander, fungal allergens; milder than SAC
- Symptoms: redness, watering, itching + sneezing, nasal discharge
- Signs: conjunctival hyperaemia, mild papillary reaction, mild chemosis
Treatment stepladder:
- Artificial tears (dilutes allergen)
- Mast cell stabilizers (sodium cromoglicate, nedocromil, lodoxamide) - preventive; need days to take effect
- Topical antihistamines (emedastine, epinastine, levocabastine) - for exacerbations
- Dual-action agents (antihistamine + mast cell stabilizer): azelastine, ketotifen, olopatadine - rapid-acting, very effective
- Short course topical steroids for severe acute episodes
- Allergen immunotherapy for refractory cases
Vernal Keratoconjunctivitis (VKC)
Demographics: Young males (boys <10 years), atopic individuals; predominantly in warm, dry climates (Mediterranean, Middle East, sub-Saharan Africa). Tends to improve after puberty.
Intense itching is the cardinal symptom; also lacrimation, photophobia, thick mucoid discharge.
Two main types:
- Palpebral VKC (upper tarsal plate predominant)
- Limbal VKC (more common in tropical/dark-skinned individuals)
Palpebral Disease Signs:
- Diffuse velvety papillary hypertrophy on superior tarsal plate
- Macropapillae (<1 mm) - flat-topped, polygonal "cobblestones"
- Giant papillae (>1 mm) - adjacent papillae amalgamate; most characteristic
- Mucus deposition between papillae
- Whitish inflammatory infiltrates in intense disease
Limbal Disease Signs:
- Gelatinous limbal conjunctival papillae
- Horner-Trantas dots - transient white cellular collections at apices of limbal papillae (eosinophil/degenerate cell aggregates) - pathognomonic
Corneal Complications (more common with palpebral VKC):
- Superior punctate epithelial erosions with overlying mucus
- Epithelial macroerosions
- Shield ulcer - exposed Bowman membrane coated with calcium phosphate and mucus; serious; resists re-epithelialization → risk of secondary infection
- Subepithelial grey-oval scars
- Pseudogerontoxon - paralimbal band of superficial scarring resembling arcus senilis (after recurrent limbal disease)
- Keratoconus - more common in VKC; partly due to eye rubbing
Treatment:
- Mast cell stabilizers + antihistamines (as for SAC/PAC)
- Topical steroids (short, intensive course; rapid taper) - for acute exacerbations
- Topical ciclosporin A 0.5-2% - steroid-sparing; effective for moderate-severe disease
- Shield ulcer: mechanical debridement, therapeutic soft contact lens, topical steroids, mitomycin C; prompt treatment to prevent bacterial superinfection
- Tacrolimus ointment for lid disease
Atopic Keratoconjunctivitis (AKC)
Demographics: Adults, peak 30-50 years; severe atopic dermatitis. Bilateral. More chronic and severe than VKC.
Hallmarks: Intense itching + severe eyelid skin disease (eczematous lichenified eyelids).
Differences from VKC:
- More severe corneal involvement; may lead to corneal vascularization, opacity, and blindness
- Eyelid disease prominent (in contrast to VKC where lid skin is usually spared)
- Staph blepharitis commonly coexists
- Cataracts (anterior subcapsular - "shield cataract") and keratoconus more common
- Herpes simplex keratitis more common (can be bilateral)
- Progression to corneal scarring, limbal stem cell deficiency
Treatment: As for VKC + aggressive lid hygiene; systemic immunosuppression (ciclosporin, azathioprine, mycophenolate) for severe cases.
Giant Papillary Conjunctivitis (GPC) / Mechanically-Induced Papillary Conjunctivitis
Caused by mechanical trauma from a foreign surface on the upper tarsal plate.
Causes: Contact lenses (most common), ocular prostheses, exposed sutures, filtering blebs.
Signs: Giant papillae (>1 mm) on upper tarsal conjunctiva, mucoid discharge, itching, lens intolerance.
Treatment: Remove/modify the offending surface; mast cell stabilizers; reduce contact lens wear; switch to daily disposable lenses.
6. Cicatrising (Scarring) Conjunctivitides
Mucous Membrane Pemphigoid (MMP) / Ocular Cicatricial Pemphigoid (OCP)
Chronic, progressive, potentially blinding autoimmune blistering disease affecting mucous membranes (and skin in 25%).
Pathogenesis: IgG (± IgA) autoantibodies against basement membrane zone components → subepithelial blistering → scarring.
Ocular Signs (progressive):
- Papillary conjunctivitis, diffuse hyperaemia, subtle fibrosis
- Inferior fornix shortening (forniceal depth measurement important for monitoring)
- Symblepharon - adhesion between palpebral and bulbar conjunctiva
- Ankyloblepharon - adhesion at outer canthus between upper and lower lids
- Goblet cell and accessory lacrimal gland destruction → severe dry eye
- Trichiasis, aberrant lashes, lid margin keratinization
- End-stage: total symblepharon, corneal opacification (limbal stem cell failure)
Systemic features:
- Mucosal involvement: oral blisters most common; oesophageal/laryngeal strictures
- Skin lesions (25%): tense blisters/erosions on head, neck, groin, extremities
Treatment (systemic - mainstay):
- Dapsone - useful first-line for mild-moderate disease (~70% respond); contraindicated in G6PD deficiency
- Methotrexate - for moderate disease
- Cyclophosphamide (with systemic steroids) - for severe/rapidly progressive disease
- Biologic agents (rituximab, IVIg) for refractory cases
- Local: preservative-free lubricants; treat trichiasis/entropion; symblepharon lysis with amniotic membrane transplantation; ultimately limbal stem cell transplantation for corneal opacification
Stevens-Johnson Syndrome (SJS) / Toxic Epidermal Necrolysis (TEN)
Severe mucocutaneous reaction (usually drug-induced; rarely post-infection).
Common drug triggers: Sulfonamides, penicillins, anticonvulsants (carbamazepine, phenytoin), allopurinol, NSAIDs.
Ocular features (acute):
- Pseudomembranous or membranous conjunctivitis
- Corneal epithelial defects, ulceration
- Iritis, episcleritis
Chronic/cicatricial:
- Similar to OCP: symblepharon, trichiasis, dry eye, corneal vascularization and opacity
- Limbal stem cell deficiency
Management: Stop causative drug; systemic steroids (controversial); amniotic membrane transplantation (acute phase) to reduce scarring; long-term cicatricial management as in MMP.
7. Miscellaneous Conjunctival Conditions
Superior Limbic Keratoconjunctivitis (SLK)
Associated with thyroid disease (check thyroid function in all patients).
Signs:
- Hyperaemia of superior bulbar conjunctiva (radial band) - stains with rose Bengal
- Limbal papillary hypertrophy and loss of palisades superiorly
- Redundant superior bulbar conjunctiva folding across the superior limbus
- Superior punctate epithelial erosions + superior filamentary keratitis (1/3 of cases)
- Mild superior pannus
- KCS in ~50%
Treatment: Lubricants (frequent), acetylcysteine 5-10% (for filaments), mast cell stabilizers/steroids, topical ciclosporin, soft contact lens, retinoic acid; surgical (conjunctival resection or cautery) for refractory cases.
Subconjunctival Haemorrhage
- Bleeding under the bulbar conjunctiva; appears bright red
- Usually spontaneous (Valsalva, coughing, hypertension, anticoagulants, trauma)
- Alarming appearance but almost always benign; resolves spontaneously in 2-3 weeks
- Recurrent: check blood pressure, coagulation screen, blood glucose
Conjunctivochalasis
Redundant, loose bulbar conjunctiva (usually inferior) that overrides the lower lid margin → epiphora, foreign body sensation, instability of tear meniscus. More common in elderly. Treatment: lubricants; conjunctival resection/cauterization for severe cases.
Pinguecula
- Yellowish-white amorphous deposit on bulbar conjunctiva, nasal > temporal; does not extend onto the cornea
- UV-related elastotic degenerative change in subepithelial stromal collagen
- Usually asymptomatic; "pingueculitis" if inflamed (treat with topical lubricants/short steroid course)
8. Pterygium
A triangular fibrovascular subepithelial ingrowth of degenerative bulbar conjunctival tissue from the limbus onto the cornea. UV-related. Familial tendency.
Histology: Elastotic degenerative changes in vascularized subepithelial stromal collagen (same as pinguecula). Invades Bowman layer.
Anatomy of a pterygium:
- Cap - avascular halo-like zone at the advancing edge
- Head - apex on cornea
- Body - vascularized triangular base on the bulbar conjunctiva
- Stocker line - linear iron deposition in corneal epithelium anterior to the head (indicates slow growth)
Symptoms:
- Small lesions - often asymptomatic
- Irritation/grittiness (dellen effect at advancing edge)
- Contact lens intolerance
- Astigmatism or visual axis obstruction (advanced lesion)
- Intermittent inflammation
Pseudopterygium: Band of conjunctiva adhering to compromised cornea at its apex. Caused by chemical burns, marginal corneal ulcer, cicatrising conjunctivitis. A probe can pass beneath the apex (distinguishes from true pterygium).
Treatment:
- Observation if small and asymptomatic
- Lubricants, sunglasses (UV protection)
- Surgery: excision + conjunctival autograft (gold standard; lowest recurrence ~5%) or amniotic membrane transplantation
- Adjuvants to reduce recurrence: mitomycin C (intraoperative or postoperative drops); beta-irradiation
- Recurrence is the main problem (bare sclera excision alone = >50% recurrence)
Summary: Key Diagnostic Differentiators
| Feature | Bacterial | Viral | Chlamydial | Allergic |
|---|---|---|---|---|
| Discharge | Mucopurulent | Watery | Mucopurulent | Watery/mucoid |
| Itching | Absent | Mild | Absent | Hallmark |
| Follicles | No | Yes | Yes (inferior fornix) | No (papillae) |
| Papillae | Mild | Mild | Mild | Giant papillae (VKC/GPC) |
| Lymphadenopathy | Absent (except GC) | Present | Present | Absent |
| Corneal signs | PEE (gonococcal: ulcer) | SEI (EKC) | Pannus, infiltrates | Shield ulcer (VKC) |
| Onset | Acute bilateral | Acute, unilateral → bilateral | Subacute | Seasonal/perennial |
Itching = allergy. Follicles = viral or chlamydial. Preauricular node = viral or chlamydial. Hyperacute purulent = gonococcal (emergency).
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., Chapter 6 (Conjunctiva) | The Wills Eye Manual, Sections 5.1, 5.2, 5.8, 6.3, Differential Diagnosis Tables
Cornea opthalmology
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content across all corneal topics. Let me compile the full review.
The Cornea - Comprehensive Ophthalmology Review
Kanski's Clinical Ophthalmology 10th ed. & The Wills Eye Manual
1. Anatomy & Physiology
The cornea is the transparent, avascular anterior window of the eye. It provides approximately 2/3 of the eye's total refractive power (~43 D of the ~60 D total). Its clarity depends on:
- Regular lamellar arrangement of collagen fibrils (spacing maintained by proteoglycans)
- Relative dehydration (maintained by endothelial pump)
- Avascularity
- Intact epithelial barrier
Layers (anterior to posterior)
| Layer | Details |
|---|---|
| Epithelium | Non-keratinizing stratified squamous; 5-6 cell layers; renewed every 7-10 days from limbal stem cells (palisades of Vogt) |
| Bowman membrane | Acellular; can't regenerate (scars if damaged) |
| Stroma | ~90% of corneal thickness; collagen lamellae + keratocytes + proteoglycans (keratan/chondroitin sulfate) |
| Descemet membrane | Basement membrane of endothelium; thickens with age; guttata = abnormal excrescences |
| Endothelium | Single layer; ~2500 cells/mm² at birth; cannot regenerate; drives fluid out of stroma (ionic pump); critical for corneal clarity |
Normal central corneal thickness: ~540 μm
Corneal sensation: V1 (ophthalmic branch of trigeminal) via nasociliary nerve → long ciliary nerves. Most sensitive tissue in the body. Reduced in herpes keratitis, neurotrophic disease, contact lens wearers.
2. Signs of Corneal Disease
Staining
- Fluorescein: Stains areas of epithelial defect (fills gaps in tight junctions; stains intercellular spaces)
- Rose Bengal: Stains devitalized/dead cells and mucus; better for filaments, dendrites, and keratoconjunctivitis sicca
Slit-lamp signs
- Keratic precipitates (KP): Inflammatory cells on endothelium
- Fine/stellate (non-granulomatous uveitis), mutton-fat/large/greasy (granulomatous - sarcoid, TB, HSV)
- Corneal oedema: Stromal haze/thickening; epithelial bullae (advanced)
- Vascularization: Superficial (pannus - anterior stroma) or deep (interstitial keratitis)
- Infiltrate: Cellular recruitment to stroma; loss of normal lamellar clarity
- Descemetocoele: Herniation of Descemet membrane through stromal thinning; surgical emergency (risk of perforation)
3. Dry Eye Syndrome (Keratoconjunctivitis Sicca - KCS)
Types
- Aqueous-deficient dry eye: Reduced tear production (Sjögren's syndrome, lacrimal gland disease, Riley-Day syndrome)
- Evaporative dry eye: Meibomian gland dysfunction (most common), blepharitis, lid abnormalities, contact lens wear, low blink rate
Symptoms
Burning, grittiness, foreign body sensation, paradoxical tearing, worse at end of day, worse in wind/low humidity.
Corneal Signs
- Punctate epithelial erosions (PEE) - stain with fluorescein (interpalpebral distribution)
- Filaments - strands of mucus + shed epithelial cells, attached at one end; stain well with rose Bengal
- Mucous plaques - semi-transparent grey-white elevated lesions
- Thin/absent marginal tear meniscus
- Severe complications: epithelial breakdown, stromal melting, perforation, bacterial keratitis
Investigations
- Tear break-up time (BUT): Normal >10 sec; <5 sec = abnormal (measure with fluorescein)
- Schirmer's test: Filter paper strip placed at lower lid lateral fornix
- Type I (no anaesthetic): measures basal + reflex; ≥10 mm in 5 min = normal; <5 mm = abnormal
- Type II (with topical anaesthetic): basal secretion only
- Tear osmolarity (most sensitive/specific): >308 mOsm/L in one eye, or >8 mOsm/L difference between eyes = abnormal
- Rose Bengal / lissamine green staining - interpalpebral staining pattern (Van Bijsterveld score)
- MMP-9 point-of-care test - elevated in dry eye inflammation
Treatment
- Artificial tears (preservative-free if using >4×/day)
- Lubricating gels/ointment (nighttime)
- Treat underlying blepharitis/MGD (warm compresses, lid hygiene, doxycycline)
- Topical ciclosporin 0.05-0.1% (Restasis/Cequa) - reduces inflammation; improves tear production
- Lifitegrast (LFA-1 integrin antagonist) - anti-inflammatory
- Punctal occlusion (plugs or cautery) - retains tears
- Bandage contact lens for filamentary keratitis
- Autologous serum drops for severe/refractory cases
- Moisture chamber spectacles, humidifiers
4. Bacterial Keratitis (Corneal Ulcer)
Pathogenesis & Risk Factors
Bacterial keratitis requires compromise of ocular defences. Exception: N. gonorrhoeae, N. meningitidis, C. diphtheriae, H. influenzae can penetrate intact epithelium.
Common organisms:
| Organism | Features |
|---|---|
| Pseudomonas aeruginosa | Gram-negative rod; most aggressive; >60% of contact lens-related keratitis; rapid melting |
| Staphylococcus aureus | Gram-positive; focal, well-defined, yellow-white infiltrate |
| Streptococcus spp. | Gram-positive; often aggressive |
| Moraxella | Gram-negative; indolent; inferior cornea; malnourished/alcoholic patients |
Risk factors:
- Contact lens wear (most important, especially extended-wear soft lenses)
- Trauma (including LASIK)
- Ocular surface disease (dry eye, lid disease, bullous keratopathy)
- Previous corneal disease
- Topical steroid use
- Immunocompromise
- Exposure keratopathy
Clinical Features
Symptoms: Acute pain, photophobia, redness, discharge, decreased VA. Rapid onset.
Signs:
- Epithelial defect (ulcer) overlying a stromal infiltrate
- Dense white-yellow stromal infiltrate with surrounding haze
- Stromal oedema, Descemet folds
- Anterior uveitis ± hypopyon (sterile pus in anterior chamber)
- Plaque-like KPs
- Chemosis and eyelid swelling (moderate-severe)
- Descemetocoele formation and perforation (especially Pseudomonas)
- Scleritis (severe perilimbal infection)
Investigations
Corneal scraping is indicated for ulcers that are:
-
2 mm in size
- Middle to deep stroma involvement
- Within visual axis
- Chronic or atypical appearance
- Non-responsive to initial treatment
Scraping technique:
- Non-preserved topical anaesthetic (proxymetacaine 0.5%)
- Sterile No. 11 blade, 20-21G needle tip, or Kimura spatula
- Scrape margins and base
- Plate directly onto culture media
- Send smears for Gram stain, Giemsa stain, KOH (fungal), Ziehl-Neelsen (acid-fast)
- Gram stain - most rapid guide to initial therapy
Culture media: Blood and chocolate agars (bacterial), Sabouraud dextrose agar (fungal), non-nutrient agar with E. coli overlay (Acanthamoeba), thioglycolate broth (anaerobic).
Treatment
Topical antibiotic therapy (high frequency, reducing as improvement noted):
- Initial: hourly day and night for 24-48 hours, then taper
- Fluoroquinolone monotherapy (ciprofloxacin, ofloxacin, moxifloxacin, gatifloxacin) - preferred empirical treatment
- Duotherapy (cephalosporin + aminoglycoside) for aggressive disease
Antibiotic table:
| Organism | Agent | Concentration |
|---|---|---|
| Empirical | Fluoroquinolone monotherapy | varies |
| Empirical (aggressive) | Cefuroxime + fortified gentamicin | 5% + 1.5% |
| Gram-positive cocci | Cefuroxime / vancomycin | 0.3% / 5% |
| Gram-negative rods | Fortified gentamicin / fluoroquinolone | 1.5% |
| Gram-negative cocci | Ceftriaxone | 5% |
| Mycobacteria | Amikacin + clarithromycin | 2% + 1% |
| Nocardia | Amikacin + trimethoprim-sulfamethoxazole | 2% |
Note: Ciprofloxacin drops cause white corneal precipitates (drug crystallization) that can delay epithelial healing.
Adjunctive measures:
- Cycloplegia (atropine) for pain + prevent posterior synechiae
- IOP control if raised
- Bandage contact lens or tissue glue for imminent perforation
- Tarsorrhaphy for exposure keratopathy
- Amniotic membrane graft for persistent epithelial defect
- Steroids are generally contraindicated initially (may worsen bacterial keratitis); may be considered once infection controlled to reduce scarring
5. Herpes Simplex Keratitis (HSK)
Most common infectious cause of corneal blindness in developed countries. ~10% of those with any history of HSK will eventually have VA <6/60.
HSV Biology
- Enveloped double-stranded DNA virus; two subtypes
- HSV-1: Above the waist (face, lips, eyes)
- HSV-2: Venereally acquired (genital); rarely ocular (neonatal transmission)
- Latency in trigeminal ganglion (for ocular HSV)
- Reactivation triggered by: fever, UV, trauma, immunosuppression, menstruation, emotional stress
Primary HSV Infection
- Usually childhood; subclinical (or mild fever + URTI)
- May cause unilateral follicular conjunctivitis + blepharitis + vesicular lid lesions
- Dendritic corneal ulcers can occur even in the presence of maternal antibodies
Recurrent HSK - Forms
(A) Epithelial (Dendritic) Keratitis
The classic presentation.
Signs in chronological order:
- Reduced VA
- Swollen opaque epithelial cells in coarse punctate or stellate pattern
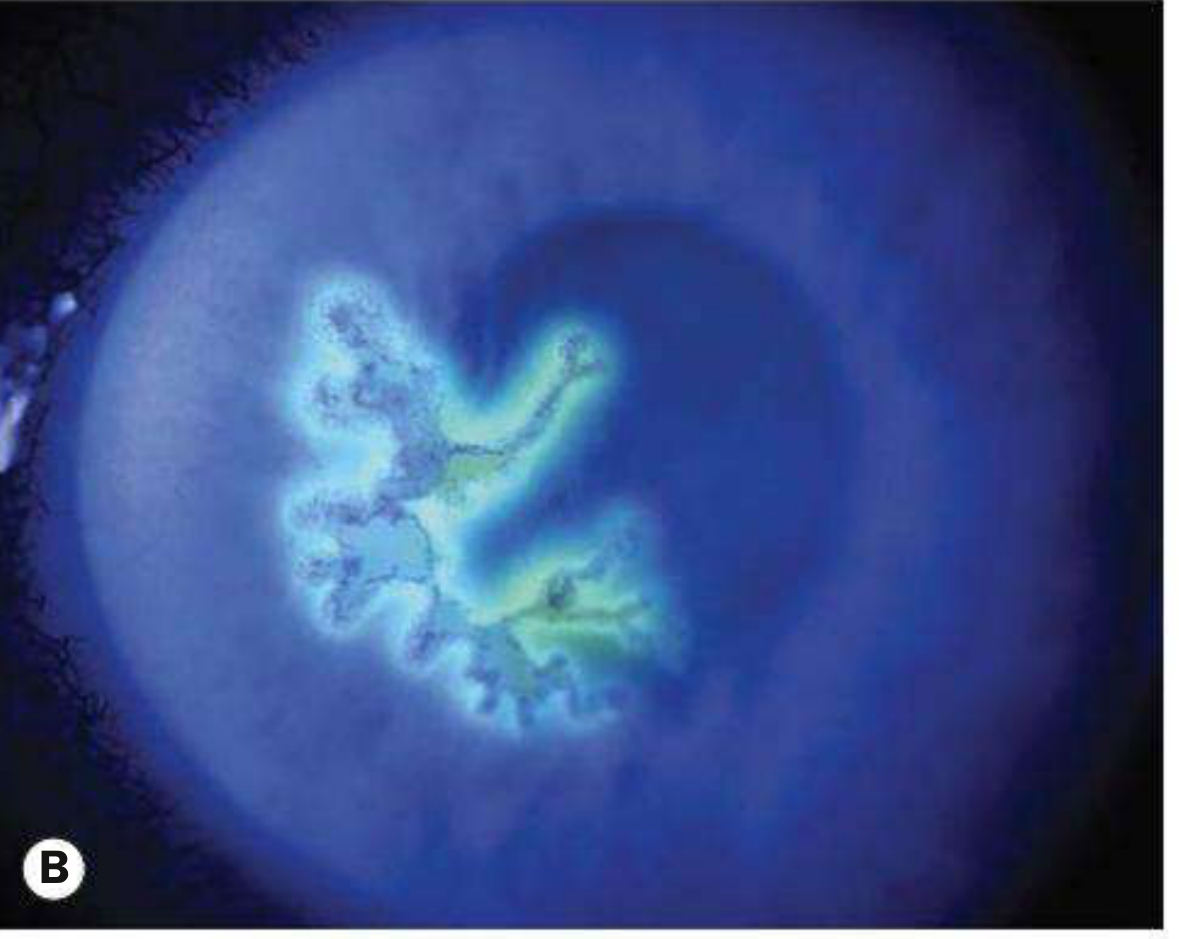
- Central desquamation → linear-branching (dendritic) ulcer with characteristic terminal buds
- Ulcer bed stains with fluorescein; margin cells (virus-laden) stain with rose Bengal
- Reduced corneal sensation (highly characteristic)
- Mild subepithelial haze
- Steroids (inadvertent): enlargement to geographic/"amoeboid" ulcer
Key: Geographic ulcer = HSK treated with steroids alone without antiviral cover.
Treatment:
- Topical aciclovir 3% ointment 5× daily for 10-14 days, OR
- Ganciclovir 0.15% gel 5× daily (better tolerated)
- Do NOT use steroids alone (will enlarge ulcer)
- Debridement of infected epithelium (historical; less used now)
(B) Disciform (Endothelial/Stromal) Keratitis
Immune-mediated reaction to viral antigen in the stroma. Not active viral replication.
Signs:
- Central disc of epithelial + stromal oedema (disciform appearance)
- Descemet membrane folds (Vogt's striae)
- Wessely immune ring - deep stromal haze ring surrounding the disc (viral antigen + antibody immune complex)
- KPs on endothelium beneath the disc
- Reduced corneal sensation
- Raised IOP (not uncommon)
- Healed lesions: faint ring of stromal/subepithelial opacification + thinning
Treatment:
- Topical steroids (prednisolone 1% or dexamethasone 0.1%) + antiviral cover (topical aciclovir or oral aciclovir)
- Monitor IOP carefully
- Steroid intensity kept to minimum - taper over ≥4 weeks
- Long-term low-dose steroid (prednisolone 0.5% once daily) often needed to maintain remission
- Oral aciclovir (400 mg twice daily) or valaciclovir (500 mg once daily) for prophylaxis of recurrence
(C) Necrotising Stromal Keratitis
Rare; active viral replication in stroma → white necrotic infiltrate; severe inflammation; scarring + vascularization. High risk of perforation. Needs aggressive topical + systemic antivirals.
(D) Neurotrophic Keratopathy
Result of corneal denervation from repeated HSV episodes.
- Impaired blink reflex + reduced tear production → epithelial breakdown
- Persistent oval epithelial defect with smooth rolled edges (typically inferior third of cornea)
- Treatment: aggressive lubrication, bandage contact lens, amniotic membrane, tarsorrhaphy, cenegermin (recombinant nerve growth factor drops)
(E) Meta-herpetic (Post-herpetic) Keratopathy
Non-infectious stromal scarring + vascularization after recurrent disease. Worsens with each episode.
HEDS Study - Key Evidence
- Oral aciclovir prophylaxis (400 mg twice daily) reduces recurrent HSK by 45%
- Topical steroids (with antiviral cover) benefit stromal (immune) keratitis
- Topical steroids do NOT benefit epithelial (active viral) keratitis
6. Fungal Keratitis
Risk Factors
- Trauma with vegetable/organic matter (filamentous fungi - Fusarium, Aspergillus)
- Contact lens wear (Fusarium, Candida)
- Topical steroids or antibiotics (disrupts flora)
- Immunocompromise (Candida - more common in endogenous/systemic spread)
- Tropical/agricultural regions (filamentous fungi more common)
Organisms
- Filamentous (moulds): Fusarium spp., Aspergillus spp. - associated with trauma
- Yeast: Candida spp. - associated with immunocompromise, chronic disease, contact lenses
Signs
- Typically slower onset than bacterial keratitis
- Feathery/hyphate margins (filamentous fungi)
- Satellite lesions (hyphal extensions)
- Dry, rough, raised infiltrate (unlike bacterial - which is smoother)
- Endothelial plaque
- Immune ring may develop
- Hypopyon
Investigations
- Corneal scrapings: KOH preparation (dissolves tissue; hyphae visible); Calcofluor white (fluoresces hyphae); Gram stain; Giemsa stain; cultures on Sabouraud dextrose agar (fungal media)
- Confocal microscopy (in vivo - non-invasive)
- PCR
Treatment
- Natamycin 5% (first-line for filamentous, especially Fusarium)
- Voriconazole 1% topical (excellent filamentous and Candida coverage; better corneal penetration; first-line in many centres)
- Amphotericin B 0.15% (first-line for Candida)
- Oral voriconazole for deep/severe keratitis or scleritis
- Steroids are contraindicated in active fungal keratitis
- Treatment duration typically 6-12 weeks (much longer than bacterial)
7. Acanthamoeba Keratitis
A protozoal infection with particularly devastating potential. Strongly associated with contact lens wear (especially swimming in lenses).
Organism: Acanthamoeba spp. - free-living amoeba found in soil, water, air; two forms: active trophozoite and resistant cyst (can withstand disinfectants).
Signs
- Severe, disproportionate pain (often out of proportion to clinical signs) - classic feature
- Slow insidious onset
- Perineural infiltrate (radial keratoneuritis) - pathognomonic; linear infiltrates tracking along corneal nerves
- Ring infiltrate (immune ring) - characteristic late sign
- Pseudodendrites (can mimic HSK dendrites but no terminal buds; stain poorly)
- Uveitis, scleritis in severe cases
Diagnosis
- Confocal microscopy - can identify cysts in vivo (doubles/trefoils of bright round structures)
- Corneal scrapings plated on non-nutrient agar with E. coli overlay (amoeba feed on bacteria)
- PCR
Treatment
- Polyhexamethylene biguanide (PHMB) 0.02% + propamidine isethionate (Brolene) 0.1% - cornerstone; hourly initially
- Or chlorhexidine 0.02% (alternative biguanide)
- Treatment for at least 12 months (to eliminate cysts)
- Steroids generally avoided initially; may be used cautiously for severe inflammation after antiamoebics started
- Corneal graft if medical treatment fails
8. Keratoconus
Key Facts
- Progressive central/paracentral corneal stromal thinning + apical protrusion + irregular astigmatism
- Prevalence: 0.1-0.2%
- Onset: teens/twenties
- Males slightly more affected
- Bilateral (eventually in almost all; initially may present as unilateral)
- ~50% of normal fellow eyes progress to KC within 16 years
- Only ~10% have a positive family history; proposed AD with incomplete penetrance
Associations
- Systemic: Down syndrome, Ehlers-Danlos syndrome, Marfan syndrome, osteogenesis imperfecta
- Ocular: Atopy (VKC, eczema), asthma - persistent eye rubbing is a key risk factor; blue sclera, aniridia, Leber congenital amaurosis, retinitis pigmentosa
Diagnosis
Symptoms: Progressive unilateral (early) myopia + irregular astigmatism; monocular diplopia.
Clinical signs:
- Oil-droplet reflex on direct ophthalmoscopy at arm's length (or ~50 cm)
- Scissor reflex on retinoscopy
- Vogt's striae - fine vertical lines in deep stroma (Descemet folds from stress)
- Fleischer ring - epithelial iron deposition at base of cone (best seen with cobalt blue filter)
- Munson's sign - V-shaped deformity of lower lid on downgaze (advanced)
- Rizzuti's sign - conical reflection on nasal cornea from temporal penlight
- Corneal thinning and protrusion on slit lamp
- Corneal sensation reduced
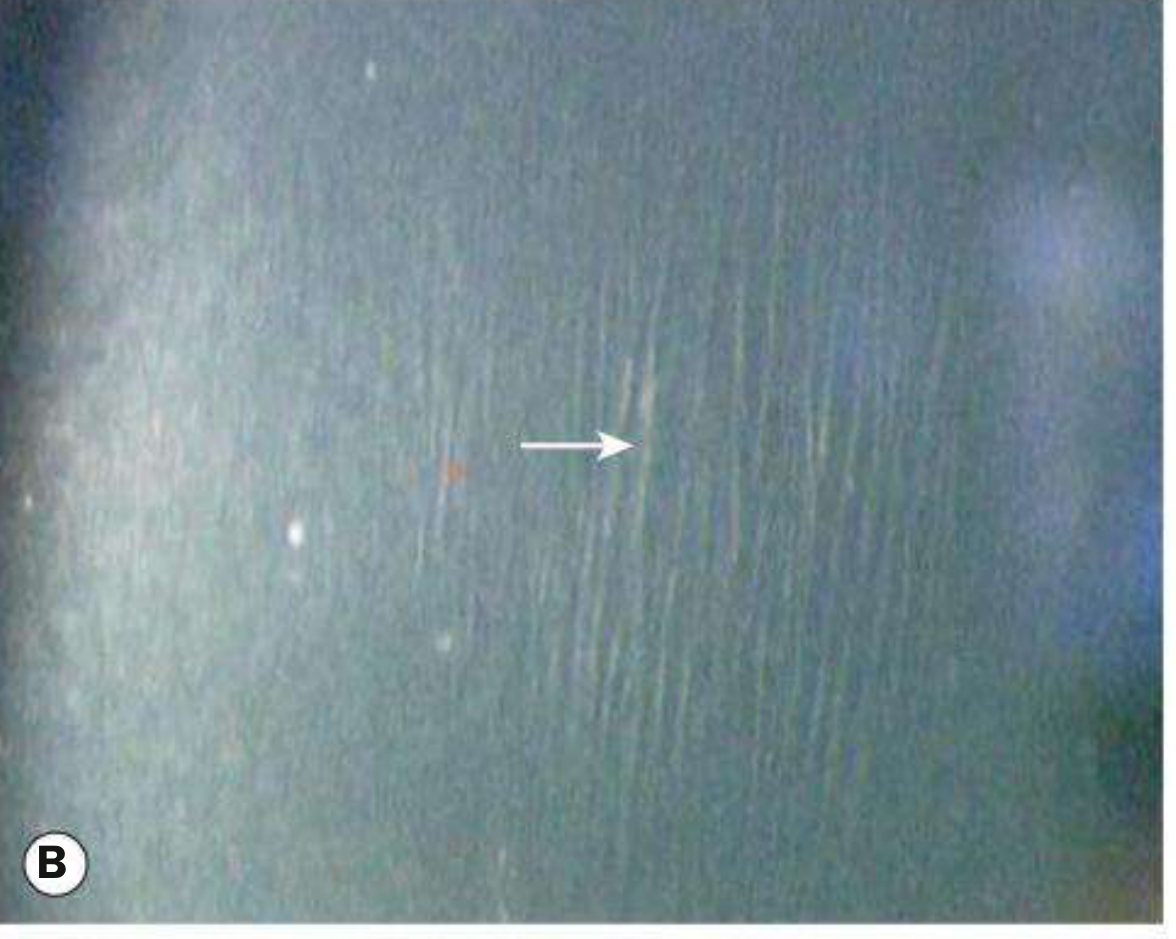
Imaging:
- Corneal topography/tomography (Pentacam Scheimpflug) - shows inferior steepening, asymmetric bowtie pattern; essential for diagnosis and monitoring
- Keratometry grading: Mild (<48 D), Moderate (48-54 D), Severe (>54 D)
- Pachymetry: thinning at apex
Acute Hydrops
Rupture of Descemet membrane → aqueous floods stroma → acute severe corneal oedema.
Signs: Sudden dramatic decrease in vision + pain; dense white opaque area of localised corneal oedema (may be diffuse in severe cases). Munson's sign prominent.
Management: Conservative (hypertonic saline 5%, bandage contact lens, cycloplegia); resolves over months with variable residual scarring. DALK contraindicated after hydrops (Descemet membrane discontinuity).
Treatment
| Stage | Management |
|---|---|
| Mild | Spectacle correction; contact lenses (rigid gas permeable lenses) |
| Progressive | Corneal collagen cross-linking (CXL) - riboflavin (B2) + UV-A irradiation; halts/reverses ectasia; performed when progression documented |
| Moderate | Intracorneal ring segment implants (ICRS/Intacs) - improve contact lens tolerance; can be combined with CXL |
| Severe | Deep anterior lamellar keratoplasty (DALK) or penetrating keratoplasty (PK) |
LASIK is absolutely contraindicated in keratoconus. Screen all refractive surgery candidates for KC first.
Pellucid Marginal Degeneration (PMD)
- Inferior crescentic corneal thinning (4-8 o'clock position) with protrusion above the thinning
- "Against-the-rule" astigmatism; "crab claw" or "butterfly" topography pattern
- Non-inflammatory; similar associations to KC
- Treatment: contact lenses; surgery for advanced cases
9. Corneal Dystrophies
General principles:
- Usually bilateral
- Primarily affect one layer of the cornea
- Slowly progressive
- Most have identified genetic mutations
- Classified by anatomical layer (IC3D classification)
Epithelial Dystrophies
Cogan (Epithelial Basement Membrane / Map-Dot-Fingerprint) Dystrophy
- Most commonly sporadic (degenerative); rare AD familial form (TGFBI gene)
- Hallmark: recurrent corneal erosions (painful, typically on waking)
- Signs on retroillumination:
- Dot-like/microcystic lesions
- Subepithelial map-like patterns surrounded by faint haze
- Fingerprint-like whorled lines
- Bleb-like/pebbled glass pattern
- Treatment: artificial tears, hypertonic saline, lubricating ointment at bedtime; epithelial debridement; anterior stromal micropuncture; excimer laser PTK
Meesmann Epithelial Dystrophy
- Rare; AD; mutations in corneal epithelial keratins (KRT3, KRT12)
- Myriad tiny uniform intraepithelial cysts centrally (sparing limbus)
- Usually asymptomatic; mild recurrent erosions in some
Bowman Layer Dystrophies
Reis-Bücklers Dystrophy (GCD type 3)
- AD; TGFBI gene
- Histology: replacement of Bowman layer by connective tissue bands
- Severe recurrent erosions in childhood; visual impairment
- Signs: grey-white geographic subepithelial opacities, dense centrally; reticular pattern with age
- Treatment: excimer PTK; keratoplasty if severe
Thiel-Behnke Dystrophy (CBD2 / Honeycomb dystrophy)
- AD; TGFBI gene; "curly fibres" on electron microscopy
- Milder than Reis-Bücklers; honeycomb/ring network of subepithelial opacities
Stromal Dystrophies
| Dystrophy | Gene | Inheritance | Histology (Stain) | Key Features |
|---|---|---|---|---|
| Lattice (TGFB1 type) | TGFB1 | AD | Amyloid (Congo red +; green birefringence) | Fine refractile lattice lines; peripheral sparing; recurrent erosions (1st decade) |
| Lattice type 2 (Meretoja/gelsolin) | GSN | AD | Amyloid | Systemic: cranial nerve palsies, skin laxity, renal; sparse lattice lines spreading from periphery |
| Granular type 1 (classic) | TGFB1 | AD | Hyaline (Masson trichrome - bright red) | Discrete white crumb-like/sugar-granule central deposits; clear stroma between; glare + photophobia |
| Granular type 2 (Avellino) | TGFB1 | AD | Hyaline + amyloid (combined) | Stellate/annular lesions; refractive surgery contraindicated (worsens) |
| Macular | CHST6 | AR | Glycosaminoglycans (Alcian blue; colloidal iron) | Dense ill-defined grey-white spots; extend to limbus; early visual loss; early erosions; corneal thinning |
| Schnyder (crystalline) | UBIAD1 | AD | Phospholipid + cholesterol deposits | Central haze + crystals; associated systemic dyslipidaemia; arcus; genu valgum |
Descemet Membrane & Endothelial Dystrophies
Fuchs Endothelial Corneal Dystrophy (FECD)
- Most important endothelial dystrophy
- Bilateral accelerated endothelial cell loss
- More common in women; associated with slightly increased glaucoma prevalence
- Genetic: mostly sporadic; AD; TCF4 gene (most cases); COL8A2 (early-onset variant)
Signs (progressive):
- Cornea guttata - irregular warts/excrescences on Descemet membrane secreted by abnormal endothelial cells
- Specular microscopy: tiny dark spots → "beaten metal" appearance of endothelium
- Blurred vision, worse in the morning (nocturnal corneal oedema; dries during waking hours)
- Central stromal oedema (thickening on pachymetry)
- Epithelial bullae → bullous keratopathy (painful blisters; rupture = acute severe pain)
- Subepithelial scarring + peripheral vascularization (end-stage)
Treatment:
- Conservative: hypertonic NaCl 5% drops/ointment; reduce IOP; hair dryer (corneal dehydration)
- Ruptured bullae: bandage contact lens, cycloplegia, antibiotic ointment, anterior stromal puncture
- Definitive: DMEK (Descemet Membrane Endothelial Keratoplasty) or DSAEK (DSAEK = Descemet Stripping Automated Endothelial Keratoplasty) - posterior lamellar transplantation; or PKP (penetrating keratoplasty)
- Promising: topical Rho-kinase inhibitor + prior transcorneal cryotherapy → stimulates endothelial proliferation
- If cataract surgery needed: consider triple procedure (phaco + IOL + DSAEK) to avoid repeated surgery
Posterior Polymorphous Corneal Dystrophy (PPCD)
- AD; usually asymptomatic
- Vesicular/band lesions on posterior Descemet; some develop corneal oedema
- Association with glaucoma; may have iris-angle abnormalities
10. Corneal Degenerations (Non-dystrophic)
Arcus Senilis (Corneal Arcus)
- Peripheral stromal lipid deposition; separated from limbus by clear zone (lucid interval)
- In elderly: normal (arcus senilis); in young patients (<50): arcus juvenilis → screen for hyperlipidaemia (familial hypercholesterolaemia)
Band Keratopathy
- Calcium deposition in Bowman layer and superficial stroma within interpalpebral fissure
- Grey-white horizontal band with peripheral "Swiss cheese" holes (corneal nerves pass through)
- Causes: chronic uveitis (especially juvenile idiopathic arthritis), hyperparathyroidism, hypercalcaemia, chronic corneal disease, renal failure, sarcoidosis
- Treatment: EDTA chelation (topical 0.35-1.7% disodium EDTA with epithelial debridement); excimer laser PTK
Corneal Deposits
| Deposit | Location | Cause |
|---|---|---|
| Amiodarone (vortex keratopathy) | Epithelium - whorl (verticillata) pattern | Amiodarone, chloroquine, hydroxychloroquine, tamoxifen |
| Kayser-Fleischer ring | Descemet membrane (periphery); brown/green ring | Wilson's disease (copper deposition) |
| Cystine crystals | Stroma | Cystinosis |
| Hudson-Stähli line | Junction of lower and middle thirds (interpalpebral) | Normal aging; iron deposition |
| Fleischer ring | Around base of keratoconus cone | KC (iron) |
| Stocker line | Anterior to pterygium head | Iron |
| Ferry's line | Around filtering bleb | Iron |
11. Peripheral Corneal Disorders
Peripheral Ulcerative Keratitis (PUK)
- Crescentic peripheral stromal thinning with overlying epithelial defect
- Associated with systemic vasculitis (rheumatoid arthritis most common - Mooren's ulcer is idiopathic; also GPA, SLE, PAN)
- Treat systemic disease; immunosuppression (systemic steroids, methotrexate, cyclophosphamide, rituximab)
Marginal Keratitis (Catarrhal Ulcer)
- Peripheral infiltrates/ulcers at 2, 4, 8, 10 o'clock with clear interval between lesion and limbus
- Immune-mediated (staphylococcal hypersensitivity) - not infectious
- Treat underlying blepharitis + short course topical steroid-antibiotic combination
Summary: Key Differentiating Points
| Condition | Key Sign | Reduced Sensation? | Staining |
|---|---|---|---|
| Bacterial keratitis | Hypopyon, mucopurulent | Mild | Fluorescein (ulcer) |
| HSV epithelial | Dendritic ulcer with terminal buds | Yes | Fluorescein (bed), Rose Bengal (margins) |
| HSV disciform | Disc oedema + Wessely ring | Yes | No ulcer |
| Acanthamoeba | Radial keratoneuritis; severe pain | Variable | Pseudodendrites |
| Fungal | Feathery margins; satellite lesions | No | - |
| Keratoconus | Oil droplet reflex; Fleischer ring | No | - |
| Fuchs dystrophy | Cornea guttata; worse mornings | No | - |
| Band keratopathy | Horizontal grey band with holes | No | - |
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed., Chapter 7 (Cornea) | The Wills Eye Manual, Sections 4.11-4.15 (Keratitis), Chapter 5 (Corneal/Conjunctival Findings)
This is a shared conversation. Sign in to Orris to start your own chat.