Indications for Transfusion i. Anemia, thrombocytopenia, coagulopathy ii. Massive transfusion protocol
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Finding Sources
I now have everything I need for a thorough, well-cited answer. Let me compile it.
Indications for Transfusion
i. Anemia - Red Blood Cell (RBC) Transfusion
General Principle
RBC transfusions are used to restore oxygen-carrying capacity when anemia is symptomatic or poses physiologic risk. The decision to transfuse should never be based on a single hemoglobin (Hb) trigger alone - the patient's clinical status, symptoms, and comorbidities must be integrated.
- Goldman-Cecil Medicine, p. 2990: "RBC transfusions are used to treat anemia when patients require increased oxygen carrying capacity, based on their individual clinical status and coexisting medical conditions. In an average adult, one RBC component (unit) should increase the hemoglobin by about 1 g/dL and the hematocrit by about 3%."
Restrictive vs Liberal Strategy
Approximately 50 RCTs have directly compared restrictive versus liberal transfusion thresholds:
| Clinical Setting | Transfusion Threshold |
|---|---|
| Hemodynamically stable critically ill patients | Hb < 7.0 g/dL (restrictive) |
| Acute coronary syndrome / acute MI | Hb < 8.0 g/dL (higher threshold) |
| Symptomatic anemia (regardless of Hb) | Transfuse based on symptoms |
| Hemorrhagic shock / hemodynamic instability | Transfuse regardless of Hb level |
- Mulholland & Greenfield's Surgery: "A 'restrictive' strategy (transfuse when Hb <7 g/dL) is as effective as a 'liberal' strategy (transfuse when Hb <10 g/dL) in critically ill patients with hemodynamically stable anemia, except possibly in patients with acute myocardial ischemia."
- In the absence of acute hemorrhage, RBC transfusion should be given as single units, reassessing before ordering a second unit.
- RBC transfusion should not be viewed as an absolute method to improve tissue oxygen consumption.
Compatible Diluents for PRBCs
Solutions compatible with packed red cells include 0.9% saline, 5% dextrose in 0.45% or 0.9% saline, and Normosol-R (pH 7.4). Lactated Ringer's is not recommended as a carrier due to calcium content that may promote clotting. - Miller's Anesthesia, 10e
ii. Thrombocytopenia - Platelet Transfusion
Prophylactic Thresholds (no active bleeding)
| Indication | Platelet Count Threshold |
|---|---|
| Hospitalized patients with therapy-induced hypoproliferative thrombocytopenia | < 10,000/μL |
| Febrile/septic patient, or minor procedures (e.g., central line placement) | < 20,000/μL |
| Elective surgery, lumbar puncture, invasive procedure, or active bleeding | < 50,000/μL |
| Neurosurgery or CNS bleeding | < 100,000/μL |
- Goldman-Cecil Medicine (Evidence-Based Transfusion Triggers Table 162-4)
Therapeutic Platelet Transfusion
- Patients with platelet count < 50,000/μL who are actively bleeding should receive platelets.
- After cardiac surgery with cardiopulmonary bypass and perioperative bleeding, transfuse if thrombocytopenic or if platelet dysfunction is evident.
- Platelet transfusion is NOT recommended for intracranial hemorrhage in patients on antiplatelet therapy (risk of harm outweighs benefit).
- Spontaneous bleeding rarely occurs if platelet count > 10,000-20,000/mm³; excessive bleeding is uncommon when count exceeds 50,000/mm³ even with surgery/trauma. - Roberts & Hedges' Clinical Procedures in Emergency Medicine
Dosing
- Typical adult dose: 1 apheresis unit or 4-6 pooled whole blood-derived concentrates (~3 × 10¹¹ platelets)
- Expected rise: 30,000-60,000/μL per dose
- Individual random-donor unit: raises count by ~5,000-10,000/mm³
- Assess response with a platelet count 15-60 minutes post-transfusion; corrected count increment (CCI) > 7.5 at 1 hour is acceptable
iii. Coagulopathy - Plasma and Cryoprecipitate
Fresh Frozen Plasma (FFP)
| Indication | Details |
|---|---|
| Massive transfusion | Plasma : RBC ratio of 1:2 (minimum) |
| INR > 2.0 prior to invasive procedure | Give minimum 4 units to correct elevated INR (note: impossible to achieve INR < 1.5 with FFP alone) |
| Plasma exchange for TTP | Replacement fluid |
- Dose: 15 mL/kg (~1000 mL or 4 units in a 70 kg patient)
- Effect: Each unit raises all coagulation factors by 2-3% in average adults; 10-15 mL/kg increases factor levels by ~20%
- ABO compatibility desirable but not required in emergencies; Rh compatibility never required
- Allow ~45-60 minutes thaw time - Roberts & Hedges' Clinical Procedures in Emergency Medicine
Cryoprecipitate
| Indication | Threshold |
|---|---|
| Hypofibrinogenemia with bleeding | Fibrinogen < 150 mg/dL (some guidelines < 100 mg/dL) |
| Fibrinolytic-induced bleeding | 10-12 bags |
| Factor VIII deficiency (when specific factor unavailable) | 1 bag/5 kg |
- Dose: 10-20 bags depending on indication
- Each unit raises fibrinogen by ~7 mg/dL
- Contains: fibrinogen, Factor VIII, vWF, Factor XIII, fibronectin
- Available in ~20 minutes - Goldman-Cecil Medicine, Roberts & Hedges
iv. Massive Transfusion Protocol (MTP)
Definition
Massive transfusion is classically defined as transfusion of ≥ 10 units of RBCs within 24 hours (or ≥ 4 units within 1 hour with ongoing hemorrhage). MTP is a pre-established hospital system to rapidly deliver blood products in a fixed ratio for life-threatening hemorrhage, typically in trauma.
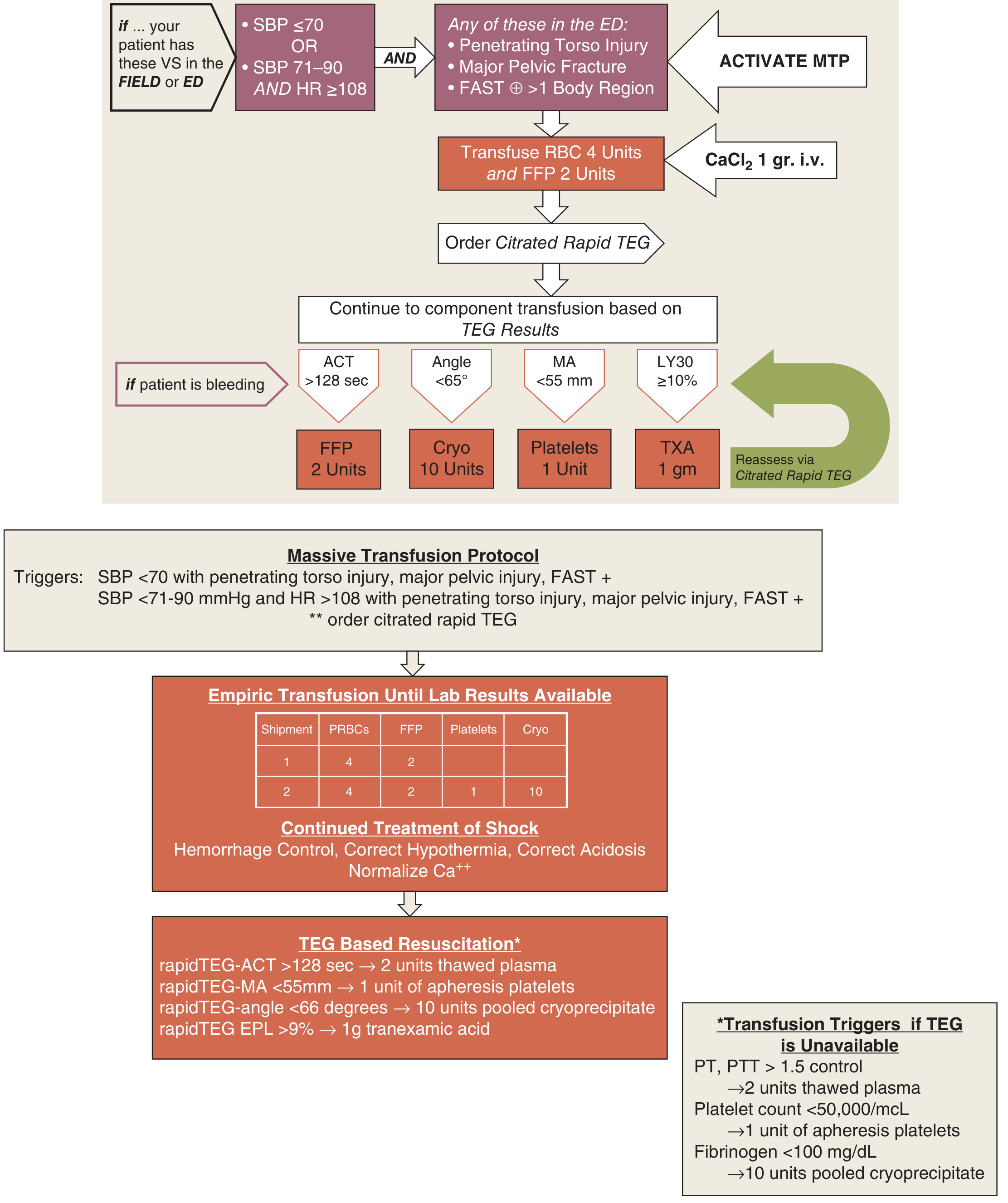
Activation Triggers (Denver Health / Schwartz's Surgery model)
Activate MTP if the patient in the field or ED has:
- SBP ≤ 70 mmHg, OR
- SBP 71-90 mmHg AND HR ≥ 108
...combined with any of:
- Penetrating torso injury
- Major pelvic fracture
- FAST positive in > 1 body region
Empiric Initial Transfusion
Upon activation:
- Transfuse: 4 units RBC + 2 units FFP immediately
- Administer CaCl₂ 1 g IV (to counteract citrate-induced hypocalcemia from massive transfusion)
- Order Citrated Rapid TEG (thromboelastography)
Component Ratios (Empiric Cooler-Based Approach)
Per Sabiston's Textbook of Surgery, when whole blood is unavailable:
- Cooler 1: 4 units type-O RBCs + 4 units AB or A plasma
- Cooler 2 onward: RBC : Plasma : Platelets in a 1:1:1 ratio
- O-negative blood reserved for females of childbearing age when blood type is unknown or Rh-negative
The preferred approach in centers with availability is low-titer O whole blood (LTOWB), which simplifies logistics and reduces dilutional coagulopathy.
TEG-Guided Resuscitation (Goal-Directed)
Once TEG results are available, component therapy is guided by specific parameters:
| TEG Parameter | Abnormality | Component Given |
|---|---|---|
| ACT (clot initiation) | > 128 sec | FFP 2 units |
| Angle (fibrin cross-linking) | < 65° | Cryoprecipitate 10 units |
| MA (maximum amplitude - platelet function) | < 55 mm | Platelets 1 apheresis unit |
| LY30 (fibrinolysis at 30 min) | ≥ 10% | Tranexamic acid (TXA) 1 g |
Reassess via repeat citrated rapid TEG and cycle through again if bleeding persists.
When TEG is Unavailable - Lab-Based Triggers
| Lab Value | Threshold | Component |
|---|---|---|
| PT / PTT | > 1.5× control | 2 units thawed plasma (FFP) |
| Platelet count | < 50,000/μL | 1 unit apheresis platelets |
| Fibrinogen | < 100 mg/dL | 10 units pooled cryoprecipitate |
Adjunct Treatment of Shock in MTP
Beyond blood products, correct the lethal triad:
- Hypothermia - warm IV fluids, Bair Hugger, heated ventilator circuit; arteriovenous rewarming for temperature < 30°C
- Acidosis - avoid hyperchloremic acidosis from excessive NS; target hemorrhage control
- Coagulopathy - addressed by goal-directed blood product administration above
- Hypocalcemia - normalize ionized calcium (CaCl₂ or calcium gluconate)
Evidence Base for MTP
- Implementing an MTP has been shown to improve survival in trauma patients in multiple studies.
- The American College of Surgeons requires all verified trauma centers to have an MTP in place.
- The 1:1:1 RBC:plasma:platelet ratio emerged from military experience in Iraq/Afghanistan and has been validated in the PROPPR trial.
- Sabiston Textbook of Surgery; Schwartz's Principles of Surgery, 11e
Denver Health MTP Flowchart
Quick Reference Summary Table
| Component | Key Threshold / Indication | Dose | Expected Response |
|---|---|---|---|
| RBC (pRBC) | Hb < 7 g/dL (stable); < 8 g/dL (ACS/MI); hemorrhagic shock | Single units; re-evaluate | ↑ Hb ~1 g/dL per unit |
| Platelets | < 10K (prophylactic); < 50K (surgery/bleeding); < 100K (neurosurgery) | 1 apheresis unit or 4-6 pooled | ↑ platelet count 30-60K/μL |
| FFP | INR > 2 pre-procedure; massive transfusion (1:2 with RBC) | 15 mL/kg (~4 units) | ↑ all clotting factors ~2-3%/unit |
| Cryoprecipitate | Fibrinogen < 150 mg/dL with bleeding | 10-20 bags | ↑ fibrinogen ~7 mg/dL/unit |
| MTP | SBP ≤ 70 OR (SBP 71-90 + HR ≥ 108) + injury criteria | 1:1:1 ratio empirically, then TEG-guided | Correct hemorrhagic coagulopathy |
This is a shared conversation. Sign in to Orris to start your own chat.