Differentials of gead swelling in newborn
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Here is a comprehensive overview of the differentials for head/scalp swelling in the newborn:
Differentials of Head Swelling in the Newborn
The key differentials are birth-related extradural/scalp fluid collections, distinguished primarily by their anatomical layer, relationship to suture lines, timing, and severity.
Anatomical Overview
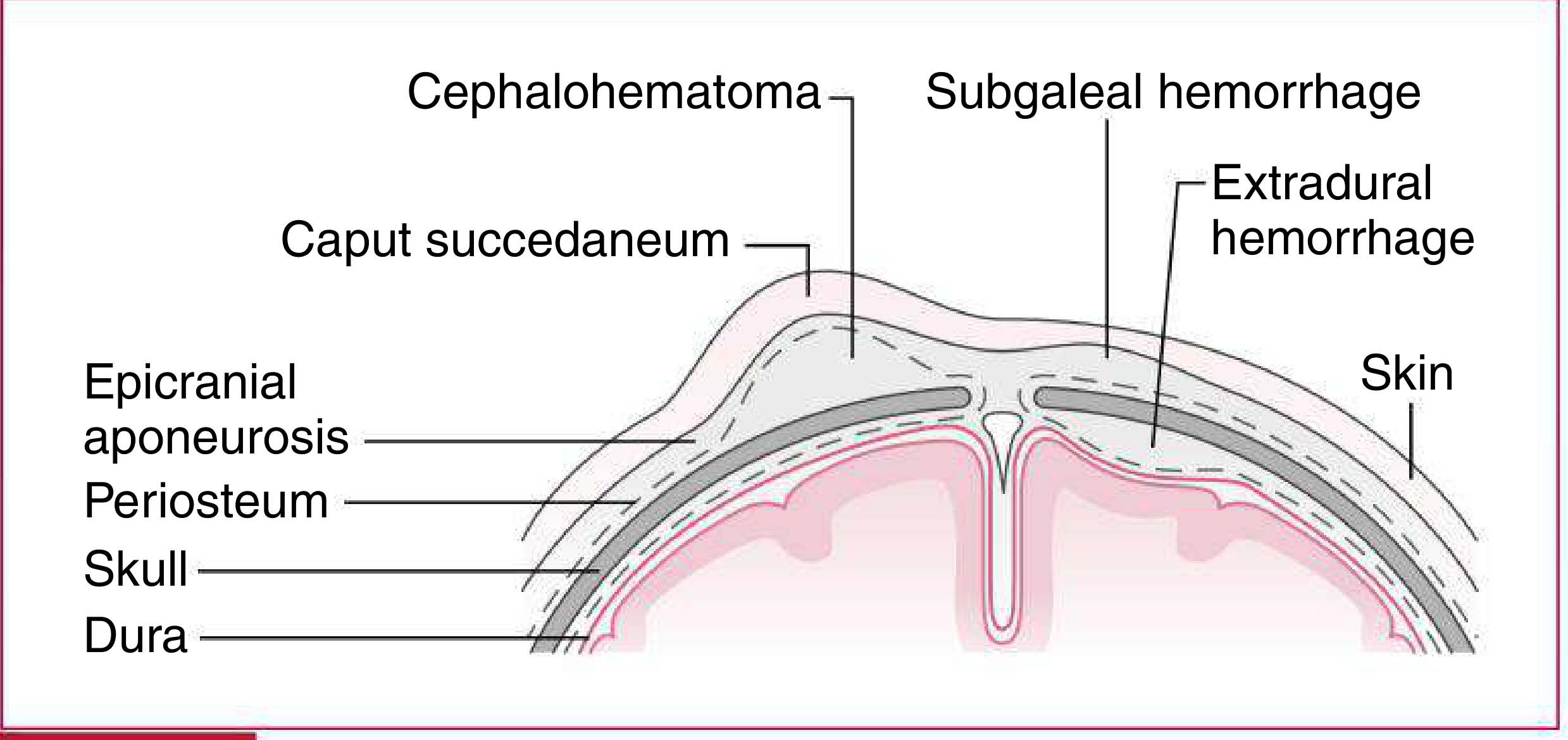
Types of extradural fluid collections in newborn infants — Harriet Lane Handbook, 23rd ed.
1. Caput Succedaneum
- Layer: Subcutaneous tissue (above epicranial aponeurosis, between skin and galea)
- Mechanism: Subcutaneous edema over the presenting part due to pressure against the cervix during delivery; common after vaginal or ventouse delivery
- Crosses suture lines: Yes — diffuse, ill-defined borders
- Consistency: Soft, pitting edema; shifts with gravity; petechiae and ecchymosis may be present
- Timing: Maximal at birth; resolves within 48–72 hours (up to 7–10 days)
- Severity: Minimal — usually benign, no treatment needed
2. Cephalohematoma
- Layer: Subperiosteal (between periosteum and skull)
- Mechanism: Rupture of diploic and/or emissary veins → subperiosteal blood collection; associated with birth trauma or vacuum-assisted delivery
- Crosses suture lines: No — well-demarcated, respects suture lines, usually unilateral (commonly over parietal bone)
- Consistency: Initially firm, becomes more fluctuant after 48 hours
- Timing: Increases after birth for 12–24 hours; resolves over weeks
- Complications: Underlying skull fracture may be present; may cause neonatal hyperbilirubinemia (from blood resorption); calcification can occur
- Severity: Rarely severe
3. Subgaleal Hemorrhage (Subaponeurotic Hemorrhage)
- Layer: Between the periosteum and the galea aponeurotica (epicranial aponeurosis) — a large potential space
- Mechanism: Damage to emissary veins; associated with birth trauma, often vacuum extraction
- Crosses suture lines: Yes — can extend from orbital ridges to nape of neck
- Consistency: Firm to fluctuant, ill-defined borders; may have crepitus or fluid waves
- Timing: Progressive increase after birth; resolution over weeks
- Severity: Potentially life-threatening — massive blood loss can cause hypovolemic shock or DIC; particularly dangerous in the setting of coagulopathy (e.g., vitamin K deficiency, hemophilia)
Comparison Table (Birth-Related Extradural Collections)
| Feature | Caput Succedaneum | Cephalohematoma | Subgaleal Hemorrhage |
|---|---|---|---|
| Layer | Above galea (subcutaneous) | Subperiosteal | Below galea, above periosteum |
| Crosses sutures | Yes | No | Yes |
| Borders | Vague, pitting | Distinct, firm→fluctuant | Ill-defined, fluid wave |
| Timing | Present at birth; resolves 48–72 hr | Grows 12–24 hr; resolves weeks | Progressive; resolves weeks |
| Severity | Minimal | Rarely severe | Potentially life-threatening |
4. Extradural (Epidural) Hemorrhage
- Located between the skull and the dura
- Usually traumatic (e.g., forceps delivery, skull fracture)
- Less common in neonates; presents with bulging fontanelle, neurological deterioration
5. Other Causes to Consider
- Encephalocele: Herniation of brain tissue through a skull defect — midline swelling, present at birth, transilluminates, pulsatile
- Aplasia cutis congenita: Congenital absence of skin/scalp, often midline or vertex — not a hematoma but can be mistaken for a scalp lesion
- Scalp abscess / cellulitis: Follows fetal scalp electrode placement; warm, tender, fluctuant, with signs of infection
- Skull fracture with soft tissue swelling: May accompany cephalohematoma or birth trauma
- Meningocele/Myelomeningocele: If swelling is over posterior midline
Key Clinical Pearl
The most dangerous is subgaleal hemorrhage — it can accommodate the entire neonatal blood volume (≈250 mL) within the subaponeurotic space. Any newborn (especially after vacuum extraction) with a progressively enlarging, "boggy" scalp swelling crossing suture lines must be monitored urgently for coagulopathy and hemodynamic compromise.
Sources: Fitzpatrick's Dermatology, Vol. 1 | Harriet Lane Handbook, 23rd ed. | Bradley & Daroff's Neurology in Clinical Practice | Grainger & Allison's Diagnostic Radiology
CAN score
Reading File
Finding Sources
Finding Sources
Finding Sources
Asking for Preferences
This is a shared conversation. Sign in to Orris to start your own chat.