Optic nerve decompression
Reading File
Finding Sources
Searching PubMed
"optic nerve decompression" OR "optic canal decompression"
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading Article
PMID: 38862644
Loading Image
Reading File
Now I have comprehensive material from Cummings Otolaryngology, Scott-Brown's, and recent evidence. Here is a structured clinical overview:
Optic Nerve Decompression
Definition and Overview
Optic nerve decompression (OND) is a surgical procedure to relieve pressure on the optic nerve, most commonly targeting the intracanalicular segment - the portion of the optic nerve confined within the rigid bony optic canal formed by two struts of the lesser wing of the sphenoid. This fixed bony enclosure makes the nerve particularly susceptible to injury and compressive injury.
- Cummings Otolaryngology Head and Neck Surgery, p. 974-975
Indications
1. Traumatic Optic Neuropathy (TON)
- Seen in 1.5-4% of all head trauma patients (up to 8% with TBI by some estimates)
- Mechanism: indirect transmission of blunt force to the optic canal -> nerve edema -> compartment-type syndrome -> apoptosis of retinal ganglion cells
- The role of surgical decompression in TON remains controversial (see below)
- Surgery is generally undertaken within 72 hours of injury if indicated
2. Compressive Optic Neuropathy (non-traumatic)
- Fibro-osseous lesions of the sphenoid (e.g., fibrous dysplasia)
- Skull base tumors compressing the orbital apex (meningioma - causes hyperostotic reaction with soft tissue mass effect)
- Sinonasal tumors
- Inflammatory conditions: orbital pseudotumor, Graves' orbitopathy (thyroid eye disease)
- Intra-sheath tumors (e.g., cavernous hemangioma of the optic canal)
- The majority of patients with compressive optic neuropathy derive significant visual improvement from decompression - in contrast to the controversial results in TON
3. Other
- Worsening vision in idiopathic intracranial hypertension (papilledema not responding to medical management)
- Orbital compartment syndrome (a distinct emergency requiring urgent intervention)
Surgical Approaches
Multiple approaches have been described, ranging from least to most invasive:
| Approach | Notes |
|---|---|
| Endoscopic endonasal | Now the preferred approach; minimally invasive, no external scar, preserves olfaction, excellent visualization |
| Transorbital | External route through the orbit |
| Transantral | Caldwell-Luc antrostomy approach (Walsh-Ogura method) |
| Extra-nasal transethmoidal | External ethmoid route |
| Intranasal microscopic | Predecessor to modern endoscopic technique |
| Craniotomy | Reserved for failure of other approaches or complex skull base pathology |
The endonasal endoscopic approach has largely supplanted open techniques. Open approaches remain relevant when endoscopic decompression has failed or is contraindicated.
Surgical Technique (Endoscopic - Standard Steps)
1. Complete ethmoidectomy and sphenoidotomy
- Expose the ethmoid roof and lamina papyracea
- Maximally open the sphenoid face to the planum sphenoidale superiorly and orbital apex laterally
- If an Onodi cell is present, remove the partition between the sphenoid sinus and Onodi cell
2. Identify key landmarks
- Bony prominences of the optic canal and carotid artery on the lateral sphenoid wall
- The opticocarotid recess (OCR) between them
- Image-guided surgery is recommended at this stage
- Note: the ophthalmic artery courses inferior/inferomedial to the optic nerve in ~20% of orbits - an important anatomical variant
3. Lamina papyracea removal
- Fracture and remove lamina papyracea ~1-1.5 cm anterior to the sphenoid face (eggshell technique)
- Avoid penetrating the periorbita - herniated orbital fat will obstruct the operative view
4. Optic canal drilling
- Use a high-speed diamond burr with copious irrigation (prevent thermal injury)
- Drill along the nerve, not across it
- Once bone is thinned, use a microcurette or elevator to gently flake fragments inferomedially away from the nerve
- Decompress 1 cm posterior to the face of the sphenoid for TON and thyroid eye disease
5. Optic nerve sheath incision (selective)
- Performed after bony decompression is complete
- Use a disposable sickle knife along the entire exposed nerve length, posterior to anterior, incorporating the annulus of Zinn
- CSF egress is expected
- If done, a mucosal onlay graft should be considered to prevent postoperative rhinorrhea
- Sheath incision is required for intra-sheath tumors; remains debated for indirect TON
Preoperative Workup
- Complete ophthalmologic examination: visual acuity, color vision (dyschromatopsia), relative afferent pupillary defect (RAPD), visual fields
- CT of sinuses and orbit: optic canal fracture/compression, bony anatomy, sinus anatomy
- MRI orbits with/without contrast: evaluate the full course of the optic nerve and orbital contents (preferred for compressive optic neuropathy)
- Visual evoked potentials: occasionally useful in obtunded/unresponsive patients (impractical in acute trauma)
Controversies: Traumatic Optic Neuropathy
The management of indirect TON is one of the most debated areas in the field. Three treatment options exist:
- Expectant management - spontaneous recovery is possible
- Corticosteroids (high-dose IV methylprednisolone) - earlier meta-analyses showed benefit; however, the International Optic Nerve Trauma Study (IONTS) failed to show a difference between groups. High-dose steroids carry increased mortality risk in acute TBI
- Surgical decompression - similarly shown in IONTS to offer no statistically significant benefit over observation
Current Consensus: No treatment (including surgery) has demonstrated clear benefit over observation in indirect TON. There is strong evidence of harm from megadose IVMP in TBI patients (increased mortality). Treatment must be individualized. - Blanch et al., Eye, 2024 [PMID: 38862644, Systematic Review]
Optic Nerve Sheath Incision: Debated in TON
- Not shown to be superior to bony decompression alone
- Theoretical advantage: allows more maximal decompression, especially with intra-sheath hematoma
- Risk: potential injury to optic nerve or ophthalmic artery; increased CSF leak risk
- Required for intra-sheath tumors (direct removal and decompression)
Outcomes
| Indication | Expected Outcome |
|---|---|
| Traumatic optic neuropathy | ~40-60% of patients show improvement in visual acuity; patients with no light perception at presentation have the poorest prognosis |
| Compressive optic neuropathy | Majority derive significant visual acuity improvement |
| Thyroid eye disease (compressive) | Good outcomes when combined with orbital decompression |
Complications
- Direct injury to the optic nerve (rare but devastating - permanent visual loss)
- Injury to the ophthalmic artery
- CSF leak (especially after nerve sheath incision - manage with mucosal onlay graft)
- Complications shared with endoscopic sinus surgery: bleeding, orbital hematoma, orbital fat herniation
- Postoperative rhinorrhea
- Diplopia (more relevant in combined orbital + optic nerve decompression for GO)
Key Points
- The intracanalicular segment is most vulnerable due to fixed bony confinement
- Endoscopic endonasal approach is now the standard, with open approaches reserved for failures or contraindications
- Decompression in TON is controversial with no high-level evidence of benefit; compressive optic neuropathy responds much better
- Diamond burr drilling with copious irrigation is the standard technique to avoid thermal nerve injury
- The ophthalmic artery has an anatomical variant (inferomedial course) in ~20% of orbits - vigilance required
- Multidisciplinary collaboration between otolaryngology and ophthalmology is essential
Sources:
- Cummings Otolaryngology Head and Neck Surgery, pp. 974-979 (Endoscopic Optic Nerve Decompression chapter)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 1, pp. 1297-1232 (Endoscopic optic nerve decompression)
- Blanch RJ et al. "Traumatic optic neuropathy management: a systematic review." Eye (Lond), 2024 Aug. [PMID: 38862644]
Bullous myringitis
Finding Sources
Searching PubMed
"bullous myringitis"
Reading File
Reading File
Reading File
Reading Article
PMID: 33883520
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive summary of bullous myringitis synthesized from four major otolaryngology and primary care textbooks plus recent systematic review evidence:
Bullous Myringitis
Definition
Bullous myringitis (BM) is an acute inflammatory condition of the tympanic membrane (TM) characterized by the formation of bullae (vesicles) on its surface. The bullae may be single or multiple, affecting a segment or the whole TM, and may extend onto the adjacent medial ear canal wall.
Pathology
The bullae are believed to develop between the middle fibrous layer and the outer squamous layer of the TM due to extravasation of serous fluid or blood. This has never been confirmed histologically, but it explains the serous or serosanguinous content seen on rupture. The intact TM (no perforation) distinguishes BM from otitis media with perforation - any otorrhea that occurs is typically scanty and self-limiting.
Otoscopic Appearance
The hallmark finding is bullae over the TM and medial canal wall, filled with serous or serosanguinous (blood-tinged) fluid:

Large single hemorrhagic bulla on the posterior aspect of the tympanic membrane - Scott-Brown's Otorhinolaryngology, Vol. 2
Aetiology
The long-held belief that BM is pathognomonic for Mycoplasma pneumoniae has been largely dispelled. Roberts (1980) summarized 6 studies with 858 BM patients - M. pneumoniae was isolated from only one. More recent evidence shows the pathogen profile closely mirrors that of acute otitis media (AOM):
- Bacterial: Streptococcus pneumoniae (consistently the predominant organism), Haemophilus influenzae, Moraxella catarrhalis, beta-haemolytic streptococci
- Viral: Rhinovirus, enterovirus, RSV, influenza A, parainfluenza virus
The tympanic blistering is likely a non-specific inflammatory response to infection, not a pathognomonic finding of any single pathogen. This view is further supported by the fact that BM is diagnosed with concurrent AOM in ~97% of cases in large paediatric series, suggesting BM may simply represent a severe variant of AOM.
Epidemiology
- True incidence is unknown, but reported in 5.7% of children under 2 years in a 1-year follow-up period
- Occurs in 1 in every 20 episodes of AOM
- Most prevalent in children aged 2-8 years (unlike AOM which peaks under 2 years)
- More common in winter months
- Usually unilateral
Clinical Features
Symptoms
- Severe, sudden-onset otalgia - typically disproportionate to the findings on examination; often the most prominent symptom
- Pain usually lasts 1-2 days, though discomfort may persist even after bulla rupture
- Compared with AOM alone, BM children show higher rates of earache (58% vs 29%), fever (62% vs 41%), and excessive crying (80% vs 65%)
- Associated upper respiratory tract infection is common
Signs
- Bullae on the TM and medial canal - serous or serosanguinous, may be single or multiple
- Scanty serosanguinous otorrhoea upon rupture (short-lived; no TM perforation)
- Middle ear effusion present in 30-40% of cases (serous OM)
- Hearing loss (see below)
Hearing Loss - A Key Complication
This is one of the most clinically important aspects of BM:
| Type | Frequency |
|---|---|
| Conductive hearing loss (CHL) | Common; from middle ear effusion |
| Sensorineural hearing loss (SNHL) or mixed | 15-66% of cases (widely varying series) |
| Sensorineural component (pure or mixed) | ~55-82% in some series |
Key points on SNHL:
- The cochlea is implicated as the site of lesion (stapedial reflex and ABR data)
- Pathogenesis of SNHL in BM is unknown
- Complete recovery of hearing occurs in 57-100% of cases regardless of treatment, though pre-existing audiological baselines are rarely available
- History and physical examination alone cannot exclude SNHL - formal audiometry is mandatory
A 2021 systematic review (Ungar et al., Otol Neurotol, PMID: 33883520) found that of 81 BM patients, 62% had confirmed hearing loss on audiometry despite only 48% reporting it subjectively. SNHL or mixed HL was present in the vast majority of those with hearing loss - pure CHL was very uncommon. This has important implications: do not wait for formal audiometry before initiating steroid treatment.
Vertigo
A prospective study showed 54% of BM patients reported vertigo at presentation; 85% had abnormal electronystagmography, including 4 patients with no subjective vertigo complaint - indicating subclinical vestibular involvement is common.
Differential Diagnosis
Three conditions must be distinguished:
| Condition | Key Distinguishing Feature |
|---|---|
| Bullous myringitis | Bullae limited to TM + medial canal; self-limiting otorrhoea |
| Acute otitis externa | Diffuse canal involvement; requires topical treatment |
| Herpes zoster oticus (Ramsay Hunt) | Vesicles on pinna/concha/canal; can cause CN VII palsy; requires antivirals |
Neither OE nor herpes zoster is typically limited to the TM alone.
Treatment
There is no consensus or high-quality evidence to guide best practice. BM is largely a self-limiting disease.
Symptomatic
- Analgesics - oral analgesia is the mainstay (pain can be severe)
- Warm compresses
- Incision/lancing of bullae - for pain relief; benefit is unproven and carries risk of secondary infection; no definitive evidence of superiority over analgesia alone
Topical
- Antibiotic/steroid drops - to prevent bacterial superinfection of the ruptured bulla
Systemic Antibiotics
- Treat as for AOM given the comparable pathogen profile
- Broad-spectrum oral antibiotics are favoured, particularly when SNHL is present
Systemic Corticosteroids (Controversial)
- Used by some authors for SNHL component, analogous to treatment of sudden sensorineural hearing loss
- Typical regimen: prednisone 1 mg/kg/day for 7 days, then tapered
- Evidence is weak: only one small comparative study (n=23) - systemic antibiotics alone vs. antibiotics + steroids - showed no improved hearing outcomes with steroids, but was likely underpowered (type II error risk)
- Eliashar et al. treated SNHL with admission + oral steroids + carbogen: 86% complete hearing recovery
- Randomized trials are lacking
Current practice guidance (Ungar et al., 2021): Because pure CHL is uncommon in BM and SNHL is frequently present (even when not subjectively reported), steroid treatment should not be delayed pending formal audiometry. Early empirical steroids are recommended when BM is diagnosed.
Myringotomy
- Indicated if middle ear effusion accompanies bullae formation
Prognosis
- Generally good and self-limiting
- Hearing loss in the majority recovers fully
- Persistent SNHL is possible - emphasizing the importance of follow-up audiometry
- No TM perforation expected from bullae rupture
Sources:
- Shambaugh Surgery of the Ear, pp. 2103-2126
- Cummings Otolaryngology Head and Neck Surgery, p. 2654
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, pp. 979-980
- K.J. Lee's Essential Otolaryngology, p. 436
- Textbook of Family Medicine 9e, p. 660
- Ungar OJ et al. "The Actual Incidence and Types of Hearing Losses in Bullous Myringitis." Otol Neurotol, 2021. [PMID: 33883520 - Systematic Review]
Prosthesis after maxillectomy
Finding Sources
Searching PubMed
"maxillectomy" AND "obturator prosthesis"
Finding Sources
Finding Sources
Searching PubMed
"maxillectomy" AND "obturator" AND "rehabilitation"
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive material. Here is the full structured overview:
Prosthesis After Maxillectomy
Overview
Maxillectomy creates an oronasal/oroantral defect that impairs speech, swallowing, mastication, and facial aesthetics. Two broad reconstruction strategies exist: prosthetic obturation and free tissue transfer (microvascular reconstruction). Prior to the advent of reliable free flap surgery, obturation was the primary method of management. Today it remains a valuable option in specific clinical contexts, and the decision between the two approaches must be individualized and multidisciplinary.
Multidisciplinary Team (MDT)
Prosthetic rehabilitation should be led by the maxillofacial prosthodontist in close collaboration with:
- Head and neck surgeon
- Oncologist/radiation oncologist
- Speech and language therapist
- Dental hygienist
- Specialist dental/facial prosthetic technicians
- The patient's primary dental practitioner (in dentate patients)
Classification of Maxillectomy Defects
Two classification systems guide decision-making:
- Brown's classification - surgery-based; widely used to decide between surgical reconstruction and obturation. When the defect extends beyond level 2, obturation yields increasingly poor results and surgical reconstruction is preferred
- Okay's classification - more directed at the maxillofacial prosthodontist; guides obturator design based on the remaining dental configuration following surgery
General principle: The more extensive the defect, the stronger the case for free tissue transfer. Defects involving the orbital floor should be reconstructed surgically wherever possible to prevent inferior displacement of the globe.
Pre-surgical Assessment
All patients should be evaluated by the maxillofacial prosthodontist before surgery:
- Screening panoramic dental radiograph + detailed oral examination
- Decision-making on dental extractions, restorations, and pre-prosthetic preparation
- Impressions and dental models taken pre-operatively (mandatory for dentate patients; may not be required for edentulous patients already wearing a well-extended prosthesis)
- Planning for osseointegrated implant placement (primary at time of surgery or secondary)
- A clear explanation to the patient of the staged prosthetic process and follow-up requirements
The Three Stages of Obturator Provision
Stage 1: Surgical Obturator (Immediate)
Inserted at the time of surgery, prior to extubation.
Purpose:
- Separates oral and nasal/antral cavities immediately
- Supports cheek soft tissues
- Assists haemostasis
- Enables early speech and swallowing
Construction:
- Pre-operative dental models allow fabrication of a tooth-bearing obturator; alternatively a simple clear acrylic cover plate is used when time is limited
- Obturating material options: addition-cured silicone putty (preferred - engages undercuts, supports cheek, assists haemostasis), black gutta percha, foam products
Retention of surgical obturator:
- Small defects with sufficient remaining teeth: dental clasps suffice
- Larger defects: bone screws and/or circum-zygomatic wires
Post-operative management:
- Requires regular removal and modification as the defect heals and shrinks
- Small defects: managed in outpatient clinic
- Large defects (especially with circum-zygomatic wires): may require return to the operating room
- Generally left in situ for 6-8 weeks post-operatively
Stage 2: Interim Obturator
- Provided after wound healing, typically at ~6-8 weeks
- The defect continues to change shape during this phase; the interim obturator is adjusted as required
- Allows the patient to resume eating, speech rehabilitation continues
- Transition period lasting several months while the defect matures
Stage 3: Definitive Obturator
- Constructed once the defect has fully healed and stabilized (typically 3-6+ months post-surgery, longer if radiotherapy is given)
- A bespoke, carefully crafted prosthesis that restores form and function optimally
Surgical Modifications to Facilitate Obturator Provision
Several surgical techniques at the time of maxillectomy improve the quality of prosthetic rehabilitation:
- Bone cuts through edentulous areas or extraction sockets - preserves periodontal bone support of remaining abutment teeth, which are vital for obturator retention
- Palatal mucosal incisions made lateral to bone cuts - creates a keratinized mucosal flap that folds over the cut bone edge, cushioning the prosthesis during masticatory function
- Split-skin graft to the cheek defect - produces a scar band within the cheek that assists retention of the obturator (one of the few retentive surfaces available in conventional obturation)
- Removal of the inferior turbinate(s) - creates more vertical space for the obturator and prevents future trauma to prolapsed turbinate tissue
- Smoothing of sharp bony margins - essential for all prosthetic rehabilitation
Obturator Design
Simple Obturator
- For low-level partial maxillectomy defects
- A soft silicone bung engages natural undercuts in the defect for retention

Simple maxillary obturator prosthesis with integral soft bung to engage defect undercuts - Scott-Brown's Vol. 3
Multi-Part Obturator
- Used when trismus limits access for impressions or prosthesis insertion/removal
- Trismus is common post-maxillectomy, especially after radiotherapy
- Impressions are taken in several parts using a multi-part technique
- The definitive obturator has a separate obturator component that inserts directly into the defect and attaches to the overlying dental component via magnet linkage

2-part obturator: the obturator component (left) and dental prosthesis component (right), joined intra-orally by magnets - Scott-Brown's Vol. 3
Osseointegrated Implants in Maxillary Obturation
When conventional obturator retention is inadequate - particularly in:
- Extensive maxillary defects
- Edentulous patients
- Patients with severe trismus
- Patients with few or no remaining teeth
Osseointegrated implants dramatically improve retention and stability.
Zygomatic Implants
- Particularly useful for large maxillary defects where there is insufficient alveolar bone for standard implants
- Achieve very high initial stability and can support the obturator at an early stage
- Multiple zygomatic implants are typically splinted together with a retentive bar, and the obturator clips or screws onto this bar
- Should ideally be placed at the time of primary resection if post-operative radiotherapy is planned, to allow osseointegration before radiotherapy-induced changes compromise implant success
- When implant-retained, the need for the prosthesis to deeply engage the defect undercuts is greatly reduced
Standard Dental Implants
- Placed in residual alveolar bone or in reconstructed bone (e.g., fibula flap)
- Can provide excellent retention in partially dentate patients with smaller defects
Facial Prostheses (Midfacial/Orbital Defects)
When maxillectomy extends to involve the midface, orbit, or nose, silicone-based facial prostheses are used. These are distinct from intra-oral obturators and address external facial defects.
Retention methods (evolution):
- Traditionally: skin adhesives, spectacle frames, mechanical undercuts
- Modern standard: osseointegrated craniofacial implants (last 30 years)
- Conventional adhesive-retained prostheses remain useful but are difficult to locate accurately, prone to dislodgement, and cause skin irritation
Pre-prosthetic surgical principles:
- Remove small areas of unsupported tissue to provide a solid margin
- Keep bulk of vascularized flaps in this area minimal (or debulk before prosthesis construction)
- Smooth sharp bony margins
- Use split-skin grafts within the orbit: provide a stable, hair-free, drier surface
- For rhinectomy: preserve nasal bones when oncologically safe - assists prosthesis retention
Obturator vs. Free Flap Reconstruction
| Factor | Obturator Favoured | Free Flap Favoured |
|---|---|---|
| Defect size | Small-moderate (level 1-2) | Large (level 3+) |
| Orbital floor involvement | No | Yes |
| Dental status | Dentate (good retention) | Edentulous |
| Oncologic surveillance | Obturator allows direct inspection | Flap obscures defect |
| Patient fitness | Poor surgical candidate | Good surgical candidate |
| HRQoL (large defects) | Worse (esp. if edentulous + XRT) | Better for complex resections |
HRQoL evidence: Obturator prosthesis is a highly positive and non-invasive approach for quality of life in maxillectomy defects. However, for large complex resections (palate + maxilla + sinuses + orbital content), microvascular reconstruction yields better HRQoL outcomes. Edentulous obturated patients have worse outcomes than dentate patients; adjuvant radiotherapy further worsens mouth opening and oral/swallowing function.
Complications and Challenges
- Trismus - limits access for impressions, insertion/removal; may necessitate extraction of additional teeth and multi-part obturator design
- Radiotherapy effects - xerostomia, trismus, mucositis, compromised implant osseointegration, increased risk of osteoradionecrosis with implants placed post-radiotherapy
- Retention difficulties - especially in edentulous patients and large defects; addressed with implants
- Globe displacement - inferior drop of globe if orbital floor not reconstructed
- Lip contracture - can occur after level 2 maxillectomy and obturation
- Speech and swallowing - incompletely restored by obturation in large defects; multidisciplinary support needed
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 3, pp. 543-547 (Prosthodontic Rehabilitation chapter)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, pp. 979 (HRQoL after maxillectomy)
- K.J. Lee's Essential Otolaryngology, p. 436
- Cummings Otolaryngology Head and Neck Surgery, pp. 1945, 2437
Superior semicircular canal dehiscence syndrome
Finding Sources
Searching PubMed
"superior semicircular canal dehiscence"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive material from four major textbooks. Here is the full structured summary:
Superior Semicircular Canal Dehiscence Syndrome (SCDS)
Background and Discovery
SCDS was first described by Minor and colleagues at Johns Hopkins in 2000, making it a relatively new clinical entity in otology. It is defined by the absence of the normal bony covering over the superior semicircular canal (SSC) at the arcuate eminence on the floor of the middle cranial fossa.
An important caveat: absent or thin bone over the SSC is found in up to 13% of asymptomatic individuals on CT scanning, which means the mere radiographic presence of dehiscence does not equal the syndrome - clinical correlation is essential.
There is morphometric evidence that SCDS is associated with a generalized reduction in thickness of the squamous portion of the temporal bone, which predisposes to defects at the middle fossa floor and explains the frequent co-existence with natural dehiscences of the tegmen tympani and tegmen mastoideum.
Pathophysiology: The "Third Mobile Window"
The normal inner ear has two mobile windows: the oval window (stapes footplate) and the round window. Sound pressure enters through the oval window, travels around the cochlea, and exits through the round window.
A dehiscence of the superior canal creates a third mobile window into the labyrinth. This has two important consequences:
1. Auditory effects
- Air-conducted sound energy is dissipated away from the cochlea through the dehiscence → reduced cochlear stimulation by air conduction → apparent conductive hearing loss
- Bone-conducted stimuli are enhanced or thresholds unchanged → bone conduction thresholds may be supra-normal (better than 0 dB)
- Net result: air-bone gap, predominantly in low frequencies (<2,000 Hz), with bone conduction thresholds sometimes reaching -20 dB or better
- Additionally, the abnormal third window alters hydrodynamic forces within the cochlea, biasing the basilar membrane toward the scala tympani - analogous to endolymphatic hydrops - which explains elevated SP/AP ratios on electrocochleography (ECochG)
2. Vestibular effects
- Sound pressure and intracranial/middle ear pressure changes are transmitted to the SSC via the dehiscence
- Loud sounds and positive pressure in the external canal → ampullofugal deflection of the superior canal → excitation of SSC afferents
- Negative pressure or Valsalva against closed glottis → ampullopetal deflection → inhibition of SSC afferents
- The eye movements evoked are strictly in the plane of the superior canal regardless of direction of gaze
Clinical Features
Patients may have exclusively auditory, exclusively vestibular, or both symptom types. The reason for this variability is unknown.
Auditory Symptoms
| Symptom | Mechanism |
|---|---|
| Autophony (hearing own voice abnormally loud) | Sound conducted directly to inner ear via dehiscence |
| Pulsatile tinnitus | Pulsatile intracranial pressure transmitted to SSC |
| Aural fullness / pressure | Third window pressure effects |
| Hyperacusis to bone-conducted sounds | Enhanced bone conduction thresholds |
| Hearing own eye movements in the affected ear | Bizarre but characteristic symptom |
| Hearing footsteps / long-bone vibration (e.g., running) | Bone-conducted energy transmitted via dehiscence |
| Air-bone gap on audiogram (low frequencies) | Third window dissipating air-conducted energy |
Vestibular Symptoms
| Symptom | Trigger |
|---|---|
| Tullio phenomenon - vertigo/oscillopsia induced by loud sounds | Acoustic stimulation of SSC via dehiscence |
| Hennebert sign - vertigo/nystagmus with positive pressure in canal or tragal pressure | Pressure transmitted to SSC |
| Pressure-induced vertigo - Valsalva, nose-blowing, straining, coughing | Intracranial pressure changes |
| Chronic disequilibrium | Persistent third window effect |
| Spontaneous unprovoked vertigo attacks | In some patients |
| Oscillopsia - apparent motion of stationary objects | SSC stimulation |
Characteristic Eye Movement
On provocation (loud sound or pressure stimulus), the eye moves in the plane of the superior canal:
- Slow phase: upward + torsional rotation of the superior pole away from the affected ear (with SSC excitation)
- Opposite direction (downward + torsion toward affected ear) with SSC inhibition
Diagnosis
Audiometry
- Air-bone gap in low frequencies (typically below 2,000 Hz)
- Supra-normal bone conduction thresholds (e.g., -10 to -20 dB)
- Acoustic reflexes present in the affected ear - this is the critical distinguishing point from otosclerosis, which also shows low-frequency CHL but with absent reflexes
- Patients with intact acoustic reflexes + air-bone gap must be investigated for SCDS before any middle ear surgery is contemplated - some have undergone unnecessary stapedectomy which does not close the air-bone gap
Key rule: Air-bone gap + present acoustic reflexes = investigate for SSCD before stapedectomy
Vestibular Evoked Myogenic Potentials (VEMP)
- Cervical VEMP (cVEMP): Lowered threshold + elevated amplitude in the affected ear - highly useful screening test. Normal cVEMP threshold is ~90-100 dB nHL; in SSCD it may drop to 60-70 dB
- Ocular VEMP (oVEMP): May be more sensitive and specific than cVEMP for this diagnosis; amplitudes are elevated on the ipsilateral side
- Both reflect the enhanced responsiveness of the otolith organs through the dehiscence
Electrocochleography (ECochG)
- Elevated SP/AP (summating potential/action potential) ratio in the symptomatic ear, similar to Meniere disease (mean 0.62 in affected ears vs. 0.29 in unaffected ears)
- Useful as a sensitive adjunct and as an intraoperative monitoring tool: the SP/AP ratio increases when the dehiscence is surgically exposed and normalizes immediately upon satisfactory plugging of the canal
- Criterion for abnormality: SP/AP >0.4
High-Resolution CT of the Temporal Bone
The definitive imaging modality.
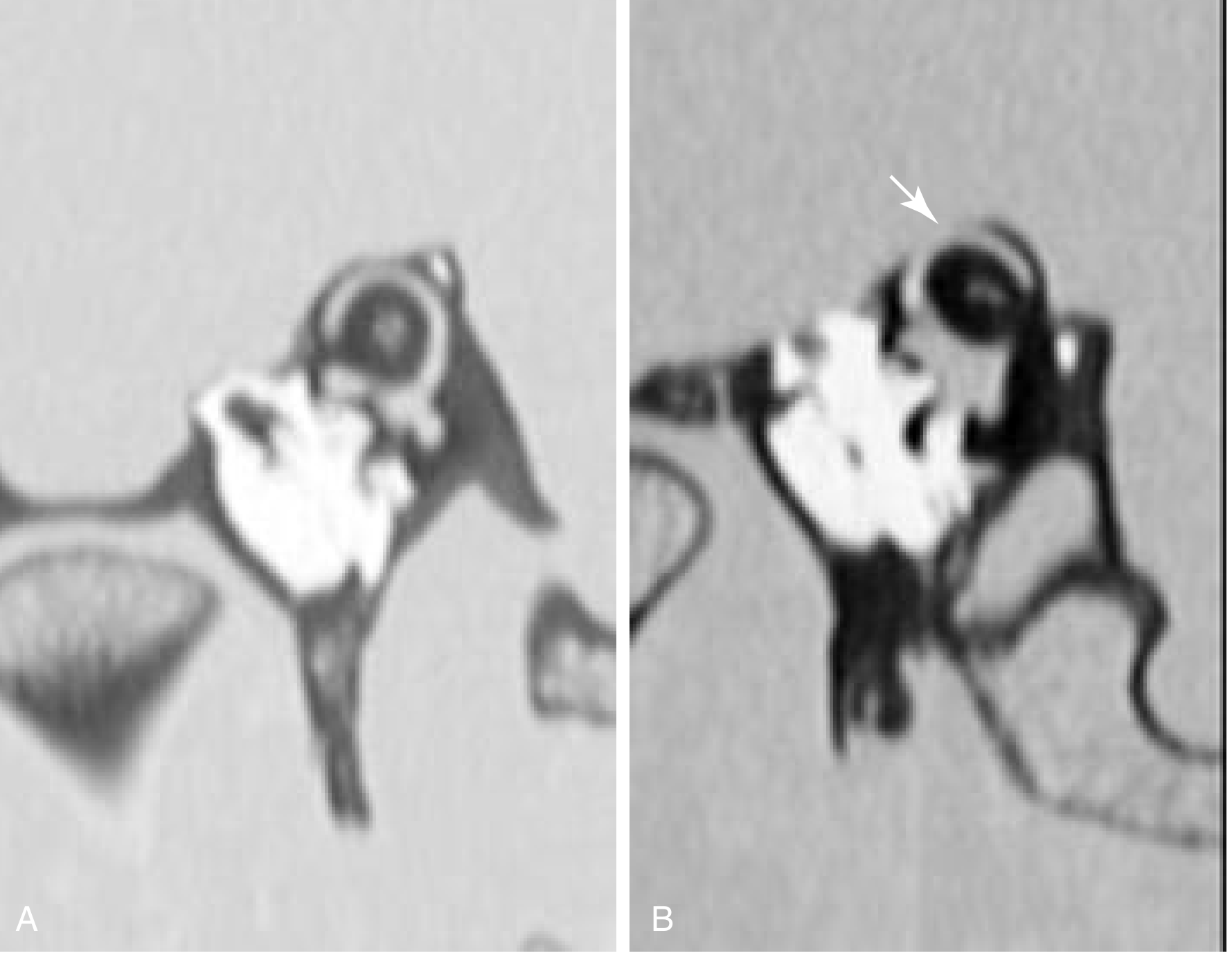
CT in the parasagittal (Pöschl) plane orthogonal to the superior canal. (A) Normal bone cover; (B) dehiscence of the superior canal (arrow). - Cummings Otolaryngology, p. 3250
Key imaging points:
- Images must be reconstructed in two dedicated planes:
- Pöschl plane - parallel to the superior canal (best demonstrates dehiscence)
- Stenver plane - perpendicular to the superior canal
- Conventional 1-mm axial/coronal CT has low specificity (high false-positive rate) due to partial volume averaging
- In cases of near-dehiscence (very thin bone that is not truly absent), CT may fail to confirm the diagnosis even with thin cuts - clinical and physiologic findings must then carry greater diagnostic weight
- CT is essential to plan the surgical approach (defect location, angle subtended, middle fossa anatomy)
Differential Diagnosis
| Condition | Key Distinguishing Feature |
|---|---|
| Otosclerosis | Absent acoustic reflexes; normal bone conduction thresholds (not supra-normal) |
| Patulous Eustachian tube | Also causes autophony; no air-bone gap; tympanometry with respiratory oscillations |
| Meniere disease | Episodic SNHL/vertigo; elevated SP/AP but no supra-normal bone conduction; no pressure/sound-evoked nystagmus |
| Perilymph fistula | History of trauma/barotrauma; no air-bone gap pattern; no supra-normal BC thresholds |
Note: SCDS is frequently misdiagnosed as a patulous Eustachian tube due to prominent autophony.
Third Window Lesions - Differential
SCDS is the best-characterized of a broader class of third window lesions that cause apparent conductive hearing loss from inner ear pathology:
Anatomical (discrete) third windows:
- Semicircular canals: superior, posterior, or lateral canal dehiscence
- Vestibule: large vestibular aqueduct syndrome, inner ear malformations
- Cochlea: dehiscence between carotid canal and scala vestibuli; DFN-3 (X-linked deafness with stapes gusher)
Diffuse third window:
- Paget disease of bone
Management
Conservative
- Many patients with incidentally discovered dehiscence and mild symptoms can be managed conservatively
- Avoidance of triggering stimuli (loud sounds, straining)
- Careful counseling about the risks of middle fossa craniotomy before considering surgery
- Vestibular rehabilitation for chronic disequilibrium
Surgical Indications
Surgery is reserved for debilitating symptoms significantly impacting quality of life. The severity and lifestyle impact are the major determinants.
Key principle: The dehiscence is repaired by plugging, not merely resurfacing. Canal plugging is associated with more reliable and complete relief of vestibular symptoms than resurfacing alone.
Surgical Approaches
1. Middle Cranial Fossa (MCF) Craniotomy
- The original and most established approach (Minor, 2000)
- Allows direct visualization and confirmation of the dehiscence
- The SP/AP ratio actually rises when the dehiscence is surgically exposed, then normalizes immediately upon satisfactory plugging - confirming adequacy of repair intraoperatively
- ECochG intraoperative monitoring is used routinely
- Plugging reliably relieves vestibular symptoms and reduces aVOR gain for the superior canal by ~44% (with a modest 10% reduction of the ipsilateral posterior canal)
- Resolves many auditory symptoms; hearing loss improvement is less predictable
- Disadvantage: Requires craniotomy + temporal lobe retraction
2. Transmastoid Approach
- More recently described alternative
- Advantages: Avoids craniotomy; no temporal lobe retraction; surgeons more familiar with mastoidectomy
- Disadvantages: Does not permit direct confirmation of dehiscence (transmastoid plugging of an intact canal has been described); plug is placed closer to the sensory epithelia (ampulla and utricle), risking disturbance; not feasible with low-hanging dura or extensive tegmen dehiscence
- Initial reports included one case of significant SNHL post-operatively; more recent series report minimal morbidity
3. Round Window Reinforcement (Third Window Occlusion)
- Controversial alternative approach: does not directly address the third window at the superior canal
- Some patients developed worse symptoms - not widely recommended
Plugging Materials and Technique
- Materials used: bone wax, bone dust, fascia/periosteum, surgical glue - applied in multiple layers
- Care must be taken to avoid suctioning perilymph from the dehiscence intraoperatively
Sources:
- Cummings Otolaryngology Head and Neck Surgery, pp. 2574-2576 (ECochG in SSCD); pp. 3249-3250 (Surgery for SSCD)
- Shambaugh Surgery of the Ear, pp. 86-88 (Third window lesions); pp. 600-601 (SCDS pathophysiology and surgery)
- K.J. Lee's Essential Otolaryngology, pp. 63-64 (SSCS syndrome)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, p. 1236 (CT imaging of SSCD)
EBV in ent
Finding Sources
Finding Sources
Searching PubMed
"Epstein-Barr virus" AND ("head and neck" OR "nasopharyngeal carcinoma")
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Excellent - I now have comprehensive content from all major textbooks. Here is the full structured overview:
Epstein-Barr Virus (EBV) in ENT
Virology and Epidemiology
EBV (Human Herpesvirus-4 / HHV-4) is a ubiquitous herpesvirus - a member of the Herpesviridae family. It has a special affinity for B lymphocytes, binding via its envelope glycoprotein to CD21 (complement receptor 2) expressed on all B cells. It also infects epithelial cells of the oropharynx and genital tract.
Transmission: primarily via saliva (kissing - hence "kissing disease"). Also transmitted via bodily secretions and blood transfusion.
Epidemiology:
- In lower-income settings with less hygiene: EBV infection in early childhood is nearly universal; usually asymptomatic
- In higher-income settings: infection is delayed until adolescence/young adulthood; symptomatic disease is much more common
- Only ~20% of seropositive persons in high-income countries shed virus; ~50% of those exposed acquire infection
- More than half of infected individuals continue to shed virus in saliva, usually for life
Latency: In most infected B cells, the virus is latent, persisting as an extrachromosomal episome. In a minority, infection shifts to a lytic phase with viral replication and release of virions. Latent B cells may become activated and proliferate under the action of several viral proteins.
EBV's Role in ENT - Overview
EBV causes a broad spectrum of head and neck conditions, ranging from the commonplace (infectious mononucleosis) to aggressive malignancies:
| Domain | Condition |
|---|---|
| Benign infectious | Infectious mononucleosis (glandular fever) |
| Oral/mucosal | Oral hairy leukoplakia |
| Malignant - epithelial | Nasopharyngeal carcinoma |
| Malignant - lymphoid | NK/T-cell lymphoma (nasal type / ENKL) |
| Malignant - lymphoid | Hodgkin lymphoma |
| Malignant - lymphoid | Burkitt lymphoma |
| Malignant - lymphoid | EBV+ DLBCL |
| Malignant - lymphoid | Post-transplant lymphoproliferative disorder (PTLD) |
| Malignant - lymphoid | Chronic active EBV infection (T/NK type) |
1. Infectious Mononucleosis (IM) / Glandular Fever
Pathogenesis
- EBV infects oropharyngeal epithelial cells initially, then spreads to underlying lymphoid tissue (tonsils, adenoids), where B cells are infected via CD21
- Infected B cells disseminate in circulation, secreting antibodies with unusual specificities (including heterophile antibodies against sheep/horse/bovine erythrocytes - the basis of diagnostic tests)
- Host CD8+ T-cell response controls B-cell proliferation and viral spread - the "atypical lymphocytes" on peripheral blood smear are activated CD8+ T cells, not infected B cells
Clinical Features (ENT Focus)
- Incubation period: 4-7 weeks
- Classical triad: sore throat + cervical lymphadenopathy + fever
- Tonsil enlargement: can be massive; may cause airway compromise and dysphagia
- Palatal petechiae: more common in younger patients
- Periorbital oedema (especially lower lids) - Hoagland sign
- Hepatomegaly and jaundice: more common in older patients
- Splenomegaly: late sign, resolves in 3-4 weeks
- Nasopharyngeal lymphoid hyperplasia: present in 92% of IM patients on flexible nasendoscopy - helps distinguish IM from acute tonsillitis
Key ENT differential: The differential between acute bacterial tonsillitis and IM can be aided by flexible nasendoscopy. Lymphoid tissue in the nasopharynx is seen in 92% of IM but not in ordinary tonsillitis.
Investigations
- FBC: lymphocytosis >50% of WBC with >10% atypical lymphocytes (Hoagland criteria), or >20% atypical lymphocytes alone
- Liver and renal function tests
- Monospot test (heterophile antibody): latex agglutination using horse RBCs; sensitivity 63-95%, specificity 84-100%
- Positivity increases over the first 6 weeks (heterophile antibody titres peak)
- Approximately 10% never develop a positive test (higher rate in children)
- False positives: mumps, SLE, Mediterranean spotted fever, diabetes, sarcoidosis
- Paul-Bunnell test: based on sheep RBC agglutination (older method)
- Gold standard: IgM antibody to EBV viral capsid antigen (VCA-IgM) during acute primary infection
- EBV viral load by PCR: useful in inconclusive serology
- L/WBC ratio >0.35: suggested as a screening tool but sensitivity 72%/specificity 84% - insufficient alone; use only with Hoagland criteria
If Monospot is repeatedly negative, consider: CMV, HIV, Toxoplasmosis, Rubella
Management
General (mild-moderate):
- Supportive: fluids, analgesia, rest
- Treat superimposed streptococcal infection if present (confirmed by throat culture)
- AVOID aminopenicillins (ampicillin/amoxicillin): virtually 100% develop a maculopapular/rubelliform rash due to transient immunostimulation (amoxicillin: 30%; ampicillin: 90%)
- Use penicillin V or cephalosporins if antibiotic needed; IV penicillin or cephalosporins for those admitted
Corticosteroids:
- Cochrane review: insufficient evidence to recommend steroids for routine symptom control in IM
- Indicated for: significant tonsillar swelling causing airway compromise/swallowing difficulty (short course)
- Corticosteroids improve pain scores and time to resolution, especially when combined with antibiotics
- When airway is unsafe: intubation or tracheostomy required
Antivirals:
- Acyclovir: meta-analysis of 5 RCTs (n=339) - clinical data do not justify use for mild-moderate IM
- May benefit patients with severe manifestations, especially as an adjunct to corticosteroids
Activity restriction:
- Patients must avoid sport/vigorous activity due to risk of splenic rupture (usually following minor trauma; rate <1 in 500)
Complications
| Complication | Notes |
|---|---|
| Airway obstruction | Cervical lymphadenopathy + tonsillar hypertrophy; rare but potentially fatal |
| Splenic rupture | Usually minor trauma; rate <1/500; patients counselled re: activity |
| Anaemia / thrombocytopenia | Haematological |
| Haemophagocytic syndrome | Severe |
| Encephalitis / meningitis | Neurological |
| Transverse myelitis, Guillain-Barré syndrome | |
| Pericarditis / myocarditis | Cardiovascular |
| Hepatomegaly / jaundice | In 10% |
| Chronic fatigue syndrome | 13% at 6 months; 4% at 2 years post-IM |
| Multiple sclerosis | Recent evidence: history of IM significantly increases MS risk |
| Unexpected death | Related to upper airway obstruction |
2. Nasopharyngeal Carcinoma (NPC)
EBV Link
EBV is strongly associated with NPC, particularly the undifferentiated/non-keratinizing subtype (WHO type II and III). Key molecular events:
- EBV infects nasopharyngeal epithelium
- In susceptible individuals → epithelial cell transformation
- Tumor cells contain EBV genomes and express latent membrane protein-1 (LMP1), which activates the NF-κB pathway generating oncogenic signals
- Tumors are often heavily infiltrated by T cells responding to viral antigens
Histological Types
| Type | EBV Association |
|---|---|
| Keratinizing SCC | Weak |
| Non-keratinizing SCC | Strong |
| Undifferentiated carcinoma | Strongest (most common type) |
Undifferentiated tumors show large epithelial cells with indistinct borders ("syncytial" growth) and prominent eosinophilic nucleoli.
Epidemiology
- Common among Southern Chinese; rare in the West (<1% of US cancers)
- Strong germline genetic susceptibility in endemic populations
- EBV is a cofactor (not sole cause) - dietary carcinogens (salted fish) and genetic factors also contribute
Clinical Use of EBV in NPC
- Plasma EBV DNA can be used to monitor treatment response and predict prognosis
- EBV serology (anti-VCA IgA, anti-EA IgA) used for screening in endemic areas
Treatment
- Early stage (T1-T2): definitive radiotherapy (RT) alone; local control 64-95%
- Locally advanced: concurrent chemoradiotherapy (CRT), with or without induction/adjuvant chemotherapy
- IMRT is now standard: preserves parotid glands, reduces xerostomia, protects brainstem/chiasm in skull base involvement
- Intergroup 00-99 study: CRT + adjuvant chemo vs. RT alone → 3-year OS 78% vs. 47% (p=0.005)
- Distant metastases remain the dominant mode of failure (up to 30%)
- Immune checkpoint inhibitors: responses reported - new strategy for refractory tumors (leveraging T-cell response to viral antigens)
3. NK/T-Cell Lymphoma, Nasal Type (ENKL)
Also known historically as "lethal midline granuloma" or angiocentric lymphoma.
Key Features
- Virtually all cases are EBV-associated - one of the strongest EBV-tumor associations
- Predominantly affects young to middle-aged adults with male predilection
- Common in East Asia and Latin America
Presentation
- Nasal mass, obstruction, epistaxis
- Palatal destruction
- Erythema and swelling of the face
- Perivascular infiltration → vascular occlusion → massive tissue necrosis (the hallmark)
- Due to necrosis: multiple biopsies often needed to make diagnosis
Diagnosis
- IHC: CD56 positive; EBV positive (in situ hybridization with EBER-1 or EBER-2 probes)
- Plasma EBV DNA level: monitors disease status, predicts prognosis
- LMP1 deletion (del-LMP1): predominant EBV strain in this tumor
- CD56+ EBV+ lymphocytes are rarely seen in normal/inflammatory nasal mucosa - important diagnostic clue
Treatment
- Historically RT was mainstay; high response rate (60-80%) but high relapse rate (~50%)
- Modern regimens incorporate chemotherapy: SMILE (dexamethasone, methotrexate, ifosfamide, L-asparaginase, etoposide)
- More than 80% present with stage I-IIE disease
4. Other EBV-Associated ENT/Head and Neck Malignancies
Hodgkin Lymphoma
- EBV is present in Reed-Sternberg cells in a subset of HL (30-50% in Western series)
- Commonly presents with cervical lymphadenopathy in ENT practice
- EBV genome-positive Burkitt lymphoma: endemic form (African) is virtually 100% EBV+
EBV+ DLBCL (Diffuse Large B-Cell Lymphoma)
- Can occur in paranasal sinuses
- EBV association particularly strong in HIV/immunosuppressed patients and in elderly (EBV+ DLBCL of the elderly)
- Paranasal sinus DLBCL: usually maxillary sinus, often extends to orbit
Post-Transplant Lymphoproliferative Disorder (PTLD)
- EBV-associated lymphoproliferative disorders are a major complication in immunodeficient/post-transplant patients
- Head and neck (tonsils, adenoids) is a common primary site
Chronic Active EBV Infection (T/NK-cell type)
- Systemic EBV+ T-cell and/or NK-cell proliferation; no morphologic features of neoplasm
- Most commonly reported in East Asia
- Can progress to overt NK/T-cell lymphoma
5. Oral Hairy Leukoplakia (OHL)
- White, corrugated, hyperkeratotic lesion on the lateral tongue
- Caused by EBV (lytic infection) of oral epithelial cells
- Diagnosis confirmed by identifying EBV on biopsy
- Typically asymptomatic
- Strongly associated with HIV infection - its presence in a previously healthy individual should prompt HIV workup
- No malignant transformation potential
- Differential diagnosis: lichen planus, idiopathic leukoplakia, carcinoma in situ
EBV Serology Summary
| Antibody | Interpretation |
|---|---|
| VCA-IgM | Acute primary EBV infection (gold standard) |
| VCA-IgG | Past infection / immunity |
| Anti-EA (early antigen) IgG | Active replication (acute or reactivation) |
| EBNA IgG | Appears 6-8 weeks after onset; confirms past infection |
| Heterophile antibodies (Monospot) | Screening test; useful but not EBV-specific |
| Anti-VCA IgA / anti-EA IgA | NPC screening (endemic areas) |
| Plasma EBV DNA (PCR) | NPC and ENKL monitoring, disease burden |
Third-Window EBV Oncological Risk Summary
Oncological risks following EBV infection / IM:
- Nasopharyngeal carcinoma (cofactor)
- Hodgkin disease (Reed-Sternberg cells EBV+)
- Burkitt lymphoma (genome-positive; endemic form ~100% EBV+)
- NK/T-cell lymphoma (nasal type; ~100% EBV+)
- EBV+ DLBCL
- Post-transplant lymphoproliferative disorders
- Gastric carcinoma (non-ENT but EBV-associated)
- Multiple sclerosis (recent evidence of association)
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 3, pp. 843-845 (IM in adults - systemic manifestations, diagnosis, treatment)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 3, pp. 1050-1051 (IM in laryngology context)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 2, pp. 8907-8912 (IM as acute tonsillitis)
- Cummings Otolaryngology Head and Neck Surgery, pp. 2278-2280 (NPC treatment, IMRT)
- Cummings Otolaryngology Head and Neck Surgery, pp. 1553-1574 (ENKL, DLBCL of paranasal sinuses)
- Robbins & Kumar Basic Pathology, pp. 398-400 (EBV pathogenesis, IM, NPC)
- K.J. Lee's Essential Otolaryngology, pp. 63, 215-221 (SSCD; OHL; Lymphoma)
Parotid gland anatomy
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Excellent - I now have rich detail from four major textbooks plus two anatomical images. Here is the complete overview:
Parotid Gland Anatomy
Embryology
- The parotid develops first among the major salivary glands (weeks 6-8 of gestation), as an outpouching of oral ectoderm growing posteriorly toward the ear
- As the gland develops, the facial nerve advances anteriorly, and the gland grows around it - this is why the facial nerve is embedded within the parotid
- Uniquely, the parotid is the last gland to be encapsulated, after lymphatics have already developed. This results in lymphatics becoming trapped within the gland parenchyma and salivary epithelial cells being included within intraparotid lymph nodes
- This embryological quirk explains the development of Warthin's tumors and lymphoepithelial cysts within the parotid (conditions not seen in submandibular or sublingual glands, which encapsulate before lymphogenesis)
General Features
- Largest of the major salivary glands
- Weight: ~25 g, irregularly lobulated
- Shape: wedge-shaped on coronal section
- Secretion type: predominantly serous (only a few mucous acini) - produces watery saliva and salivary amylase
- Unique feature: only salivary gland containing intraglandular lymph nodes (the majority in the superficial lobe)
Extent and Surface Anatomy
| Border | Relationship |
|---|---|
| Superior | Zygomatic arch |
| Inferior | Upper part of neck; tail overlies posterior belly of digastric and anterior SCM |
| Anterior | Masseter muscle (overlies it) |
| Posterior | Below the EAC, onto the mastoid process and lateral process of C1 |
| Medial/deep | Fills the gap between mandible anteriorly and mastoid/styloid process; extends close to the lateral wall of the oropharynx |
The inferior tail of parotid lies between the ramus of the mandible and the sternocleidomastoid, overlying the digastric.
The deep border abuts the prestyloid compartment of the parapharyngeal space.
Axial MRI showing relationships of the parotid:
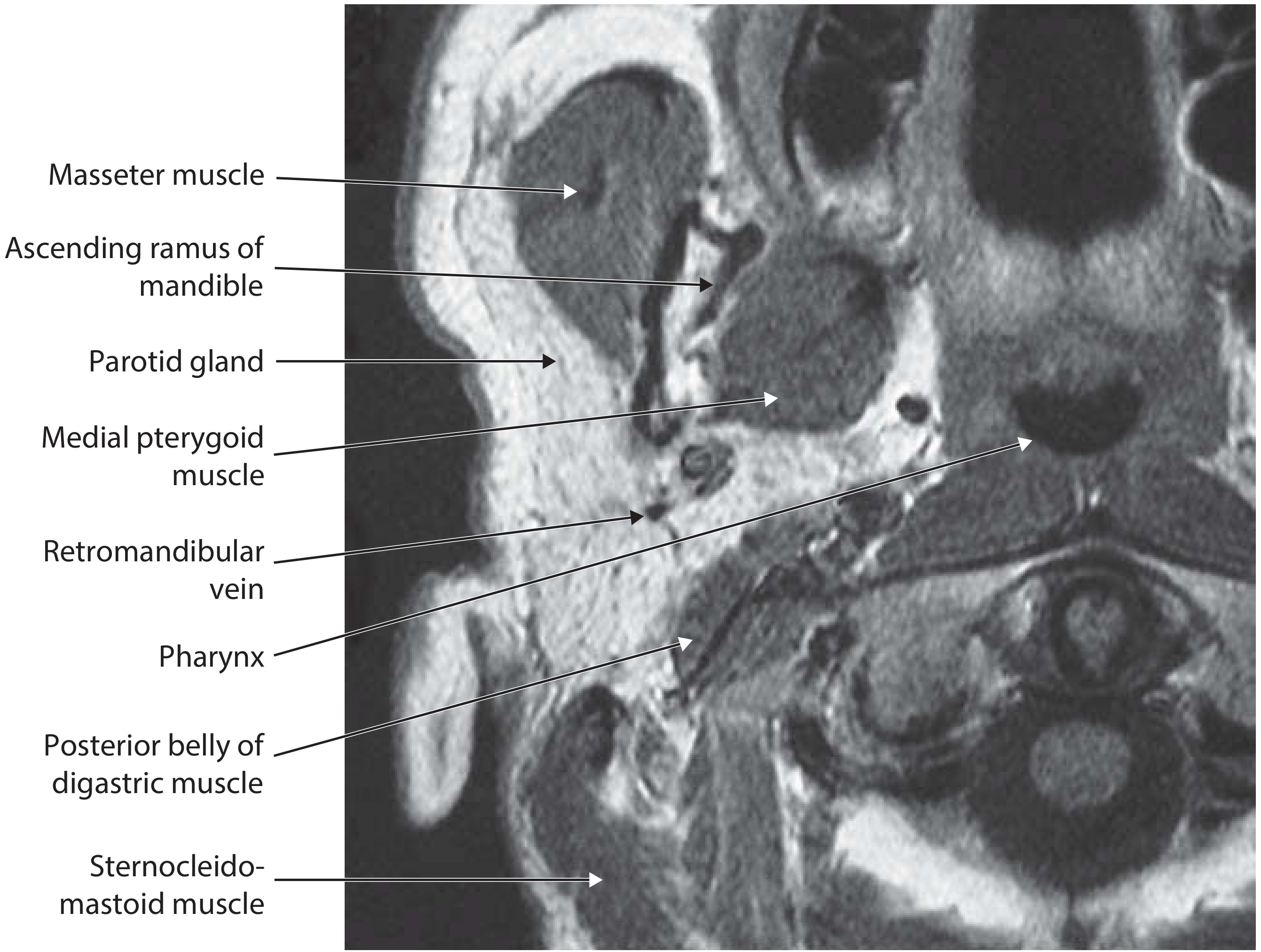
Axial MR showing the wedge-shaped parotid gland, its division into superficial and deep lobes by the retromandibular vein, and its relationships to the masseter, ascending ramus, medial pterygoid, posterior belly of digastric, and SCM - Scott-Brown's Vol. 3
Surface Layers (Superficial to Deep)
- Skin
- Platysma (posterior border)
- Parotid fascia
- Superficial lymph nodes (on or deep to fascia)
- Parotid gland parenchyma
Capsule and Fascia
- The deep cervical fascia splits to enclose the gland - this investment is the parotid fascia (also called parotidomasseteric fascia)
- Continuous anteriorly with the fascia over the masseter
- Extends up to the zygomatic arch superiorly
- The SMAS (superficial musculoaponeurotic system) overlies the gland, adherent to the parotidomasseteric fascia in the pretragal area, becoming separate in the cheek
- The deep part of the fascia extends to the base of skull and is thickened between the styloid process and the angle of the mandible forming the stylomandibular ligament
- The fascia is largely tough and inelastic but thins anteriorly
- Clinical implication: inflammatory oedema and rapidly growing tumours cause the capsule to stretch and become painful before overt enlargement is visible
- The relatively thin fascia over the apex can allow spread of sepsis into the parapharyngeal space
Lobes: Superficial vs. Deep
The facial nerve divides the gland into two "lobes" (primarily a surgical, not embryological, concept):
| Lobe | Volume | Position |
|---|---|---|
| Superficial (lateral) lobe | ~80% | Lateral to plane of facial nerve |
| Deep lobe | ~20% | Medial to plane of facial nerve; extends into the parapharyngeal space |
- The majority of intraglandular lymph nodes are in the superficial lobe
- Deep lobe tumours can extend into the prestyloid compartment of the parapharyngeal space, causing a medial oropharyngeal bulge
- Deep lobe tumours limited by the stylomandibular ligament may expand both superficially and into the parapharyngeal space forming a dumbbell-shaped mass
- Most parotid tumours arise from the superficial lobe
Accessory Parotid Gland
- A separate portion of parotid tissue typically lying on the masseter muscle, between the parotid duct (below) and the zygomatic arch (above)
- Has its own excretory ductule that joins the Stensen duct
- Subject to the same pathologies as the main parotid gland
Parotid Duct (Stensen's Duct)
- Lined by low cuboidal epithelium with a smooth muscle and fibrous tissue wall
- Length: ~5 cm; internal calibre: ~0.6 mm
- Originates within the gland, enveloped by the deep lobe; only small ductules connect the superficial lobe to the duct
- Exits from the anterior border of the gland
- Travels across the masseter muscle (superficially)
- Turns medially at the anterior border of the masseter
- Pierces the buccinator and runs obliquely between buccinator and oral mucosa
- Opens at the parotid papilla on the oral mucosa opposite the second upper molar tooth
- Surface marking: the middle of a line from the intertragal notch of the auricle to the midpoint of the philtrum
- Key relationship: the facial nerve and its branches are always lateral to the parotid duct
Facial Nerve - The Most Important Surgical Structure
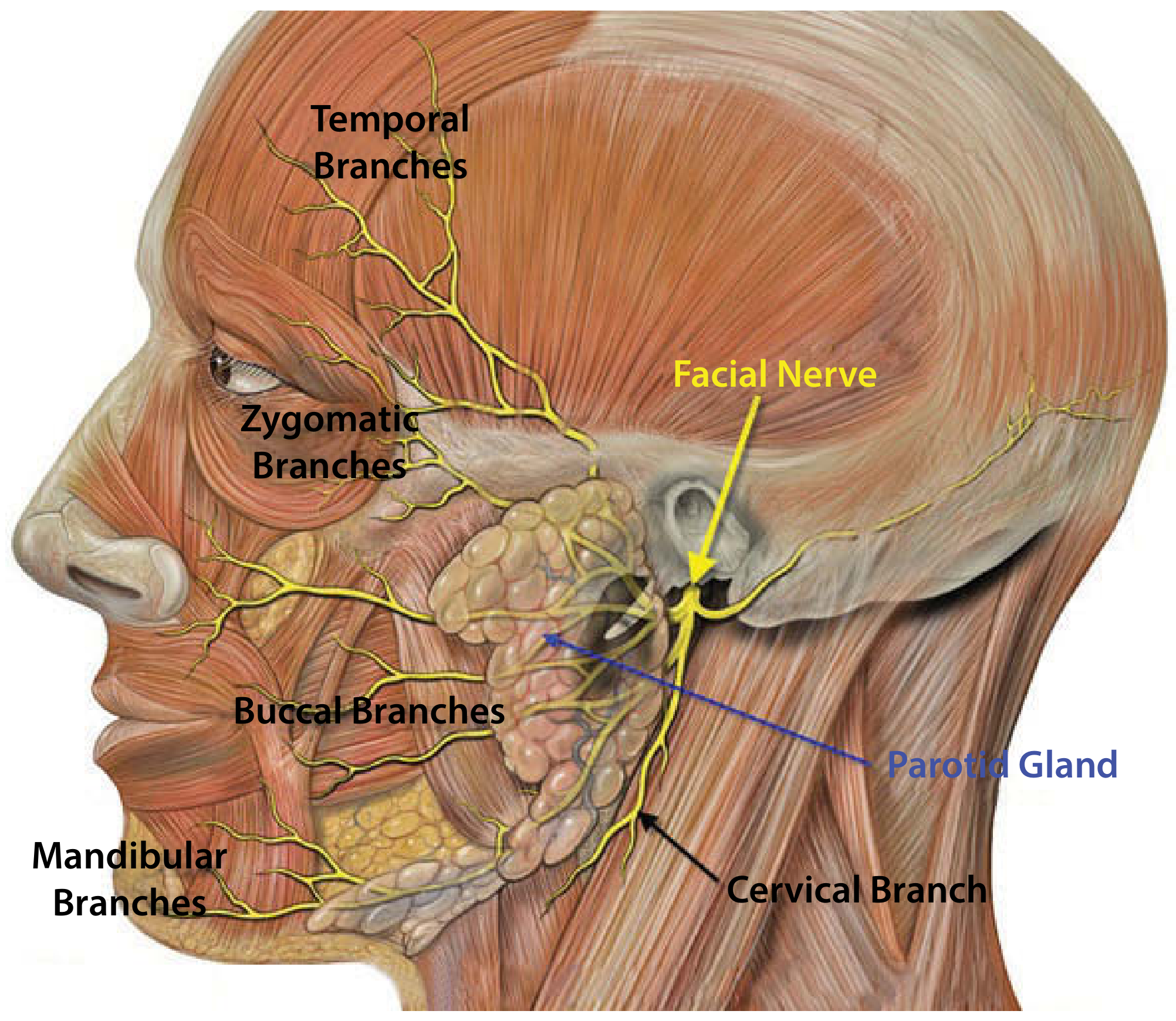
Anatomy of the parotid gland showing the facial nerve entering and dividing within the gland into its five named branches - Scott-Brown's Vol. 3
Entry into the parotid
- Exits the stylomastoid foramen just deep to the junction of the cartilaginous and bony parts of the external auditory meatus
- Usually a single trunk (rarely double - estimated 3-26.7%)
- The main trunk lies approximately 1 cm above the posterior belly of digastric
- Passes downwards and forwards over the styloid process and attached muscles
- Enters the gland high on the posteromedial surface, between the mastoid and styloid processes
- Before entering the gland, gives off:
- Posterior auricular branch - supplies occipital belly of occipitofrontalis
- Muscular branch - supplies posterior belly of digastric and stylohyoid
Division within the parotid
On entering the gland, the main trunk divides into:
- Upper: zygomaticotemporal (upper) division
- Lower: cervicofacial (lower) division
These further subdivide into five terminal branches - the pes anserinus (goose's foot):
| Branch | Muscles Supplied |
|---|---|
| Temporal | Frontalis, upper orbicularis oculi, corrugator |
| Zygomatic | Lower orbicularis oculi, zygomaticus |
| Buccal | Buccinator, orbicularis oris, upper lip muscles |
| Marginal mandibular | Lower lip and chin muscles (depressors) |
| Cervical | Platysma |
Branching patterns
Multiple branching patterns described - Davis and McCormack each described 6 types; Katz and Catalano described 5 types; Kwak et al. described 4 types based on the buccal branch origin.
Cross-innervation
- Most pronounced between zygomatic and buccal branches (extensive anastomoses)
- Least for the marginal mandibular branch (few anastomoses)
- Clinical implication: midfacial movement defects are rare after zygomatic/buccal branch injury due to cross-innervation; marginal mandibular injuries cause predictable lower lip weakness
Spatial relationship to vascular structures
- The facial nerve lies superficial to the retromandibular vein
- The retromandibular vein lies superficial to the external carotid artery
- The retromandibular vein is therefore a useful radiological landmark for localizing the facial nerve on MRI
Blood Supply
Arterial
- External carotid artery courses medial to the parotid and divides within the gland into:
- Maxillary artery - exits the anteromedial surface
- Superficial temporal artery - continues superiorly, exits from the superior surface; gives off the transverse facial artery
Venous
- The maxillary vein and superficial temporal vein unite to form the retromandibular vein within the gland
- The retromandibular vein emerges from the lower pole of the gland and divides into:
- Anterior branch - joins the facial vein → internal jugular vein (lies just deep to the marginal mandibular branch of facial nerve)
- Posterior branch - joins the posterior auricular vein → external jugular vein
Nerve Supply (Innervation)
Parasympathetic (secretomotor)
The complete pathway:
- Preganglionic fibres: inferior salivatory nucleus (medulla)
- → Glossopharyngeal nerve (CN IX)
- → Tympanic branch (Jacobson's nerve) → enters middle ear via tympanic canaliculus → tympanic plexus
- → Lesser superficial petrosal nerve (LSPN)
- → Exits skull base via foramen ovale (or nearby canaliculus)
- → Otic ganglion (ganglion associated with V3, just inferior to foramen ovale) - synapse here
- → Postganglionic fibres travel with the auriculotemporal nerve (branch of V3/mandibular nerve)
- → Parotid gland
Neurotransmitter: acetylcholine - stimulates watery, protein-poor saliva
Sympathetic (vasoconstrictor)
- Superior cervical ganglion → postganglionic fibres
- Follow the external carotid artery plexus and middle meningeal artery plexus
- → Parotid gland
Neurotransmitter: norepinephrine (via α1, α2, β1, β2 receptors on acinar cells)
Sensory
- Auriculotemporal nerve (V3): sensory to the gland
- Great auricular nerve (C2/C3): sensory to the parotid fascia and lower two-thirds of the pinna; divides into anterior and posterior branches. The posterior branch can often be preserved during parotidectomy, reducing post-operative auricular numbness
Clinical correlation - Frey's syndrome (auriculotemporal nerve syndrome)
After parotidectomy, aberrant regeneration of parasympathetic fibres (normally innervating the parotid) into the sympathetic supply of skin sweat glands → sweating and flushing of the overlying skin during eating (gustatory sweating). Acetylcholine is the neurotransmitter for both parasympathetic and (cutaneous) sympathetic fibres, explaining why the misdirected parasympathetic fibres can activate sweat glands.
Lymphatics
- Intraparotid lymph nodes are present (unique to the parotid among salivary glands - due to late encapsulation after lymphogenesis)
- Superficial lymph nodes lie on or deep to the parotid fascia
- The majority of intraparotid nodes are in the superficial lobe
- Parotid nodes receive drainage from the scalp, external auditory canal, pinna, eyelids, and lacrimal gland
- Drain ultimately to upper deep cervical nodes (level II)
- Clinical implication: cutaneous malignancies of the scalp/pinna/face can metastasize to intraparotid nodes; lymphomas can present as parotid masses
Microscopic Anatomy
- Parotid is predominantly serous (small granules, secretes proteins and enzymes including amylase)
- Acinar organization:
- Secretory acini → intercalated ducts (lined by simple low cuboidal epithelium; surrounded by myoepithelial cells) → striated ducts (columnar cells with basal folding; actively transport water and electrolytes) → main excretory duct (lined by tall columnar epithelium)
- Lobules are connected by dense fibrous tissue containing excretory ducts, vessels, lymphatics, nerve fibres and ganglia
Parapharyngeal Extension
- The deep lobe of the parotid extends directly into the prestyloid compartment of the parapharyngeal space (which contains fat, deep lobe tissue, lymph nodes, and branches of V3)
- Deep lobe tumours expanding into this space present as a medial oropharyngeal bulge or a neck mass
- This anatomical extension explains why the oropharynx must always be examined when assessing the parotid gland
Sources:
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery Vol. 3, pp. 721-724 (Parotid gland - clinical anatomy, microscopy, embryology, duct, facial nerve, vessels, nerve supply)
- Cummings Otolaryngology Head and Neck Surgery, pp. 1525, 3787-3789 (Parotid gland; innervation)
- K.J. Lee's Essential Otolaryngology, pp. 641-642 (Parotid anatomy)
- Gray's Anatomy for Students, p. 1052 (Innervation)
Sialendoscopy
Finding Sources
Searching PubMed
"sialendoscopy" AND ("outcomes" OR "technique" OR "salivary")
Reading File
Reading Article
PMID: 37486613
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have thorough material from textbooks and high-quality recent evidence. Here is the comprehensive review:
Sialendoscopy
Definition and Concept
Sialendoscopy is a minimally invasive, endoscopic technique for the diagnosis and treatment of obstructive and inflammatory salivary gland disorders. It uses miniature semirigid or flexible endoscopes to directly visualize the ductal system of the major salivary glands - the parotid (Stensen duct) and submandibular (Wharton duct) - enabling real-time diagnosis and, where instrumented, therapeutic intervention without the need for gland excision.
It represents a paradigm shift in the management of salivary gland disease: conditions previously requiring gland excision (sialadenectomy) can now often be managed by gland-preserving endoscopic techniques.
Historical Context
Sialendoscopy was developed in the 1990s and has been progressively refined with advances in miniaturized optics and instrumentation. It has been successfully adapted for use in the pediatric population - a traditionally challenging group for salivary gland intervention.
Indications
| Category | Specific Indications |
|---|---|
| Sialolithiasis | Parotid and submandibular ductal/hilar stones |
| Ductal stenosis / strictures | Congenital or acquired ductal narrowing |
| Inflammatory / obstructive conditions | Chronic or acute sialadenitis of parotid or submandibular glands |
| Juvenile Recurrent Parotitis (JRP) | Most common paediatric indication (68.9% of paediatric cases) |
| Sjögren syndrome | Inflammatory ductal changes; stenosis |
| Ductal abnormalities | Polyps, sialodochitis, ductal kinks |
| Diagnostic | Unexplained salivary gland swelling without obvious cause; occult sialolith; undetected by imaging |
| Post-irradiation salivary gland stenosis (RAIS) | Radiation-induced ductal stenosis |
In the paediatric systematic review cited in Cummings: JRP was the most frequent indication (68.9%), followed by sialolithiasis (14.7%).
Contraindications
- Active infection (sialendoscopy is contraindicated in the presence of active infection - risk of spreading infection along the ductal system)
- Trismus limiting access
- Very young/uncooperative patients unable to tolerate local anaesthesia (general anaesthesia required)
Background: Sialolithiasis (Context for Sialendoscopy)
Understanding why sialendoscopy is so valuable requires knowledge of sialolithiasis:
Epidemiology and Distribution
- Sialolithiasis is the most common cause of salivary gland inflammation
- Submandibular gland: most commonly affected (80-90% of stones occur in the Wharton duct)
- Parotid (Stensen) duct: 10-20% of cases
- Sublingual duct: ~1%
Why stones prefer the submandibular gland
- Wharton duct is longer, wider, more tortuous, and angulated against gravity as it courses around the mylohyoid → slower flow, poorer egress
- Submandibular saliva is more viscous with higher calcium and phosphorous concentration
- In the submandibular gland: sialolith formation is often the primary event → stasis → retrograde bacterial migration → sialadenitis
- In the parotid gland: chronic sialadenitis precedes stone formation (inverse relationship)
Stone location
- Parotid: stones most commonly at the hilum or parenchyma
- Submandibular: stones most commonly in the duct
Pre-endoscopy management
- Initial: sialagogues (sour candy, lemon drops, pickles), hydration, local heat, gland massage
- Transoral milking/incision for palpable submandibular stones within 2 cm of the duct orifice
The Sialendoscope: Instrumentation
Types by Rigidity
- Flexible endoscopes - good for navigating curves; smaller working channels
- Semirigid endoscopes - most commonly used; balance between maneuverability and instrument channel capacity
- Rigid endoscopes - limited to straight segments
Types by Function
- Diagnostic endoscopes: fiberoptic light + image transmission; may include irrigation channel; no working channel for instruments
- Therapeutic endoscopes:
- Compact: single integrated unit combining fiberoptic light, image transmission, working channel, and irrigation channel (cannot be disassembled)
- Modular (semirigid): optical fibers combined as a separate probe inserted into sheaths of various sizes; the space between optical system and sheath wall serves as the irrigation channel
Standard Sizes (Erlangen/Karl Storz system)
- 0.8 mm: light + image + irrigation; no working channel
- 1.1 mm: light + image + irrigation + working channel
- 1.6 mm: light + image + irrigation + working channel (may be too large for some paediatric patients)
The working channel accommodates:
- Microdrill - for stone fragmentation
- Holmium laser fiber - for larger stone fragmentation
- Balloon dilator - for ductal stenosis
- Wire basket - for stone fragment extraction

Wire basket retrieving a submandibular stone - Cummings Otolaryngology p. 3882
Marchal model (Karl Storz semirigid series): has a slight bend near the distal tip, aiding steering in certain situations but reducing the usable working channel diameter.
Surgical Technique
Anaesthesia
- General anaesthesia is standard
- Local anaesthesia feasible in cooperative children ≥8 years
- For adults: increasingly performed under local anaesthesia in an office-based setting
Steps
1. Positioning and preparation
- Appropriate bite block placed on the contralateral side
- Topical mucosal anaesthesia to the papilla (if local anaesthesia)
2. Papilla identification and dilation
- Identify the salivary duct papilla (Stensen duct: opposite second upper molar; Wharton duct: floor of mouth)
- Serial dilation using salivary duct probes and dilators
- Note: Wharton duct is more difficult to cannulate than Stensen duct
3. Endoscope introduction
- Sialendoscope introduced via the dilated orifice through an introducer sheath
- Attached to camera and monitor for real-time visualisation
4. Ductal exploration
- Under continuous saline irrigation (maintains lumen patency and clears secretions/debris)
- Advanced to the first branching point; each branch explored as far as the scope can comfortably pass
- Ductal system assessed for:
- Sialoliths (size, location, mobility)
- Stenoses / strictures
- Mucosal changes (polyps, sialodochitis, erythema)
- Ductal kinks
5. Intervention (as needed)
| Finding | Intervention |
|---|---|
| Small stone (≤5 mm) | Wire basket retrieval |
| Large stone (>5 mm) | Holmium laser fragmentation or intraductal pneumatic lithotripsy, then basket retrieval |
| Ductal stenosis | Balloon dilatation |
| Impacted/large stone | Combined (hybrid) approach (endoscope localises the stone; external or intraoral incision used to extract) |
6. Post-procedure
- Temporary ductal stent may be placed (especially in Stensen duct after manipulation, to prevent stricture)
Approaches: Pure Endoscopic vs. Combined
Pure Endoscopic
- Stone visualised and retrieved entirely through the working channel
- Limited to stones that can be captured in the wire basket or fragmented to basket-retrievable size
Combined (Hybrid) Approach
- Endoscope localises the stone (or ultrasound used for localisation)
- A small external or intraoral incision is made over the stone location to extract it
- Success rate for endoscope-assisted transoral removal: 86.3% (meta-analysis)
- Particularly useful for large or impacted stones
- Combined approach for parotid gland: 78.2% success rate
Lithrotripsy Modalities
Intracorporeal Lithotripsy
- Holmium laser: delivers laser energy through a fiberoptic cable passed through the working channel; can fragment most stones safely including large ones; preferred modality
- Pneumatic lithotripsy (microdrill): intraductal compressive fragmentation; gaining experience in recent years
Extracorporeal Lithotripsy (ESWL)
- Compressive shock waves focused via acoustic lenses → stone fragmentation
- Not FDA-approved in the United States
- Residual stone fragments can be subsequently removed by sialendoscopy
Specific Conditions and Sialendoscopy
Ductal Stenosis
- Balloon dilatation is the primary therapeutic manoeuvre
- May be primary (inflammatory) or secondary to irradiation (RAIS)
- Success rate for stenoses: 56.3% (lower than for stone disease - more variable outcomes)
Juvenile Recurrent Parotitis (JRP)
- Sialendoscopy is both diagnostic (confirms ductal ectasia) and therapeutic
- Treatment: irrigation + corticosteroid instillation through the working channel
- Success rate: 67.0%
Sjögren Syndrome / Chronic Inflammatory Disease
- Sialendoscopy + intraductal steroid irrigation used to manage ductal stenosis
- Post-irradiation salivary gland stenosis (RAIS): lowest success rate (45.8%)
Diagnostic Role
- Locates stones not detected by ultrasound, CT, or MRI
- Identifies ductal pathology that explains unexplained salivary gland swelling
- Reveals ductal polyps, sialodochitis, kinks
Outcomes: Evidence-Based
Systematic review and meta-analysis (Beumer et al., Oral Diseases, 2024 - PMID 37486613)
- 91 studies, 8,218 patients, 9,043 procedures
- Weighted pooled success rate: 80.9% overall
| Subgroup | Success Rate |
|---|---|
| Sialolithiasis (all) | 89.6% |
| Submandibular gland | 88.3% |
| Parotid gland | 81.2% |
| Endoscope-assisted transoral stone removal | 86.3% |
| Combined approach (parotid) | 78.2% |
| Juvenile Recurrent Parotitis | 67.0% |
| Ductal stenosis | 56.3% |
| Post-irradiation stenosis (RAIS) | 45.8% |
| Incidence of sialadenectomy (gland removal) | 0-14% |
| Major complications | None reported |
The success rate has not considerably changed over the last 9 years, indicating a mature technique with stable outcomes.
Complications
- Ductal perforation: most common complication (especially in paediatric series)
- Ductal avulsion
- Temporary ductal swelling / post-procedural sialadenitis
- Transient pain
- Ductal stenosis (particularly after Stensen duct incision/manipulation - hence stenting is important)
- Nerve injury: rare
No major complications have been reported in large meta-analytic data.
Paediatric Sialendoscopy
- Effective and feasible in children
- General anaesthesia typically required (local anaesthesia possible in cooperative children ≥8 years)
- The 1.6-mm telescope may occasionally be too large for some paediatric patients → smaller scopes (0.8-1.1 mm) preferred
- Indications: JRP (most common - 68.9%), sialolithiasis (14.7%)
- Long-term results are excellent: children treated for sialolithiasis remained free of recurrent swelling at 4-8 year follow-up
Advantages over Traditional Surgery
| Traditional approach | Sialendoscopic approach |
|---|---|
| Sialadenectomy (gland removal) | Gland preservation |
| General anaesthesia required | Can be done under local anaesthesia (adults) |
| External scar / incision | No external incision (or minimal incision in combined approach) |
| Risk of lingual/facial nerve injury | Low complication rate |
| Loss of salivary function | Salivary function preserved |
| Long recovery | Short recovery |
Office-Based Sialendoscopy
A growing trend (reviewed in Otolaryngol Clin North Am, 2025 [PMID 40133106]) is performing sialendoscopy in an office/clinic setting under local anaesthesia, which:
- Reduces costs and avoidance of general anaesthesia
- Enables repeat procedures if needed
- Suitable for diagnostic procedures and small stone retrieval
Sources:
- Cummings Otolaryngology Head and Neck Surgery, pp. 1487-1488 (Sialolithiasis and sialendoscopy); pp. 3880-3883 (Paediatric sialendoscopy chapter)
- K.J. Lee's Essential Otolaryngology, pp. 650-651 (Sialadenitis and sialendoscopy)
- Beumer LJ et al. "Success rate of sialendoscopy. A systematic review and meta-analysis." Oral Dis, 2024. [PMID: 37486613 - 91 studies, n=8218]
- Rahmati RW. "Office-Based Sialendoscopy." Otolaryngol Clin North Am, 2025. [PMID: 40133106]
- Teng TZJ et al. "Steroid Use in Sialendoscopy - A Systematic Review." Clin Otolaryngol, 2026. [PMID: 41501981]
This is a shared conversation. Sign in to Orris to start your own chat.