When to say aki and when to say ckd
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a thorough breakdown of when to use each term, grounded in KDIGO criteria from the textbooks.
AKI vs CKD - When to Use Each Term
The single most important separator is time. Everything else follows from that.
AKI - Acute Kidney Injury
Say AKI when the drop in kidney function is abrupt and recent, meeting ANY of these KDIGO criteria:
| Criterion | Threshold |
|---|---|
| Rise in serum creatinine (SCr) | ≥ 0.3 mg/dL within 48 hours |
| Rise in SCr from baseline | ≥ 1.5x baseline within 7 days |
| Urine output (oliguria) | < 0.5 mL/kg/h for ≥ 6 consecutive hours |
Functionally: AKI = increase in SCr by 50% within 7 days, OR increase by 0.3 mg/dL within 2 days, OR oliguria.
Structurally: AKI has NO structural criteria - it is a purely functional diagnosis.
Classic clinical settings for AKI:
- Sepsis, hypotension, major surgery (ischemia/prerenal)
- Nephrotoxic drugs (aminoglycosides, NSAIDs, contrast, cisplatin)
- Rhabdomyolysis, crush injury, hemolysis
- Obstruction (post-renal) - sudden anuria, flank pain
CKD - Chronic Kidney Disease
Say CKD when kidney damage or reduced function has been present for > 3 months, meeting either:
| Criterion | Threshold |
|---|---|
| Functional | GFR < 60 mL/min/1.73m² for > 3 months |
| Structural | Kidney damage (proteinuria, hematuria, imaging abnormality, biopsy findings) for > 3 months |
KDIGO 2012 defines CKD as: "abnormalities of kidney structure or function, present for more than 3 months, with implications for health." It is classified by cause + GFR category + albuminuria category (CGA).
Classic CKD settings:
- Diabetic nephropathy (most common cause)
- Hypertensive nephrosclerosis
- Glomerulonephritis
- Polycystic kidney disease
- Recurrent AKI leading to fibrosis
The Overlap Zone - AKD (Acute Kidney Disease)
KDIGO introduced a third term to handle the gray zone:
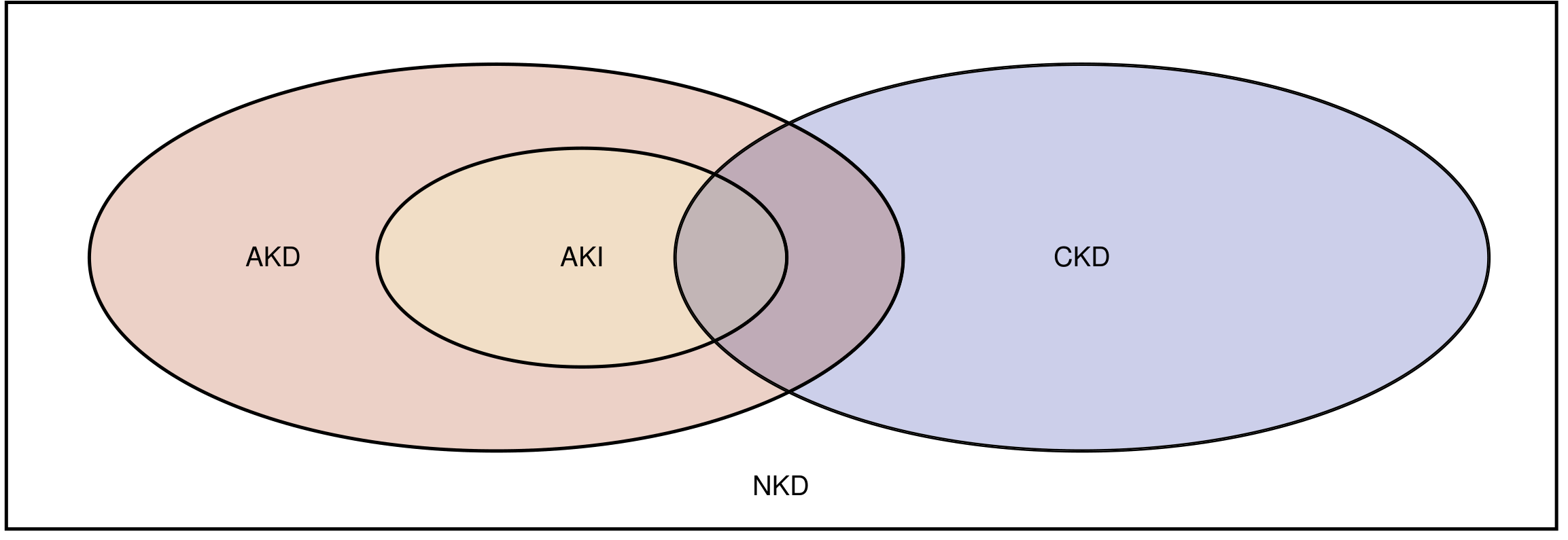
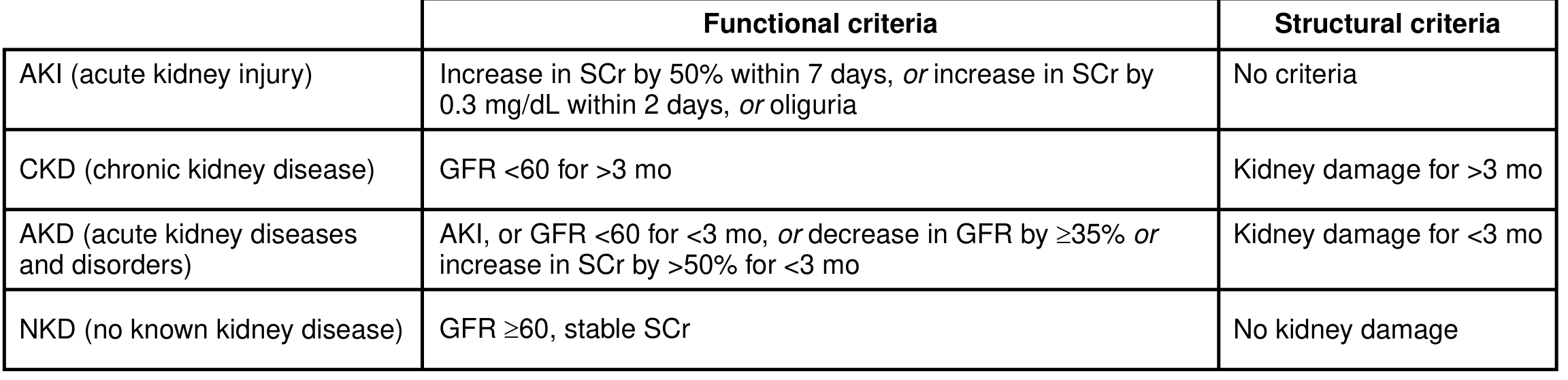
- AKD (Acute Kidney Disease): Kidney damage or GFR < 60 for < 3 months, or SCr increase > 50% for < 3 months. Used when the problem is subacute - lasting beyond 7 days but not yet 3 months.
- NKD (No Known Disease): GFR ≥ 60, stable SCr, no structural damage.
The Tricky Situation - "Acute on Chronic"
When a patient has known CKD and then gets an acute insult, you say "AKI on CKD". This is common:
- CKD is an independent risk factor for AKI
- Baseline SCr may not be known, making it hard to define how acute the rise is
- In absence of a known baseline, KDIGO recommends back-calculating SCr assuming eGFR of 75 mL/min/1.73m² - but this can mislabel undiagnosed CKD as AKI
Quick Decision Guide
| Scenario | Label |
|---|---|
| SCr rose 0.4 mg/dL over 24 hours after surgery | AKI |
| SCr has been 2.1 for 6 months, GFR 35 | CKD |
| Known CKD, SCr jumped acutely on admission | AKI on CKD |
| SCr elevated for 6 weeks, cause unclear | AKD (not yet CKD) |
| GFR ≥ 60, stable, no proteinuria | NKD |
| Diabetic patient, albuminuria 2g/day, GFR 55 for 4 months | CKD (high risk of progression) |
Sources: National Kidney Foundation Primer on Kidney Diseases 8e (KDIGO AKI/AKD definitions); Campbell Walsh Wein Urology (CKD/AKI definitions and overlap); Brenner and Rector's The Kidney (AKI-CKD epidemiology).
When to give what type of iv fluids
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Now I have enough from all sources for a thorough, well-organized answer.
When to Give Which IV Fluid
The right fluid depends on what you're replacing, the clinical goal, and the patient's electrolyte and acid-base status. Here is a systematic breakdown.
1. Composition Reference Table
| Fluid | Na+ | Cl- | K+ | Other | Osmolality | pH |
|---|---|---|---|---|---|---|
| 0.9% NaCl (Normal Saline) | 154 | 154 | - | - | 308 | 5.5 |
| Lactated Ringer's (LR) | 130 | 109 | 4 | Lactate 28, Ca²⁺ | 273 | 6.5 |
| Plasma-Lyte | 140 | 98 | 5 | Acetate + gluconate | 294 | 7.4 |
| 0.45% NaCl (Half Normal) | 77 | 77 | - | - | 154 | 5.5 |
| 5% Dextrose (D5W) | 0 | 0 | - | 50g glucose | 252 | 4.0 |
| 3% NaCl (Hypertonic Saline) | 513 | 513 | - | - | 1026 | 5.0 |
| 20-25% Albumin | - | - | - | Oncotic protein | High | ~7.0 |
2. Crystalloids
Balanced Crystalloids - Lactated Ringer's / Plasma-Lyte (DEFAULT first choice for most scenarios)
Use when:
- Sepsis / septic shock - LR or Plasma-Lyte preferred over NS; reduces hyperchloremic acidosis and improves outcomes including survival benefit (Rosen's Emergency Medicine)
- Acute pancreatitis - LR is the explicitly preferred resuscitation fluid (IAP/APA guidelines); goal-directed 5-10 mL/kg/hr
- Surgical/perioperative fluid - balanced crystalloids preferred over NS for intraoperative replacement
- Burns (Parkland formula) - LR is the standard: TBSA% × weight(kg) × 4 mL, half in first 8 hours, half in next 16 hours
- General volume resuscitation in most hospitalized patients
- Hypovolemia with metabolic acidosis - LR/Plasma-Lyte avoid worsening the acidosis
- Patients already receiving large volumes - switch to balanced if giving >2L total
Why NOT normal saline instead? Large volumes of NS cause hyperchloremic metabolic acidosis (SID = 0), which can worsen renal function, impair immune function, and in rhabdomyolysis, exacerbate myoglobin tubular precipitation and hyperkalemia risk.
0.9% Normal Saline - Specific Use Cases
Use when:
- Hyponatremia (mild to moderate) - isotonic saline to correct sodium gently
- Hypochloremic metabolic alkalosis - e.g., prolonged vomiting (nasogastric losses are Cl-rich); NS replaces the lost chloride and corrects the alkalosis
- Diabetic Ketoacidosis (DKA) - initial resuscitation with NS (first 1-2 L), then switch to 0.45% or balanced
- Blood transfusion compatibility - only NS is compatible with packed red cells (LR contains Ca²⁺ that can cause clotting in blood lines)
- Hypovolemia with hyponatremia
- Patients with ESRD (use cautiously) - historically taught because LR contains K⁺; however, the K⁺ in LR (4-5 mEq/L) is low and unlikely to cause hyperkalemia - balanced crystalloids are increasingly acceptable even in ESRD (Miller's Anesthesia)
Avoid NS when: metabolic acidosis is already present, large volumes needed, sepsis, renal dysfunction.
0.45% NaCl (Half Normal Saline)
Use when:
- Free water deficit / hypernatremia - hypotonic fluid replaces pure water loss
- Diabetic hyperosmolar state (HHS) - after initial volume stabilization with NS
- Maintenance fluids when only partial sodium replacement is needed
- DKA - after initial NS bolus and once glucose <250 mg/dL, switch to D5-0.45% NS
5% Dextrose (D5W)
Distributes throughout total body water - provides free water, essentially no volume effect.
Use when:
- Hypoglycemia - D50W bolus (20-50 mL) for severe/altered consciousness; then D5W infusion to maintain
- Hyperkalemia treatment - D50W (50 mL of 50% dextrose) with 10 units regular insulin to shift K⁺ into cells; followed by D5W infusion to prevent rebound hypoglycemia
- Free water replacement (hypernatremia with pure water deficit)
- Drug dilution vehicle - many IV medications are reconstituted in D5W
- DKA maintenance - once glucose drops to 200-250 mg/dL, add dextrose to prevent hypoglycemia while continuing insulin
Do NOT use for volume resuscitation - it has no sustained intravascular effect and causes hyponatremia in large volumes.
3% Hypertonic Saline
Use when:
- Severe symptomatic hyponatremia (seizures, coma, altered consciousness) - 100-150 mL bolus of 3% NaCl; raises Na⁺ by ~2 mEq/L per 100 mL bolus; correct no faster than 1-2 mEq/L/hr
- Raised intracranial pressure (ICP) - traumatic brain injury, cerebral edema; draws water out of brain tissue osmotically; alternative to mannitol
- Cerebral herniation - emergent ICP reduction
Caution: Central pontine myelinolysis if Na⁺ corrected too fast (> 10-12 mEq/L in 24 hours). Always via central line if >2%.
3. Colloids
Albumin (4-5% or 20-25%)
Use when:
- Spontaneous bacterial peritonitis (SBP) in cirrhosis - 1.5 g/kg albumin at diagnosis + 1 g/kg on day 3 (prevents hepatorenal syndrome - strong evidence)
- Large-volume paracentesis (>5L) - 6-8 g/kg albumin to prevent post-paracentesis circulatory dysfunction
- Hepatorenal syndrome - combined with terlipressin/vasoconstrictors
- Severe hypoalbuminemia with ascites
Do NOT use for routine volume resuscitation (no mortality benefit over crystalloids in most settings); crystalloids are favored over colloids for general resuscitation (Harrison's).
4. Blood Products (when crystalloids fall short)
| Product | Use |
|---|---|
| Packed red cells (PRBCs) | Active hemorrhage, Hgb <7 (or <8 in cardiac disease) |
| Fresh Frozen Plasma (FFP) | Coagulopathy, massive hemorrhage; PRBC:FFP ratio ≤ 2:1 in trauma |
| Platelets | Thrombocytopenia with active bleeding, plt <50k pre-procedure |
| Cryoprecipitate | Fibrinogen deficiency, hemophilia A, von Willebrand disease |
In ruptured AAA or trauma with uncontrolled hemorrhage, early 1:1 PRBC:FFP (damage control resuscitation) outperforms large crystalloid volumes, which worsen dilutional coagulopathy and acidosis.
5. Quick Clinical Decision Guide
| Clinical Scenario | First Choice Fluid |
|---|---|
| Sepsis / septic shock resuscitation | LR or Plasma-Lyte (30 mL/kg bolus) |
| Acute pancreatitis | LR (5-10 mL/kg/hr, goal-directed) |
| Major burns | LR (Parkland formula) |
| DKA initial | NS 1-2L, then 0.45% NaCl ± D5 |
| HHS | NS first, then 0.45% NaCl |
| Hypochloremic alkalosis (vomiting) | NS |
| Severe symptomatic hyponatremia | 3% NaCl bolus |
| Raised ICP / cerebral edema | 3% NaCl or Mannitol |
| Hypoglycemia (severe/IV) | D50W bolus → D5W infusion |
| Hyperkalemia (insulin shift) | D50W + insulin, then D5W |
| Cirrhosis + SBP or large paracentesis | Albumin |
| Blood transfusion line | NS only (not LR) |
| Active hemorrhage | PRBCs + FFP |
| Routine surgical maintenance | Balanced crystalloid (LR/Plasma-Lyte) |
Sources: Rosen's Emergency Medicine (balanced crystalloid vs. saline; hypertonic saline); Current Surgical Therapy 14e (sepsis/pancreatitis fluid choice); Bailey and Love's Surgery (burn resuscitation); Miller's Anesthesia 10e (intraoperative fluids, ESRD); Harrison's Principles (AKI fluid replacement, albumin); Washington Manual (dextrose for hypoglycemia); Tintinalli's Emergency Medicine (hyperchloremic acidosis, hypertonic saline).
Pyrexia of unknown origin
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Excellent content from Harrison's and Frameworks for Internal Medicine. Now I have everything needed for a thorough answer.
Pyrexia of Unknown Origin (PUO / FUO)
Definition (Petersdorf & Beeson 1961, updated by KDIGO/ADQI)
The modern definition requires all three:
- Fever ≥ 38.3°C (101°F) on at least two occasions
- Illness duration ≥ 3 weeks
- No known immunocompromised state (immunocompromised patients are a separate category with different workup)
No diagnosis despite initial evaluation. The term should NOT be applied to every febrile illness - most fevers resolve or declare themselves before 3 weeks.
Epidemiology - What Is Most Common By Region?
| Region | Most Common Cause |
|---|---|
| Western Europe / USA | Noninfectious inflammatory diseases (NIIDs) - up to 1/3 of cases |
| South Asia / East Asia | Infections (TB most common - up to 50% of infections in FUO) |
| Any region | 20-50% remain undiagnosed even after full workup ("FUO paradox") |
The "FUO paradox": because CT, MRI, and PET/CT diagnose most fevers within 3 weeks now, only the hardest cases survive to meet FUO criteria - making FUO harder to solve than ever before.
The Four Categories of Causes
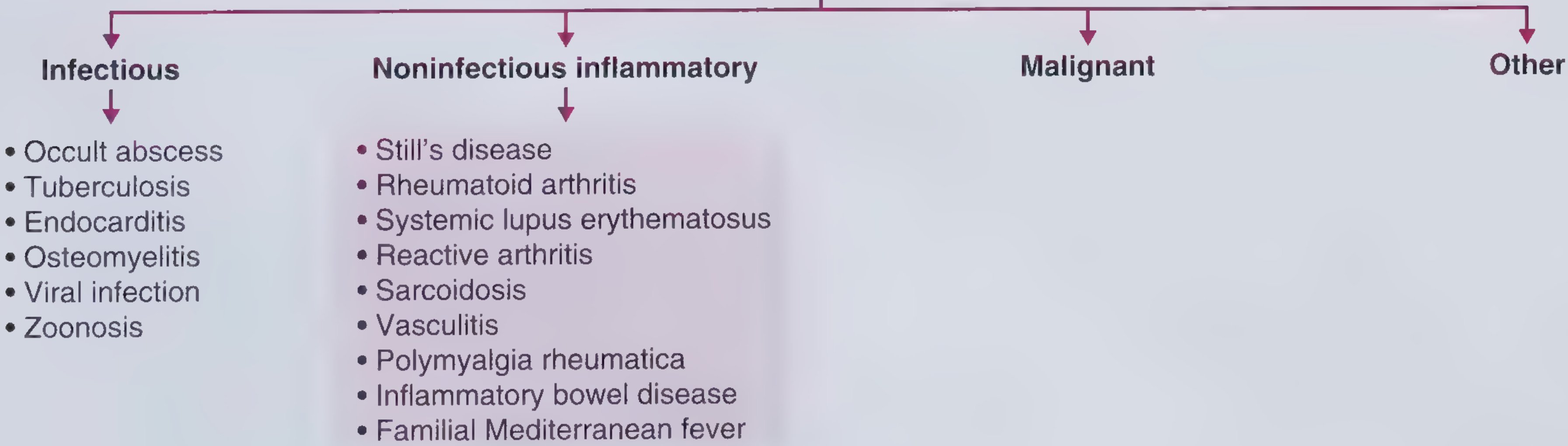
1. Infectious Causes (~15-36% in West; majority in Asia)
| Disease | Key Clue |
|---|---|
| TB (extrapulmonary / miliary) | Immigrant from endemic region, hepatomegaly, miliary nodules on CT, cholestatic LFTs |
| Endocarditis (culture-negative) | Recent dental procedure, new murmur (decrescendo diastolic = aortic regurgitation), negative cultures |
| Intra-abdominal abscess | History of diverticulitis, appendicitis, bowel surgery; focal tenderness; fever weeks later |
| Vertebral osteomyelitis / spondylodiscitis | Back pain + fever, IV drug use, bacteremia |
| Q fever (Coxiella burnetii) | Rural area, animal contact, heart valve disease; serologic IFA testing |
| Whipple's disease (T. whipplei) | Diarrhea + arthralgias + weight loss; PCR/biopsy of duodenum |
| Leptospirosis | Freshwater exposure, conjunctival suffusion, AKI, thrombocytopenia, elevated LFTs |
| Brucellosis | Contact with livestock or unpasteurized dairy |
| Viral (EBV, CMV, HIV) | Lymphadenopathy, pharyngitis, heterophile antibodies, serology |
| Fungal (histoplasmosis, coccidioidomycosis) | Specific geographic/exposure history |
History red flags for infection: country of origin, travel history, animal/zoonotic exposures, sexual history, IV drug use, indwelling hardware, recent procedures, antibiotic history.
2. Noninfectious Inflammatory Diseases (NIIDs) (~up to 33% in West)
| Disease | Key Clue |
|---|---|
| Adult-onset Still's disease (AOSD) | Ferritin dramatically elevated (often >2000 ng/mL), quotidian high fever, evanescent salmon-colored rash, pharyngitis, arthritis; bimodal age (15-25 and 36-46 yr) |
| Giant Cell Arteritis (GCA) | Age >50, headache, jaw claudication, tender/nodular temporal artery, elevated ESR; accounts for ~1/5 of FUO in elderly |
| Polymyalgia Rheumatica (PMR) | Pain/stiffness in shoulder and hip girdle muscles; morning stiffness; dramatic response to steroids; closely associated with GCA |
| SLE | Pancytopenia, low complement, ANA+, young woman |
| Rheumatoid Arthritis | Symmetric polyarticular arthritis (wrists, MCPs, PIPs), RF positive |
| Reactive Arthritis | Sterile arthritis after urethritis (post-STI); urethral discharge history |
| Sarcoidosis | Bilateral hilar lymphadenopathy, elevated ACE, non-caseating granulomas |
| Polyarteritis Nodosa (PAN) | Hep B infection, testicular pain, livedo reticularis, mononeuritis multiplex |
| IBD (Crohn's / UC) | Change in bowel habits, weight loss; diagnosed by colonoscopy; UC more common cause of FUO |
| Familial Mediterranean Fever (FMF) | Autosomal recessive; Mediterranean ethnicity (Arab, Armenian, Turkish, Jewish, North African); recurrent episodes of fever + serositis (peritonitis/pleuritis/synovitis) lasting 1-4 days; first attack usually <10 years; Colchicine is treatment |
History red flags for NIID: morning stiffness >1 hour, arthralgias/myalgias, rash, ocular symptoms, response to steroids, family history of autoinflammatory disorders.
3. Malignant Causes (~7-15%)
| Malignancy | Key Clue |
|---|---|
| Lymphoma (most common, ~1/4 of malignant FUO) | Lymphadenopathy, splenomegaly, elevated LDH; can be purely non-nodal (intravascular lymphoma) - poor prognosis |
| Leukemia (acute > chronic) | Aleukemic leukemia - peripheral smear may be normal; bone marrow biopsy needed |
| Myelodysplastic syndrome (MDS) | Age >50, cytopenias (anemia, thrombocytopenia, neutropenia), macrocytosis |
| Renal Cell Carcinoma | Hematuria, polycythemia, smoker |
| Hepatocellular Carcinoma | Cirrhosis background |
| Colon cancer | Streptococcus gallolyticus (bovis) endocarditis is a classic association |
| Metastatic breast cancer | HER2+ on biopsy |
| Atrial Myxoma | "Tumor plop" sound on auscultation, embolic events |
Note: In patients with known malignancy, infection (not the tumor itself) is still the most common cause of FUO.
4. Miscellaneous / Other Causes
- Drug fever - must always be excluded; stop or replace all medications
- Factitious fever - manipulation of thermometer (exclude early)
- Benign hyperthermia - exclude before extensive workup
- Thromboembolic disease - DVT/PE can cause fever
- Thyroiditis / Subacute thyroiditis - painful thyroid, elevated T4
- Alcoholic hepatitis
- Kikuchi disease - necrotizing lymphadenitis in young Asian women
Diagnostic Approach (Harrison's / KDIGO Structured Protocol)
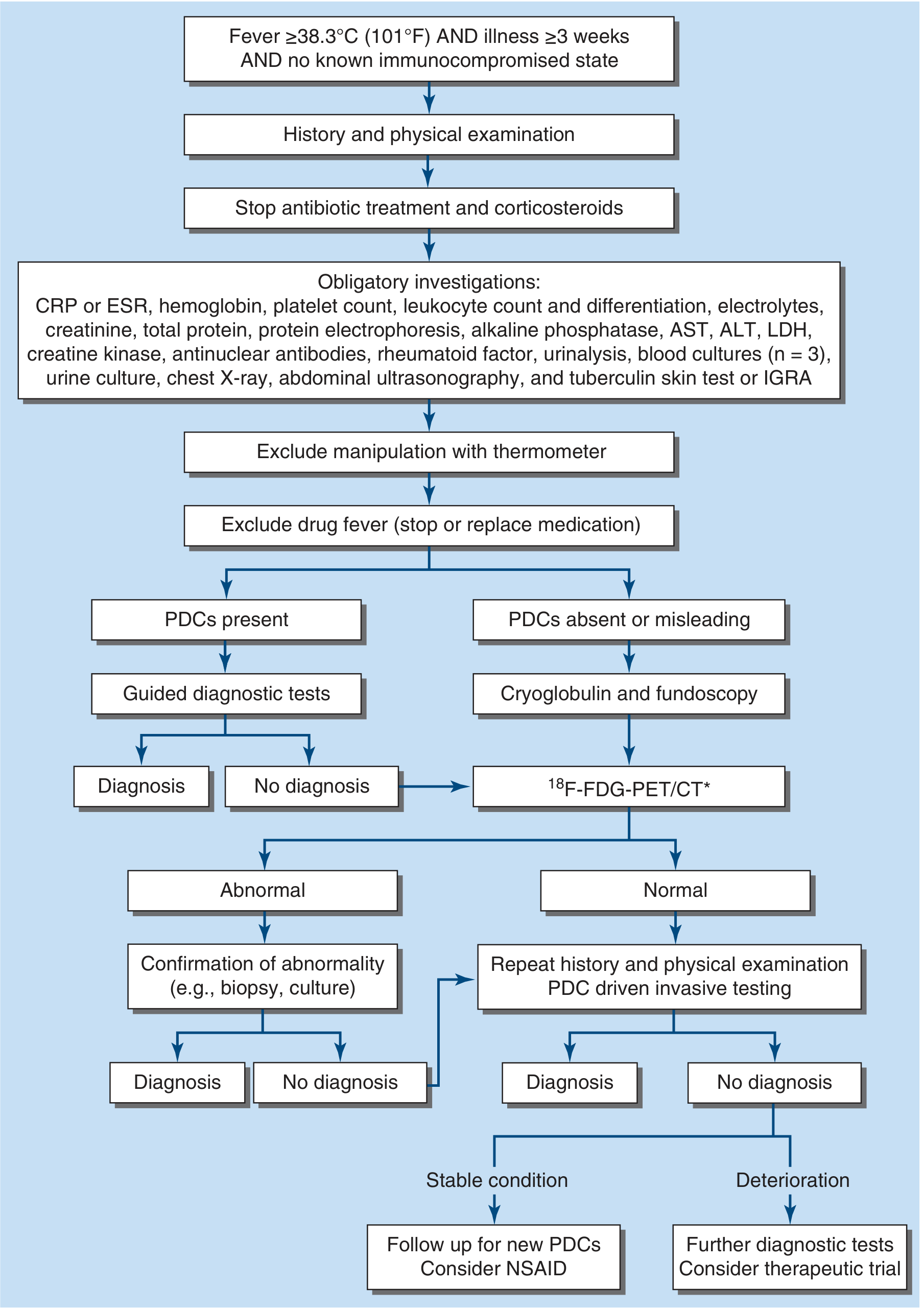
Step 1 - Stop antibiotics and corticosteroids (they mask cultures and shrink lymph nodes)
Step 2 - Obligatory investigations (everyone gets these):
- CRP or ESR, CBC with differential
- Electrolytes, creatinine, LFTs (AST, ALT, ALP), LDH, total protein, protein electrophoresis, creatine kinase
- ANA, rheumatoid factor
- Urinalysis + urine culture
- Blood cultures x3
- Chest X-ray
- Abdominal ultrasound
- Tuberculin skin test (TST) or IGRA
Step 3 - Search for Potentially Diagnostic Clues (PDCs) - all localizing signs, symptoms, and abnormalities
| If PDCs present | If PDCs absent |
|---|---|
| Guided targeted tests based on clue | Cryoglobulins + fundoscopy |
| ↓ | ↓ |
| Diagnosis / no diagnosis | ¹⁸F-FDG-PET/CT (or gallium/labeled leukocyte scintigraphy if unavailable) |
Step 4 - ¹⁸F-FDG-PET/CT is the key advanced imaging:
- If abnormal → confirm with biopsy or culture of that site
- If normal → repeat history and physical; PDC-driven invasive testing
Step 5 - If still no diagnosis:
- Stable: follow up, consider NSAIDs
- Deteriorating: further diagnostics, consider therapeutic trial
Empirical Treatment (use cautiously, only when appropriate)
| Drug | When to trial |
|---|---|
| Antibiotics | Hemodynamic instability or neutropenia |
| Anti-tuberculars | Positive TST/IGRA, granulomatous disease + anergy, endemic area with extrapulmonary TB picture; wait for cultures/PCR first |
| Colchicine | Features of FMF (Mediterranean ethnicity, recurrent serositis); also pericarditis, Behçet's |
| NSAIDs | Persistent fever, no source; AOSD responds dramatically |
| Glucocorticoids | Only after infection and lymphoma are sufficiently excluded; effective for GCA/PMR; risk: masks lymphoma and infections |
| IL-1 inhibitors (Anakinra) | Autoinflammatory syndromes (FMF, CAPS, TRAPS, AOSD); highly effective |
Key rule: Avoid empirical steroids until malignant lymphoma and active infection have been reasonably excluded - steroids can temporarily suppress lymphoma while allowing it to progress.
Prognosis
- Patients who remain undiagnosed after thorough evaluation generally do well - most become symptom-free spontaneously
- Mortality risk is highest during the index admission before diagnosis is made
- FUO of longer duration (>12 months) is less likely to be infection or malignancy, but never zero - lymphoma has been reported even at >12 months
- Normal PET/CT is associated with lower likelihood of finding a final diagnosis
Sources: Harrison's Principles of Internal Medicine 22e (FUO definition, epidemiology, differential, structured approach); Frameworks for Internal Medicine (infectious, inflammatory, and malignant causes with clinical scenarios).
Blood brain axis
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Loading Image
I have rich content now. Let me compile the full answer.
The Blood-Brain Axis
"Blood-brain axis" encompasses two closely related concepts:
- The Blood-Brain Barrier (BBB) - the structural and functional interface between blood and CNS
- The Gut-Microbiome-Brain Axis - the bidirectional communication network between the intestinal microbiome, enteric nervous system, immune system, and the brain (including through the BBB)
Part 1: The Blood-Brain Barrier (BBB)
Structure
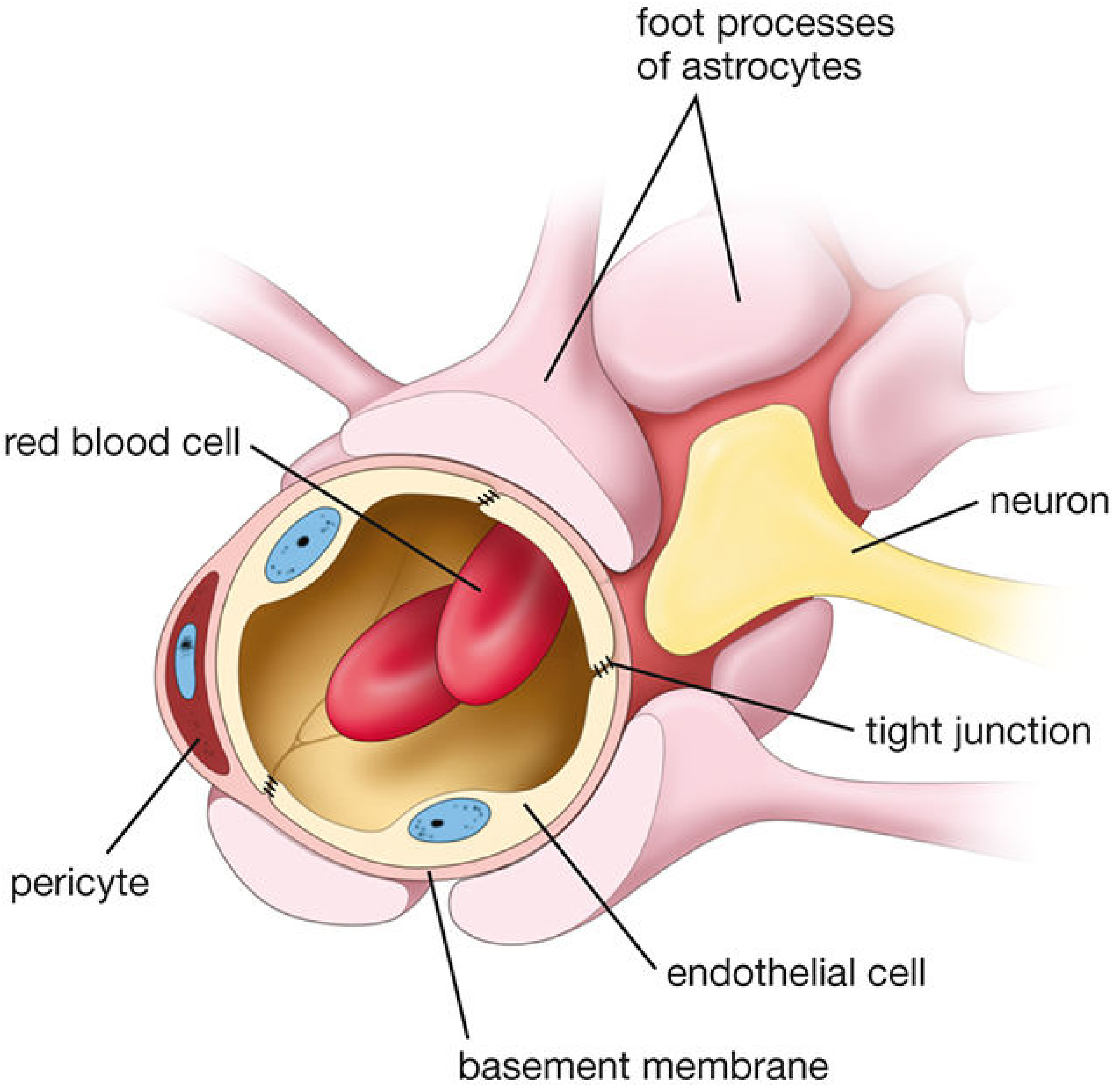
The BBB is formed by four key components working together as the "neurovascular unit":
| Component | Role |
|---|---|
| Endothelial cells (with tight junctions) | Physical barrier - the core of the BBB; unlike systemic capillaries, brain capillaries have NO fenestrations |
| Tight junctions (occludins, claudins, ZO proteins) | Seal gaps between endothelial cells; prevent paracellular diffusion; more like epithelial than typical endothelial junctions |
| Astrocyte end-feet | Ensheath capillaries; release soluble factors that maintain tight junction integrity; regulate water homeostasis via aquaporin-4 (AQP4) channels |
| Pericytes | Embedded in basement membrane; regulate capillary tone and BBB permeability |
The barrier develops embryologically through interaction between glial astrocytes and capillary endothelial cells. The astrocytes don't physically form the barrier - but without their signaling, tight junctions deteriorate.
What Can and Cannot Cross
Freely crosses (no transporter needed):
- O₂, CO₂
- Lipid-soluble molecules: ethanol, steroid hormones, anesthetic agents
- Molecules < 500 Da that are lipophilic
Cannot cross by passive diffusion:
- Most water-soluble drugs and toxins
- Large proteins
- Most ionic substances (including K⁺ - neurons are extremely sensitive to extracellular K⁺ fluctuations)
Crosses via specialized transporters:
| Substance | Transporter |
|---|---|
| Glucose | GLUT1 (SLC2A1) - neurons depend almost exclusively on glucose |
| Amino acids | Cationic amino acid transporters (SLC7A1) |
| Nucleotides, vitamins, ions | Various SLC family transporters |
| L-DOPA (levodopa) | Large neutral amino acid transporter |
| Waste/toxins out | ABC efflux transporters (P-glycoprotein, BCRP) |
Clinical relevance - why L-DOPA and not dopamine?
Dopamine cannot cross the BBB. L-DOPA (its precursor) crosses via amino acid transporters, then is decarboxylated to dopamine inside the brain. This is why Parkinson's disease is treated with levodopa, not dopamine itself. However, dopamine formed from L-DOPA in the endothelial cell also cannot exit back into the brain - the BBB regulates how much L-DOPA reaches neurons.
Circumventricular Organs (CVOs) - Where the BBB is Absent
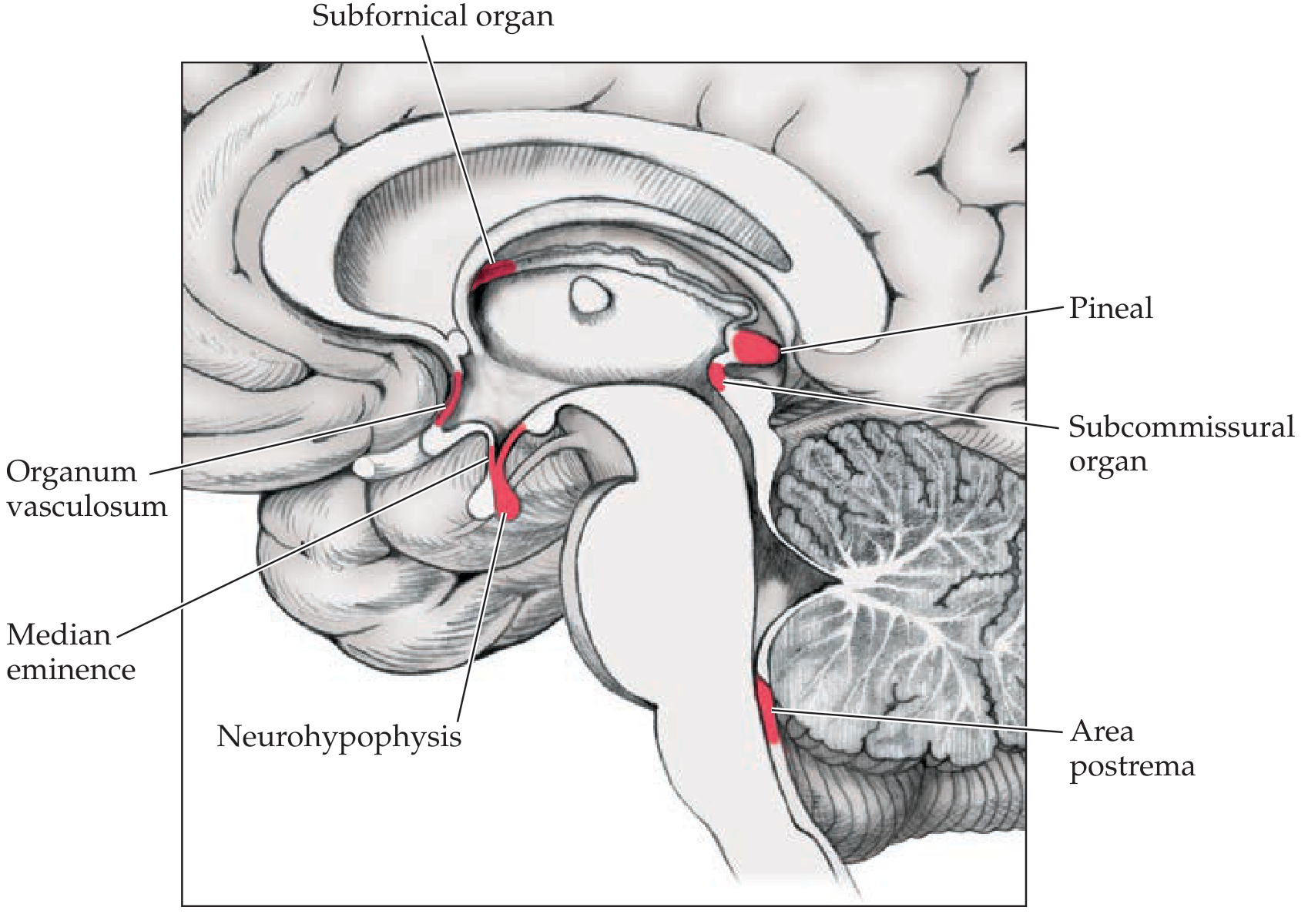
Certain midline brain regions along the 3rd and 4th ventricles intentionally lack a BBB - they have fenestrated capillaries that allow direct blood-to-brain chemical sampling.
| Circumventricular Organ | Function |
|---|---|
| Area postrema (chemoreceptor trigger zone) | Detects circulating emetic toxins → triggers vomiting; only paired CVO; in medulla at caudal 4th ventricle |
| Median eminence | Releases hypothalamic hormones into portal blood to control pituitary |
| Neurohypophysis (posterior pituitary) | Releases AVP (ADH) and oxytocin into systemic circulation |
| Subfornical organ | Detects angiotensin II in blood → regulates fluid balance, thirst, AVP release |
| Organum vasculosum of lamina terminalis | Neuroendocrine functions; detects osmolarity changes and circulating cytokines (fever induction) |
| Pineal gland | Melatonin secretion; circadian rhythm regulation |
| Subcommissural organ | Function not fully established |
These organs are the "windows" of the brain - they sample blood chemistry and relay that information to the protected CNS. Angiotensin II in blood raises BP by acting through the subfornical organ and area postrema (areas outside the BBB).
Blood-CSF Barrier (separate but related)
At the choroid plexus, a different barrier operates:
- Choroid plexus capillaries are freely permeable (fenestrated)
- But the choroid plexus epithelial cells form the real barrier between blood and CSF
- CSF is reabsorbed at arachnoid granulations via giant vacuoles
- Substances pass freely between CSF and brain parenchyma (ependymal layer is open)
This means: blood → choroid epithelium barrier → CSF → ependyma (open) → brain parenchyma
BBB Breakdown in Disease
When the BBB fails, tight junctions are lost and astrocyte morphology changes. This leads to:
| Disease | BBB Role |
|---|---|
| Stroke | Ischemia causes BBB breakdown; cerebral edema from plasma leaking in |
| Meningitis / Encephalitis | Inflammation disrupts tight junctions; allows pathogens and immune cells in |
| Brain tumors | Tumor vasculature lacks proper tight junctions; enhances on contrast MRI |
| Alzheimer's disease | BBB breakdown in hippocampus contributes to neurodegeneration |
| MS (Multiple Sclerosis) | Lymphocyte infiltration across BBB triggers demyelination |
| Osmotic demyelination syndrome | Rapid Na⁺ correction causes cerebral dehydration → BBB breakdown → astrocyte injury → myelinolysis |
| Brain edema (any cause) | AQP4 channels on astrocyte end-feet regulate water entry/exit in edema |
Part 2: The Gut-Microbiome-Brain Axis
The gut and brain communicate bidirectionally through multiple pathways:
Top-Down (Brain → Gut)
- Stress, emotions, and psychological experiences alter gut motility, secretion, and microbiome composition
- The brain influences the enteric nervous system via the autonomic nervous system
- Mouse models: various stressors change gut microbiota composition
Bottom-Up (Gut/Microbiome → Brain)
The intestinal microbiome influences the CNS through at least three routes:
| Route | Mechanism |
|---|---|
| Vagus nerve pathway | Intestinal microbes activate the enteric nervous system → signals travel via vagus nerve → activate stress circuits in the brain |
| Circumventricular organ pathway | Microbial metabolites target CNS areas without a BBB (e.g., hypothalamic-pituitary-adrenal axis) - bypassing the barrier entirely |
| Diffusible molecules | Short-chain fatty acids (SCFAs: butyrate, propionate, acetate) produced by bacteria can cross the BBB and influence neuronal function |
What the Microbiome Does to the Brain
- Programs the HPA (hypothalamic-pituitary-adrenal) axis early in life, shaping stress reactivity across the lifespan
- Influences BBB formation itself during development
- Affects myelination and neurogenesis
- Alters behavior (demonstrated in germ-free mouse models)
Clinical Associations (Human)
| Condition | Microbiome Link |
|---|---|
| Autism spectrum disorder | Altered microbiome composition; gut-brain signaling dysregulation |
| Anxiety and depression | Microbiome modulates serotonin precursors, tryptophan metabolism |
| IBS (irritable bowel syndrome) | Gut-brain axis dysregulation; visceral hypersensitivity; anxiety comorbidity |
| Obesity / Type 2 diabetes | Microbiome regulates energy harvest, satiety hormones (GLP-1), insulin sensitivity |
| Parkinson's disease | Alpha-synuclein pathology may begin in enteric neurons; vagal propagation hypothesis |
| Hepatic encephalopathy | Gut bacteria produce ammonia and other toxins that cross a compromised BBB |
The Circadian Dimension
The microbiota exhibit diurnal fluctuations in composition and function (e.g., butyrate production rhythms). These signal to the molecular clock in the brain and liver, and the circadian clock in turn shapes microbiota composition - making diet timing, sleep, and gut health deeply interconnected.
Drug Implications of the BBB
| Drug | BBB Behavior |
|---|---|
| Domperidone | Does NOT cross BBB - safe antiemetic in Parkinson's (unlike metoclopramide which blocks central dopamine receptors) |
| Levodopa | Crosses via amino acid transporter - used in Parkinson's |
| Most antibiotics | Poor BBB penetration (except chloramphenicol, metronidazole, rifampicin, some fluoroquinolones) |
| Mannitol (IV) | Creates osmotic gradient to reduce cerebral edema |
| Chemotherapy | Most agents excluded by ABC efflux transporters - major challenge in CNS tumors |
Sources: Neuroanatomy through Clinical Cases 3e (BBB structure, circumventricular organs); Histology - A Text and Atlas (tight junctions, astrocytes, transporters, AQP4, CVOs); Sleisenger and Fordtran's GI and Liver Disease (microbiome-gut-brain axis, vagal pathway, SCFAs, HPA programming, behavior and disease links); Robbins & Kumar Basic Pathology (BBB breakdown in disease).
This is a shared conversation. Sign in to Orris to start your own chat.