Angina pectoris ( pharmacology)
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Searching PubMed
angina pectoris pharmacological treatment
I now have all the information needed for a comprehensive response. Let me compile it.
Angina Pectoris — Pharmacology
Overview
Angina pectoris results from an imbalance between myocardial oxygen supply and demand, most commonly due to atherosclerotic coronary artery disease. Three classic forms exist:
| Type | Trigger | Mechanism |
|---|---|---|
| Stable (effort) angina | Physical exertion | Fixed atheromatous plaque → fixed flow limitation |
| Unstable angina | Rest or minimal exertion | Plaque rupture / dynamic obstruction |
| Variant (Prinzmetal) angina | Often at rest | Coronary artery vasospasm |
Pharmacotherapy works by reducing myocardial O₂ demand (↓ heart rate, preload, afterload, contractility) and/or increasing O₂ supply (coronary vasodilation, relief of spasm).
Drug Groups
1. Organic Nitrates & Nitrites
Prototype: Nitroglycerin (glyceryl trinitrate)
Mechanism of Action:
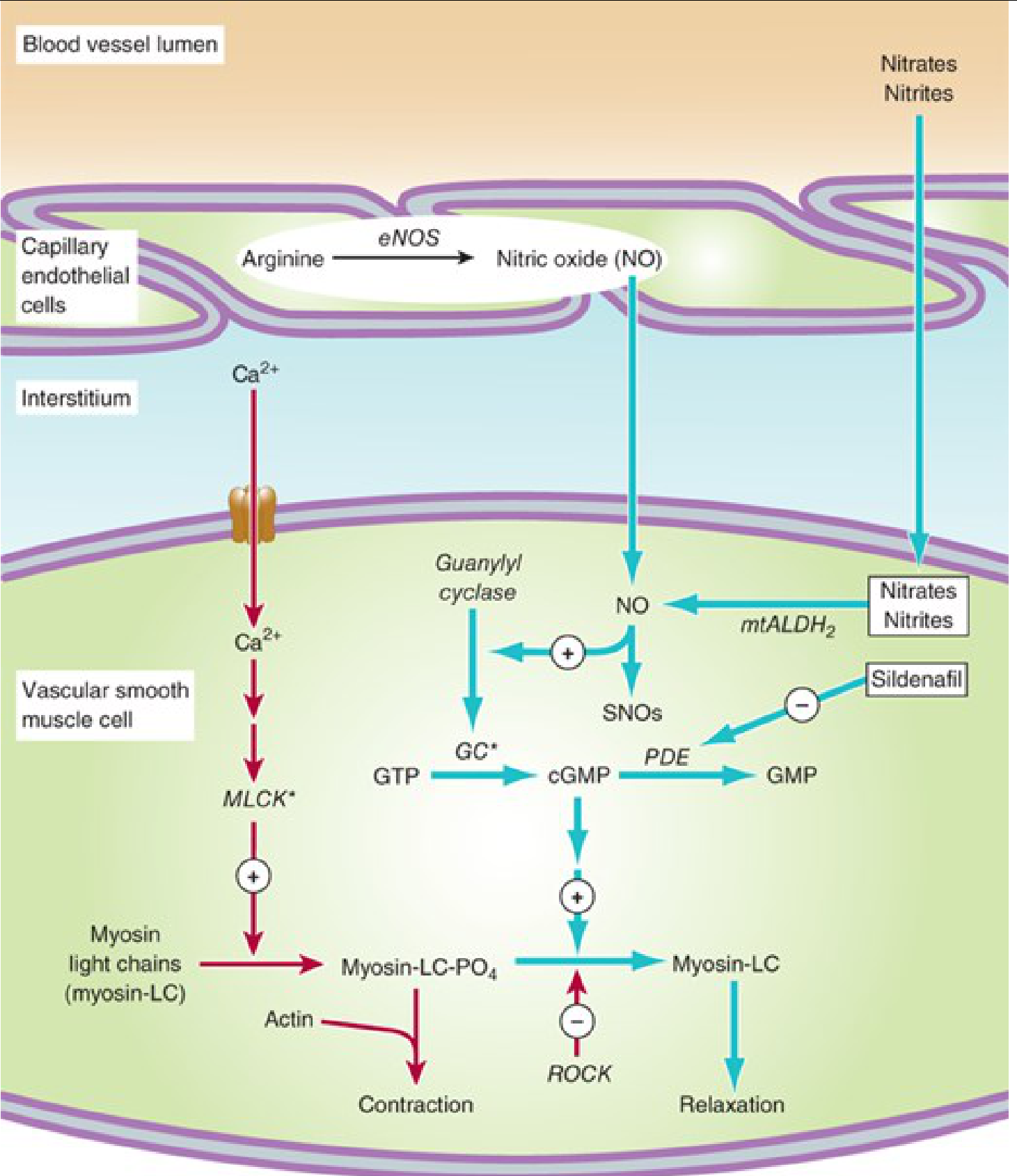
Nitrates are converted intracellularly (via mitochondrial aldehyde dehydrogenase-2, mtALDH2) to nitric oxide (NO). NO activates guanylyl cyclase → ↑ cGMP → dephosphorylation of myosin light chains → smooth muscle relaxation and vasodilation.
Hemodynamic effects:
- Venodilatation (dominant): ↓ venous return → ↓ preload → ↓ wall tension → ↓ O₂ demand
- Arteriolar dilation: ↓ afterload (at higher doses)
- Coronary artery dilation: Relieves vasospasm (variant angina); preferentially dilates epicardial coronary vessels
Pharmacokinetics & Preparations:
| Drug | Route | Onset | Duration | Use |
|---|---|---|---|---|
| Nitroglycerin (sublingual) | SL | 1–3 min | 10–30 min | Acute attack |
| Isosorbide dinitrate (SL) | SL | 5 min | 10–60 min | Acute attack |
| Nitroglycerin (IV) | IV | Minutes | Brief (stops with infusion) | Severe rest/unstable angina |
| Nitroglycerin (oral sustained) | Oral | 30 min | 6–8 h | Prophylaxis |
| Nitroglycerin (transdermal patch) | Transdermal | Slow | 8–12 h | Prophylaxis |
| Isosorbide mononitrate | Oral | — | 6–10 h | Prophylaxis (100% bioavailability) |
Note: Oral nitrates have very low bioavailability (<10–20%) due to high hepatic first-pass metabolism. Isosorbide mononitrate (active metabolite) has 100% bioavailability.
Toxicity:
- Orthostatic hypotension, reflex tachycardia
- Throbbing headache (meningeal vessel dilation)
- Tolerance: Develops with continuous exposure; prevented by providing a nitrate-free interval (8–12 h/day, usually overnight)
Key Drug Interaction: Synergistic, potentially fatal hypotension with PDE-5 inhibitors (sildenafil, tadalafil) — absolutely contraindicated combination.
2. Beta-Adrenoceptor Blockers (β-Blockers)
Prototype: Propranolol (non-selective); Atenolol, Metoprolol (β₁-selective)
Mechanism: Competitive antagonism at β-adrenoceptors → ↓ heart rate, ↓ myocardial contractility, ↓ blood pressure → reduced myocardial O₂ demand
Effects on determinants of O₂ demand:
- ↓ Heart rate (most important)
- ↓ Contractility (inotropy)
- ↓ Systolic blood pressure
Clinical Use:
- First-line prophylaxis for stable (effort) angina — shown to increase exercise time to angina/ST depression
- Protective post-MI; reduce mortality
- Not effective for variant angina (may worsen coronary spasm)
Pharmacokinetics: Oral and IV; duration varies by agent (propranolol 4–6 h; atenolol longer)
Toxicity:
- Bronchospasm (avoid in asthma — use β₁-selective agents)
- AV block, acute heart failure
- Fatigue, cold extremities
- Do not abruptly discontinue — rebound angina/tachycardia
3. Calcium Channel Blockers (CCBs)
Mechanism: Block voltage-gated L-type calcium channels on cardiac and vascular smooth muscle. Drugs bind to the α₁ subunit of the channel, reducing frequency of channel opening in response to depolarization → ↓ intracellular Ca²⁺.
Two pharmacological subgroups:
| Subgroup | Drugs | Primary Action |
|---|---|---|
| Non-dihydropyridines | Verapamil, Diltiazem | Cardiac > vascular: ↓ HR, ↓ AV conduction, ↓ contractility + vasodilation |
| Dihydropyridines | Nifedipine, Amlodipine, Felodipine | Vascular > cardiac: Potent vasodilation, less cardiac depression |
Effects on angina:
- Reduce myocardial O₂ demand (all agents)
- Dilate coronary arteries — particularly effective in variant angina (relieve spasm)
- Amlodipine/nifedipine: potent peripheral arteriolar dilation → ↓ afterload
Clinical Use:
- Stable angina: All CCBs used for prophylaxis
- Variant (Prinzmetal) angina: Drug of choice (along with nitrates)
- Verapamil/diltiazem: also used for rate control in SVT
Toxicity:
- Verapamil/diltiazem: AV block, bradycardia, acute heart failure, constipation (verapamil)
- Nifedipine/dihydropyridines: Flushing, headache, peripheral edema, reflex tachycardia (especially with immediate-release nifedipine — contraindicated in ACS)
- Amlodipine: long half-life (30–50 h), once-daily dosing, less tachycardia
4. Newer & Adjunct Antianginal Drugs
Ranolazine
- Mechanism: Inhibits the late inward Na⁺ current (late I_Na) → ↓ Na⁺-dependent Ca²⁺ overload via Na⁺/Ca²⁺ exchanger → ↓ diastolic tension and O₂ demand
- Does not affect heart rate or blood pressure significantly
- Approved in the USA for chronic stable angina refractory to other agents
- Prolongs QT interval but not associated with torsades de pointes
- Inhibits metabolism of digoxin and simvastatin
Ivabradine
- Mechanism: Selectively inhibits the hyperpolarization-activated I_f (funny) current (If/HCN channels) in the sinoatrial node → reduces heart rate without affecting contractility or blood pressure
- Efficacy similar to β-blockers and CCBs in stable angina
- Useful when β-blockers are contraindicated (e.g., asthma)
- Approved in the USA for stable symptomatic heart failure with reduced EF (also used off-label for angina)
Nicorandil
- Mechanism: Potassium channel activator + nitrate component → dual vasodilation (venous and arterial)
- Available in Europe/Asia; not approved in the USA
Trimetazidine
- Mechanism: Metabolic modulator — inhibits long-chain 3-ketoacyl thiolase (LC-3KAT), partially blocking fatty acid oxidation → shifts myocardium to more O₂-efficient glucose oxidation
- Effective in stable angina; not approved in the USA
Summary: Drug Choice by Angina Type
| Angina Type | First-Line | Alternatives |
|---|---|---|
| Stable (effort) | β-Blockers + long-acting nitrates | CCBs (all types), ranolazine, ivabradine |
| Unstable angina (ACS) | IV nitrates + heparin + antiplatelet therapy | PCI/stenting preferred; aspirin, statins |
| Variant (Prinzmetal) | CCBs (nifedipine, amlodipine) + nitrates | Avoid β-blockers |
| Stable + asthma | CCBs or long-acting nitrates | Ivabradine |
| Refractory stable | Add ranolazine | Trimetazidine (where available) |
Key Determinants of Myocardial O₂ Demand
The three drug classes reduce these determinants:
| Determinant | Nitrates | β-Blockers | CCBs |
|---|---|---|---|
| Preload (ventricular volume) | ↓↓ | ↓ | ↓ |
| Afterload (systemic BP) | ↓ | ↓ | ↓↓ (DHPs) |
| Heart rate | ↑ (reflex) | ↓↓ | ↓ (non-DHPs) |
| Contractility | ↑ (reflex) | ↓↓ | ↓ (non-DHPs) |
| Coronary spasm relief | ✓ | ✗ | ✓✓ |
Combining β-blockers with nitrates is logical: β-blockers blunt the reflex tachycardia caused by nitrates, while nitrates offset the increased preload (ventricular volume) that can result from β-blocker-induced bradycardia.
Source: Katzung's Basic and Clinical Pharmacology, 16th Edition, pp. 304–325
This is a shared conversation. Sign in to Orris to start your own chat.