Ift vs tens machine choice in physiotherapy
IFT vs TENS — Choosing in Physiotherapy
1. Basic Principles
| Feature | TENS | IFT |
|---|---|---|
| Current type | Low-voltage monophasic or biphasic pulsed | Two medium-frequency AC currents (typically 4000 Hz & 4001–4250 Hz) that interfere to produce a low-frequency beat |
| Effective frequency | 1–150 Hz (directly applied) | Beat frequency 1–150 Hz produced deep in tissue |
| Electrode setup | 2–4 surface electrodes | 4 electrodes (2 circuits cross at the target tissue) |
| Depth of penetration | Superficial (skin & subcutaneous) | Deeper tissues (muscle, joints, deeper nerves) |
| Skin impedance | High — limits deep penetration | Overcome by medium-frequency carrier; low skin resistance |
2. Mechanism of Analgesia
- Gate control theory — high-frequency TENS (>80 Hz) activates large-diameter Aβ fibres, inhibiting nociceptive transmission in the dorsal horn via interneurons in the substantia gelatinosa
- Endorphin release — low-frequency TENS (<10 Hz) stimulates Aδ fibres and promotes endogenous opioid (enkephalin/β-endorphin) release
- Possible direct local vasodilation reducing ischaemic pain
- The same gate control and endorphin mechanisms, but the interference beat frequency is generated within deep tissue, so it reaches structures that TENS cannot penetrate effectively
- Less skin irritation because the carrier frequency (4000 Hz) has low impedance through skin; the therapeutic low-frequency effect is produced internally
- Additionally has a muscle pumping effect at certain frequencies (~10–50 Hz), promoting blood flow and oedema reduction
3. Parameter Comparison
| Parameter | TENS | IFT |
|---|---|---|
| Carrier frequency | 1–150 Hz directly | 4000 Hz (one circuit), 4001–4250 Hz (other) |
| Beat/therapeutic frequency | Same as applied | 1–250 Hz (adjustable) |
| Pulse width | 50–200 µs (affects fibre type activated) | Determined by beat frequency |
| Modes | Conventional, acupuncture-like, burst, modulation | Constant, sweep (AMF), rhythmic |
| Session duration | 20–30 min | 15–20 min |
4. Indications — When to Choose Which
Choose TENS when:
- Superficial/localised pain — skin wounds, superficial soft tissue injuries, post-herpetic neuralgia
- Chronic musculoskeletal pain — back pain, osteoarthritis (mild), myalgia
- Neuropathic pain — phantom limb, peripheral neuropathy
- Postoperative pain — early mobilisation, incision site pain
- Obstetric pain (after first trimester) — especially low back pain in labour
- Home use — TENS is portable, inexpensive, self-administered; ideal for ongoing chronic pain management
- Neuralgias — herpes zoster, trigeminal neuralgia (electrode placement around but not over the area)
Choose IFT when:
- Deep tissue pain — hip joint, knee joint, shoulder joint pathology; deep muscle spasm
- Acute oedema & post-traumatic swelling — IFT's muscle pumping at 10–50 Hz helps lymphatic drainage
- Periarticular conditions — bursitis, capsulitis, periarthritis
- Deep nerve pain — sciatic nerve involvement, deep lumbar pain
- Muscle re-education / stimulation of deep muscles where surface TENS cannot reach
- Circulatory insufficiency — IFT promotes vasodilation of deep vessels
- Chronic pelvic pain, stress urinary incontinence — IFT reaches pelvic floor muscles effectively
5. Contraindications
| Contraindication | TENS | IFT |
|---|---|---|
| Demand pacemaker | ✗ Avoid | ✗ Avoid |
| First-trimester pregnancy | ✗ Avoid | ✗ Avoid |
| Over active malignancy | ✗ Avoid | ✗ Avoid |
| Cardiac dysrhythmias | ✗ Avoid | ✗ Avoid |
| Undiagnosed pain | ✗ Avoid | ✗ Avoid |
| Over infected/damaged skin | ✗ | ✗ |
| Over carotid sinus/anterior neck | ✗ | ✗ |
| Thrombosis / DVT | — | ✗ (muscle pump effect could dislodge clot) |
| Metal implants at site | Caution | Greater caution (stronger current concentration) |
6. Practical Decision Guide
Is the target tissue deep (joint, deep muscle, sciatic nerve)?
YES → IFT preferred
NO (superficial / skin / subcutaneous)?
→ TENS preferred
Is oedema / swelling the primary concern?
YES → IFT (muscle pump frequency 10–50 Hz)
Is the patient managing pain at home long-term?
YES → TENS (portable, affordable, self-use)
Is it a neuropathic / post-herpetic pain?
YES → TENS (especially high-frequency conventional)
Is it acute joint pain / peri-articular inflammation?
YES → IFT
7. Quick Summary
| TENS | IFT | |
|---|---|---|
| Best for | Superficial, neuropathic, chronic pain; home use | Deep tissue, joint, oedema, pelvic floor |
| Depth | Superficial | Deep |
| Portability | High (handheld units) | Low (clinic-based) |
| Skin comfort | May cause irritation with prolonged use | Better tolerated (medium-frequency carrier) |
| Evidence base | Strong for chronic back pain, neuropathic pain | Moderate; good for knee OA, post-trauma swelling |
| Cost | Low | Higher (clinic equipment) |
Sudden hamstring or calf cramp at night everyday or sometime or Charley horse syndrome
Sudden hamstring or calf cramp at night everyday or sometime or Charley horse syndrome
Nocturnal Leg Cramps (Charley Horse)
What Actually Happens (Mechanism)
"Any local irritating factor or metabolic abnormality of a muscle — such as severe cold, lack of blood flow, or overexercise — can elicit pain or other sensory signals transmitted from the muscle to the spinal cord, which in turn cause reflex feedback muscle contraction. The contraction stimulates the same sensory receptors even more, which causes the spinal cord to increase the intensity of contraction. Thus, positive feedback develops, so a small amount of initial irritation causes more and more contraction until a full-blown muscle cramp ensues." — Guyton and Hall Textbook of Medical Physiology
Common Causes & Triggers
Physiological (Most Common)
| Cause | Why It Causes Cramps |
|---|---|
| Dehydration | Reduced plasma volume → poor muscle perfusion + electrolyte concentration |
| Electrolyte imbalance | Low Mg²⁺, K⁺, Ca²⁺, Na⁺ → increased motor neuron excitability |
| Prolonged standing or sitting | Sustained posture shortens calf muscles |
| Overexertion / unaccustomed exercise | Metabolic byproduct accumulation; muscle fatigue |
| Sleep posture (feet plantar-flexed, sheets pressing down) | Shortened calf in a vulnerable position |
| Pregnancy (especially 3rd trimester) | Electrolyte shifts, increased lower-limb venous pressure |
| Older age | Reduced motor neuron number, loss of muscle bulk, poorer circulation |
Medical Conditions to Rule Out
| Condition | Mechanism |
|---|---|
| Peripheral vascular disease / arterial insufficiency | Ischaemia → cramp (classic "charley horse" in DVT calf — Harrison's/Rosen's) |
| Deep vein thrombosis (DVT) | Persistent calf cramp that worsens over days — a red flag |
| Hypothyroidism | Muscle cramp is a recognized symptom (slowed ATP turnover) |
| Hypocalcaemia | Low Ca²⁺ → increased neuromuscular irritability, cramps, tetany |
| Hypomagnesaemia | Mg²⁺ is a natural NMDA antagonist; low levels lower seizure/cramp threshold |
| Hypokalaemia | Diuretic use, vomiting, diarrhoea |
| Chronic kidney disease | Uraemia + electrolyte dysregulation |
| Diabetes mellitus | Peripheral neuropathy alters motor neuron thresholds |
| Liver cirrhosis | Electrolyte imbalance, poor nutrition |
| Neurological disease | ALS, Parkinson's, radiculopathy (L5/S1 → calf; L5 → hamstring) |
Drug-Induced Cramps
- Diuretics (furosemide, thiazides) — potassium/magnesium loss
- Statins — myopathy-related
- Beta-agonists (salbutamol)
- Raloxifene, clonazepam, lithium
- Alcohol (chronic use)
Red Flags — When to Seek Medical Evaluation
- Unilateral calf cramp that persists and worsens over days → suspect DVT
- Associated with leg swelling, redness, or warmth
- Occurring with leg pain on walking (cramping that relieves with rest) → suspect peripheral arterial disease / claudication
- In a pregnant woman — may indicate electrolyte emergency
- Accompanied by muscle weakness, wasting, or fasciculations → possible neurological cause (ALS, radiculopathy)
- Not responding to any conservative measures
Immediate Relief (During a Cramp)
- Stretch the muscle — straighten the knee and dorsiflex the foot (pull toes toward the shin). This breaks the positive feedback loop by activating the Golgi tendon organ, triggering autogenic inhibition.
- Stand up and bear weight on the affected leg — immediate reflex inhibition of the cramp.
- Massage the muscle belly firmly in the direction of the fibres.
- Apply warmth (warm towel/heat pack) — reduces muscle spindle sensitivity.
- For hamstring cramps: lie flat, extend the knee, and flex the hip with the leg straight.
Prevention & Long-Term Management
Lifestyle & Physical
| Measure | Evidence |
|---|---|
| Stretching before bed — calf stretches (wall stretch, towel stretch) | Good evidence; reduces frequency |
| Adequate hydration throughout the day | Practical; especially important in athletes/elderly |
| Regular moderate exercise (walking, swimming) | Improves circulation and muscle conditioning |
| Avoid tucked-in tight sheets at night (keep feet free to dorsiflex) | Reduces passive plantar flexion trigger |
| Correct footwear — avoid flat/unsupported shoes all day | Reduces calf fatigue |
| Avoid prolonged sitting with legs crossed or dangling |
Nutritional Supplementation
| Supplement | Dose / Notes |
|---|---|
| Magnesium | 300–400 mg/day (glycinate or citrate form best absorbed) — good evidence, especially in pregnancy |
| Potassium | Via diet (bananas, oranges, sweet potato) or supplement if deficient |
| Calcium | Important if hypocalcaemic or in elderly |
| Vitamin D | Supports Ca²⁺ absorption and muscle function |
| Electrolyte drinks | Useful in athletes or high-sweat situations |
Pharmacological (Doctor-prescribed)
| Drug | Notes |
|---|---|
| Quinine sulfate | Historically the most effective; now restricted in many countries due to cardiac arrhythmia risk (QT prolongation). Only if cramps are severe and unresponsive to other measures. |
| Magnesium supplementation | Safest first-line pharmacological option |
| Diltiazem (calcium channel blocker) | Some evidence in refractory cases |
| Gabapentin / pregabalin | Used when neuropathic component suspected |
| Verapamil | Second-line option |
| Vitamin B complex | Some supporting evidence, particularly B1 (thiamine) |
Physiotherapy Role
- Stretching programme — daily calf, hamstring, and plantar fascia stretching
- IFT or TENS — for muscle pain relief post-cramp
- Hydrotherapy — warm water exercise reduces muscle excitability
- Gait and posture assessment — flat feet (pes planus) or leg length discrepancy can overload the calf/hamstring chronically
- Dry needling to trigger points in gastrocnemius/soleus if chronic tightness is a contributing factor
- Manual therapy to lumbar spine if L4/L5/S1 radiculopathy is suspected as the underlying driver
Summary Table
| Feature | Detail |
|---|---|
| Most common site | Gastrocnemius (calf), also hamstring |
| Peak time | 2–4 AM (deepest sleep, most relaxed muscles) |
| Duration of episode | Seconds to 10 minutes; soreness may last hours–days |
| Most common cause | Dehydration + electrolyte imbalance + posture |
| First-line treatment | Stretch + dorsiflex immediately; hydration; Mg supplementation |
| Dangerous mimic | DVT (worsening unilateral calf pain — investigate urgently) |
| Best prevention | Nightly stretching + adequate hydration + magnesium |
Person having pain in one side of his body continues after having hamramegaic stroke of 9 months also history of RA and gout muscle power is good but still pain one only affected side of body
Unilateral Pain After Haemorrhagic Stroke — Clinical Analysis
1. Primary Diagnosis: Central Post-Stroke Pain (CPSP)
What It Is
"Lesions at any level of the neuroaxis (generally affecting spinothalamocortical afferent sensory pathways) including the medulla, pons, midbrain, thalamus, subcortical white matter, and the cortex may produce central poststroke pain syndrome. The thalamus and brainstem are common sites; 8–16% of thalamic strokes may lead to chronic pain." — Bradley and Daroff's Neurology in Clinical Practice
"The severe, persistent, unrelenting unilateral pain often is described in dramatic terms... With partial recovery of sensation or with an acute but incomplete lesion, spontaneous pain or discomfort (Dejerine-Roussy syndrome), sometimes of the most distressing type, may appear on the affected side." — Adams and Victor's Principles of Neurology, 12th Ed.
Why It Fits This Patient
| Feature | Explanation |
|---|---|
| Pain only on affected side | Damage to contralateral thalamus/VPL nucleus or parietal white matter produces unilateral hemibody pain |
| 9 months post-stroke | CPSP typically develops weeks to months after stroke — a delay is characteristic |
| Good muscle power | CPSP is a pure sensory/pain phenomenon; motor pathways can be intact |
| Haemorrhagic stroke | More tissue destruction than ischaemic stroke → greater likelihood of sensory pathway disruption |
Characteristics of CPSP
- Burning, aching, shooting, or squeezing pain — constant or paroxysmal
- Allodynia — normally non-painful stimuli (light touch, clothing) cause pain
- Hyperalgesia — exaggerated pain response to stimuli
- Hyperpathia — delayed, explosive pain after stimulation
- Thermal allodynia — cold especially triggers or worsens pain
- Emotional disturbance, noise, or even music can aggravate it
"Thermal — especially cold — stimuli, emotional disturbance, loud sounds, and even certain types of music may aggravate the painful state." — Adams and Victor's Principles of Neurology
2. Compounding Causes (RA + Gout on Affected Side)
Rheumatoid Arthritis (RA)
- RA causes synovial inflammation, joint destruction, and peripheral sensitisation
- On the stroke-affected side, reduced activity and immobilisation worsens RA joint involvement (disuse synovitis, contractures)
- The patient may have shoulder, hand, or knee joint pain from RA that blends with CPSP
- RA flares in immobilised joints → adhesive capsulitis (frozen shoulder) is very common post-stroke
Gout
- Gout attacks (acute crystal arthropathy) cause exquisite joint pain — most commonly in foot, ankle, knee
- On the affected side, reduced mobility → poor urate clearance from joints → more frequent gout attacks
- Gout pain is episodic, sudden, nocturnal, severe — may be misinterpreted as worsening CPSP
- Dehydration (common in stroke patients) and diuretic use raise serum urate
Hemiplegic Shoulder Pain (Separate Entity)
"Some 40–60% of patients develop shoulder pain after a stroke. It is postulated that the pain is due to inflammation in the joint secondary to immobilisation and joint contracture (frozen shoulder syndrome)." — Bradley and Daroff's Neurology in Clinical Practice
3. Full Differential Diagnosis
| Diagnosis | Likelihood | Key Feature |
|---|---|---|
| Central Post-Stroke Pain (CPSP / Dejerine-Roussy) | High | Burning, allodynia, whole hemibody, 9 months post-stroke |
| Hemiplegic shoulder pain | High | Shoulder subluxation + capsulitis post-stroke |
| RA flare (affected side joints) | Moderate | Joint swelling, morning stiffness, symmetrical |
| Gout attack | Moderate | Sudden, episodic, nocturnal, periarticular |
| Spasticity-related pain | Moderate | Muscle tightness, painful spasms (even with good power, spasticity may be present) |
| Complex Regional Pain Syndrome (CRPS) type 1 | Low-moderate | Autonomic changes, allodynia, disuse of limb |
| DVT | Rule out | Calf pain, swelling, immobility risk factor |
| Peripheral nerve compression | Low | Prolonged positioning post-stroke |
4. Assessment Approach
History
- Character of pain: burning/shooting/aching? Constant or paroxysmal?
- Does light touch or cold worsen it? (→ CPSP allodynia)
- Is pain episodic and joint-specific? (→ Gout)
- Morning stiffness >30 min, symmetric joints? (→ RA)
- Shoulder pain with overhead movement? (→ Hemiplegic shoulder)
Examination
- Sensory testing: pinprick, light touch, temperature, vibration on affected vs. unaffected side
- Check for allodynia (cotton wool → pain on affected side = CPSP)
- Joint examination: swelling, tenderness, range of motion
- Shoulder: assess for subluxation (fingerbreadth gap below acromion)
- Look for tophaceous deposits (gout)
Investigations
| Test | Purpose |
|---|---|
| MRI brain (review old/new) | Confirm stroke location — thalamic/parietal involvement supports CPSP |
| Serum uric acid | Gout |
| Synovial fluid aspiration (if joint swollen) | MSU crystals = gout; inflammatory = RA |
| RF, anti-CCP, ESR, CRP | RA activity |
| Doppler ultrasound leg | Exclude DVT |
| X-ray shoulder | Subluxation, joint space reduction |
5. Management
A. Central Post-Stroke Pain (CPSP)
"Dysesthesias, when severe and persistent, may respond to anticonvulsants (carbamazepine 100–1000 mg/d; gabapentin 300–3600 mg/d; or pregabalin 50–300 mg/d), antidepressants (amitriptyline 25–150 mg/d; nortriptyline 25–150 mg/d; desipramine 100–300 mg/d; or venlafaxine 75–225 mg/d)." — Harrison's Principles of Internal Medicine, 22nd Ed.
| Drug | Dose | Notes |
|---|---|---|
| Amitriptyline | 25–75 mg nocte | Best evidence for CPSP; also helps sleep |
| Gabapentin | 300–3600 mg/day in divided doses | Titrate slowly |
| Pregabalin | 50–300 mg/day | Better tolerated than gabapentin |
| Lamotrigine | 25–200 mg/day | Open-label evidence for CPSP |
| Duloxetine / venlafaxine | Standard doses | SNRI option |
- Motor cortex stimulation (MCS) — neurosurgical; evidence for refractory CPSP
- Deep brain stimulation (DBS)
- Ketamine infusion — short-term pain relief
- TENS / IFT — adjunct; modest benefit for peripheral component
B. Hemiplegic Shoulder Pain
- Proper positioning and arm support (sling when mobilising)
- Range-of-motion physiotherapy — passive then active-assisted
- Suprascapular nerve block — for refractory shoulder pain
- Intra-articular corticosteroid — if adhesive capsulitis
- Avoid aggressive passive stretch (can worsen subluxation)
C. Gout (on Affected Side)
- Colchicine (0.5 mg BD) or NSAIDs for acute attacks (caution: renal function post-stroke)
- Allopurinol for prophylaxis (start once acute attack settles; target uric acid <360 µmol/L)
- Adequate hydration
- Dietary: reduce purines (red meat, organ meat, alcohol — especially beer)
- Note: NSAIDs should be used cautiously in post-stroke patients (cardiovascular and renal risk)
D. RA Management
- Continue/optimise DMARDs (methotrexate, hydroxychloroquine, leflunomide)
- Physiotherapy — joint protection, splinting, range of motion
- Short-course corticosteroids for acute flares on affected side
- Avoid long-term NSAIDs post-haemorrhagic stroke
E. Physiotherapy (Overall)
| Modality | Role |
|---|---|
| Graded motor imagery / mirror therapy | Recalibrates cortical pain maps in CPSP |
| Desensitisation programme | Gradually reduces allodynia through graded touch |
| IFT / TENS | Peripheral pain modulation |
| Heat therapy | Muscle relaxation, joint stiffness |
| Occupational therapy | ADL adaptation, splinting |
| Hydrotherapy | Joint offloading, pain-free movement |
Summary
Post-haemorrhagic stroke unilateral pain at 9 months
+ Good motor power
+ Allodynia / burning quality
→ PRIMARY = Central Post-Stroke Pain (CPSP / Dejerine-Roussy)
Co-existing RA → adds joint inflammation and immobility pain
Co-existing Gout → adds episodic crystal arthropathy attacks
Immobility → adds hemiplegic shoulder pain (40–60% of stroke patients)
Management is MULTIMODAL:
Amitriptyline or Gabapentin/Pregabalin (CPSP)
+ Physiotherapy (desensitisation, ROM, positioning)
+ Optimised RA DMARD therapy
+ Allopurinol + Colchicine (Gout)
+ Shoulder protection and nerve block if needed
Hammoroids and role of physiotherapy in
Haemorrhoids & the Role of Physiotherapy
1. What Are Haemorrhoids?
"Hemorrhoids are normal vascular structures in the submucosal layer of the anal canal, arising from a channel of arteriovenous connective tissues that drains into the superior and inferior hemorrhoidal veins." — Roberts and Hedges' Clinical Procedures in Emergency Medicine
2. Classification
| Grade/Type | Description |
|---|---|
| Internal Grade I | Bulge into canal, no prolapse, painless bleeding |
| Internal Grade II | Prolapse on straining, spontaneously reduce |
| Internal Grade III | Prolapse on straining, require manual reduction |
| Internal Grade IV | Permanently prolapsed, cannot be reduced |
| External | Below dentate line, covered by skin (anoderm), very painful, somatic innervation |
| Mixed | Both internal and external components |
3. Symptoms
- Bright red rectal bleeding (on tissue or in bowl — not mixed with stool)
- Prolapse felt as a lump at the anus
- Perianal itching / discomfort (mucus discharge)
- Aching or heaviness after defecation
- Acute severe pain — thrombosed external haemorrhoid
- Anaemia in chronic bleeders
4. Causes & Contributing Factors
| Factor | Mechanism |
|---|---|
| Chronic constipation / straining | Raised intra-abdominal and venous pressure |
| Low-fibre diet | Hard stools → prolonged straining |
| Prolonged sitting (desk job, toilet reading) | Sustained perineal pressure |
| Obesity | Raised intra-abdominal pressure |
| Pregnancy | Venous compression by uterus + hormonal laxity of connective tissue |
| Pelvic floor dysfunction | Weak or hypertonic pelvic floor increases bearing-down forces |
| Sedentary lifestyle | Reduced venous return from lower body |
| Heavy lifting / chronic cough | Valsalva-like pressure surges |
5. Medical & Surgical Management (Context for Physiotherapy)
Conservative (First-line)
- High-fibre diet (25–35 g/day) + increased water (8–10 glasses/day) — most important intervention
- Bulk-forming laxatives (psyllium/ispaghula husk)
- Sitz baths — warm water soaks 15–20 min, 2–3×/day; reduces spasm, oedema, pain
- Topical agents — corticosteroid/anaesthetic creams (short term only)
- Stool softeners (docusate sodium)
Office Procedures
- Rubber band ligation — best evidence for Grade II–III internal haemorrhoids
- Infrared photocoagulation (IRC)
- Sclerotherapy
Surgical
- Haemorrhoidectomy — Grade III–IV, mixed, failed office procedures
- Stapled haemorrhoidopexy
6. Role of Physiotherapy
A. Pelvic Floor Rehabilitation
Pelvic Floor Strengthening (Kegel Exercises)
- Strengthens the levator ani, pubococcygeus, and external anal sphincter
- Improves venous return from the anorectal vasculature
- Reduces passive engorgement of haemorrhoidal cushions
- Reduces faecal incontinence associated with prolapsed haemorrhoids
- Technique: Contract pelvic floor as if stopping urine midstream → hold 5–10 seconds → relax fully → repeat 10–15 times, 3 sets/day
Pelvic Floor Relaxation / Downtraining
- Many patients with haemorrhoids have a paradoxically contracting or hypertonic pelvic floor — they strain against a tight sphincter, massively increasing rectal pressure
- Biofeedback-assisted relaxation teaches the patient to relax the puborectalis and external anal sphincter during defecation
- Evidence supports biofeedback for dyssynergic defecation (outlet obstruction constipation) — a major cause of haemorrhoid worsening
Biofeedback Therapy
- Surface EMG or manometry probes provide real-time feedback of sphincter and pelvic floor activity
- Teaches proper coordination — relax floor while bearing down gently
- Reduces straining force and time spent on the toilet
- Also used post-haemorrhoidectomy to restore continence
B. Posture and Defecation Mechanics
- Physiotherapists educate on optimal defecation posture
- The squatting position (knees higher than hips — use a footstool/squatty potty) straightens the anorectal angle, reduces straining effort by ~30%, and reduces time to defecation
- Correcting breath-holding and Valsalva straining — teach diaphragmatic breathing with gentle exhale during defecation instead of breath-holding
C. Electrotherapy Modalities
| Modality | Application |
|---|---|
| Interferential Therapy (IFT) | Applied perianally/lower abdomen; reduces oedema, improves local circulation, pain relief |
| TENS | Perianal electrode placement for post-haemorrhoidectomy pain and sphincter spasm |
| Ultrasound therapy | Thermal and non-thermal effects — reduces perianal oedema and promotes healing post-procedure |
| Infrared / Low-level laser therapy | Wound healing post-haemorrhoidectomy, reduces pain and inflammation |
| High-voltage galvanic stimulation | Used in some centres for anal sphincter re-education |
D. Manual Therapy / Soft Tissue Techniques
- Myofascial release of hypertonic pelvic floor muscles (internal and external techniques)
- Trigger point therapy to levator ani, obturator internus, piriformis — reduces referred perineal pain
- Scar tissue mobilisation post-haemorrhoidectomy — prevents fibrotic stricture and painful scarring
- Perineal massage — improves tissue extensibility and reduces postoperative discomfort
E. Post-Haemorrhoidectomy Rehabilitation
| Goal | Intervention |
|---|---|
| Pain management | TENS, sitz baths, positioning advice |
| Prevent constipation | Dietary advice, defecation technique retraining |
| Restore sphincter function | Pelvic floor exercises, biofeedback |
| Reduce oedema | IFT, elevation, sitz baths |
| Scar management | Manual therapy, ultrasound |
| Early mobilisation | Walking programme to improve venous return |
F. Lifestyle and Exercise Prescription
- Aerobic exercise (walking, swimming, cycling) improves bowel motility, reduces constipation, and promotes venous return from the lower body
- Avoid prolonged sitting — advise regular standing/walking breaks
- Core strengthening — reduces intra-abdominal pressure fluctuations during daily activities
- Avoid heavy straining exercise (heavy deadlifts, intense Valsalva exercises) during acute flares
- Weight management — obesity directly increases haemorrhoidal pressure
G. Patient Education (Key Physiotherapy Role)
| Topic | Key Message |
|---|---|
| Fibre and hydration | 25–35 g fibre/day; 2–2.5 L water/day |
| Toilet behaviour | No more than 3–5 minutes on the toilet; no phone/reading |
| Defecation posture | Footstool to raise knees above hips |
| Avoid straining | Let gravity and pelvic relaxation do the work |
| Exercise | Daily walking 20–30 min minimum |
| Recognise red flags | Blood mixed in stool (not on surface), unexplained weight loss, change in bowel habit → refer for colonoscopy |
7. Summary Table
| Role of Physiotherapy | Specific Techniques |
|---|---|
| Pelvic floor rehabilitation | Kegel exercises, downtraining, biofeedback |
| Defecation retraining | Posture, breath control, timing |
| Pain relief | TENS, IFT, ultrasound, sitz baths |
| Post-surgical rehab | Scar management, sphincter re-education, oedema control |
| Lifestyle modification | Exercise prescription, weight management, dietary education |
| Prevent recurrence | Bowel habit regulation, core stability, avoiding prolonged sitting |
Disc bulge, prolapse, protrusion and role mcqenzie and extension exercises
lumbar disc herniation protrusion extrusion sequestration types diagram
McKenzie extension exercise lumbar spine prone press up back pain
Disc Bulge, Prolapse, Protrusion & the McKenzie / Extension Exercise Approach
Part 1: Disc Pathology — Classification & Terminology
Anatomy of the Intervertebral Disc
- Nucleus pulposus — central gel-like core, high water content, absorbs axial load
- Annulus fibrosus — concentric collagen rings encasing the nucleus; resists radial and tensile forces
- Cartilaginous end plates — anchor the disc to vertebral bodies
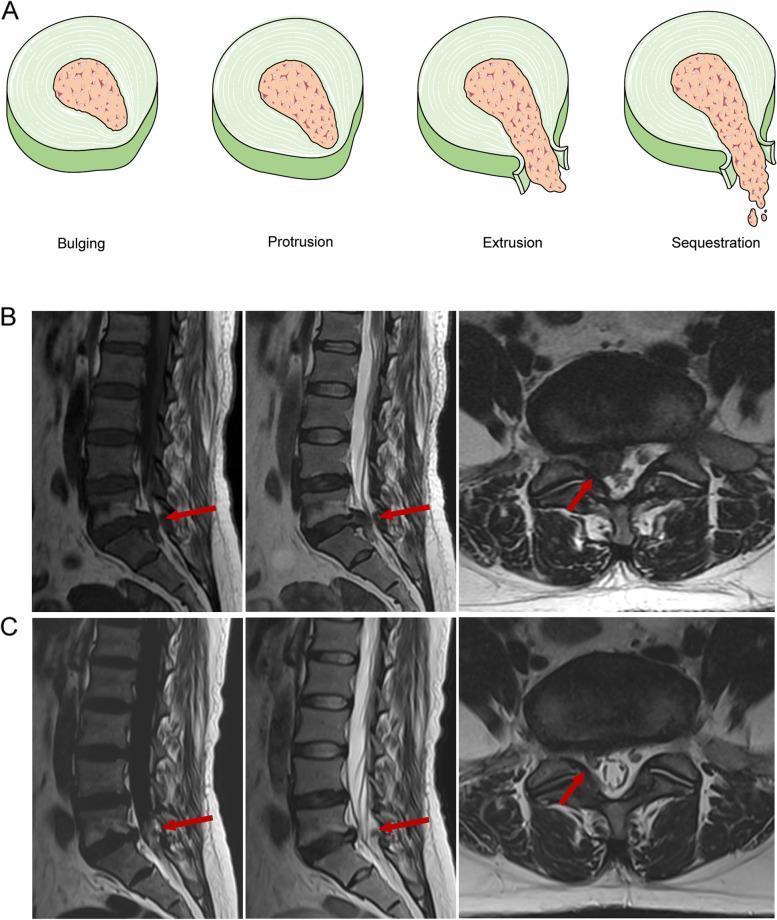
Disc Pathology Classification (Combined Task Forces / Radiological Standard)
"A 'disc protrusion' is used when the base of the disc is broader than any other diameter of the displaced disc material. It is called an 'extruded disc' when the base against the disc is smaller than the diameter of the displaced disc material." — Grainger & Allison's Diagnostic Radiology
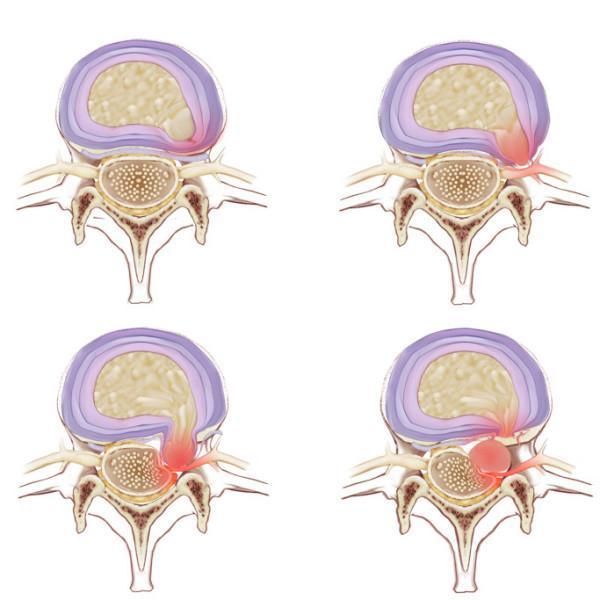
| Stage | Description | Annulus Status | Clinical Significance |
|---|---|---|---|
| Disc Bulge | Generalised, symmetric extension of disc margin >2 mm beyond endplate over >180° | Annulus intact, stretched | Often asymptomatic; associated with degeneration |
| Disc Protrusion | Focal herniation; base (neck) wider than apex; nucleus pushes against but is contained by annulus | Annulus intact (inner layers may tear) | Pain, possible nerve irritation; good prognosis conservatively |
| Disc Extrusion / Prolapse | Nucleus breaks through annulus; base narrower than apex ("toothpaste sign"); material in epidural space | Annulus torn through | Radiculopathy likely; more severe but often resorbs spontaneously |
| Sequestration / Free Fragment | Extruded material completely detached from parent disc, migrates up/down canal | Full annular rupture | Most severe; risk of cauda equina; paradoxically may resorb fastest |
| Subannular extrusion | Nucleus migrates within annular layers, outermost intact | Partial breach | Intermediate severity |
"An extrusion is seldom seen in asymptomatic patients... Disc material exposed to the epidural space appears to resolve more quickly than subligamentous disc herniations." — Grainger & Allison's Diagnostic Radiology
Location Classification (Axial/Transverse Plane)
| Zone | Effect |
|---|---|
| Central | Compresses thecal sac; bilateral symptoms; cauda equina risk if large |
| Paracentral (posterolateral) | Most common; compresses descending nerve root (e.g., L4–5 disc → L5 root) |
| Foraminal | Compresses exiting root (e.g., L4–5 disc → L4 root) |
| Extraforaminal (far lateral) | Rare; compresses exiting root outside canal |
Common Levels & Nerve Root Signs
| Level | Root Compressed | Pain Distribution | Motor Loss | Reflex |
|---|---|---|---|---|
| L3–L4 | L4 | Anterior thigh → medial leg | Knee extension | Knee jerk ↓ |
| L4–L5 | L5 | Posterior thigh → lateral leg → dorsum of foot | Foot/great toe dorsiflexion (EHL) | None (or tibialis posterior) |
| L5–S1 | S1 | Posterior thigh → calf → lateral foot | Plantarflexion, toe flexion | Ankle jerk ↓ |
Natural History
"Disc herniation occurs when the annulus fibrosis thins and tears, and the nucleus pulposus prolapses, usually laterally, compressing and inflaming a nerve root. Clinical symptoms are typically self-limited, with a high rate of spontaneous improvement... The size of the disc protrusion may naturally decrease over time." — Rosen's Emergency Medicine
Part 2: McKenzie Method (MDT — Mechanical Diagnosis and Therapy)
Who Developed It?
Three McKenzie Syndromes
| Syndrome | Description | Key Feature | Treatment Direction |
|---|---|---|---|
| Derangement Syndrome | Disc material displaced within/through annulus causing mechanical blockage | Pain changes with movement; centralisation or peripheralisation occurs | Direction of preference (usually extension for lumbar; flexion occasionally) |
| Dysfunction Syndrome | Adaptive shortening or scarring of pain-sensitive structures | Pain only at end range; no centralisation | Exercises to stress the shortened structure progressively |
| Postural Syndrome | Pain from prolonged mechanical deformation of normal tissues | Pain only with sustained postures, relieves with movement | Postural correction, no repeated exercises needed |
The Centralisation Phenomenon — Core Concept
The most important clinical sign in McKenzie assessment.
- Centralisation = good prognostic sign → continue that movement direction
- Peripheralisation = bad sign → stop that direction, try the opposite
- Centralisation predicts success of conservative management
McKenzie Assessment Process
- Repeated movement testing — perform 10 repetitions in each direction (flexion, extension, lateral glide, combined) in standing and lying
- Observe effect on symptoms — centralisation, peripheralisation, no change
- Identify directional preference — the movement that centralises/abolishes pain
- Classify syndrome — Derangement, Dysfunction, or Postural
- Prescribe direction-specific exercises
Part 3: Extension Exercises — The McKenzie Lumbar Programme
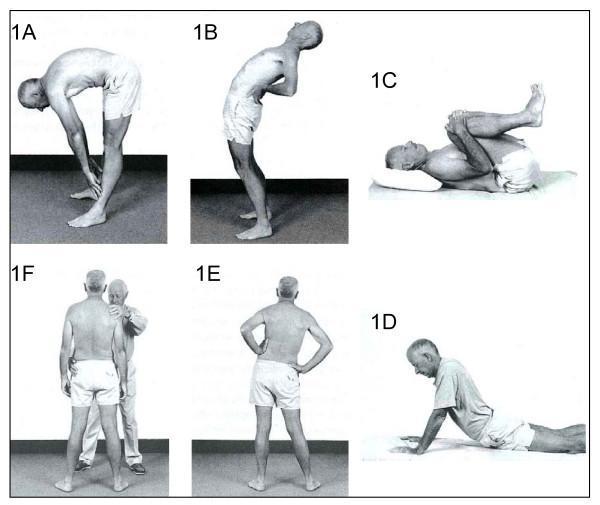
Extension Exercise Progression (Lumbar)
Stage 1 — Lying Prone (Passive Position)
- Lie face down, arms by sides, rest for 3–5 min
- Allows lumbar spine to naturally extend
- Used for acute, very painful patients
Stage 2 — Prone on Elbows
- Prop up on forearms (sphinx position)
- Partial extension loading
- Hold 2–3 min; repeat several times
Stage 3 — Prone Press-Up (Most Important)
- Lie prone; place hands under shoulders
- Push upper body up keeping hips/pelvis on the floor
- Elbows straighten fully → maximises lumbar extension
- 10–15 repetitions, multiple times/day
- Key: maintain passive lower body; do not activate glutes
Stage 4 — Standing Extension
- Stand with feet apart, hands on lower back
- Arch backward as far as possible, hold 2–3 seconds
- Useful when going from sitting to standing (office breaks)
- Repeat 10×, used as a prophylactic break
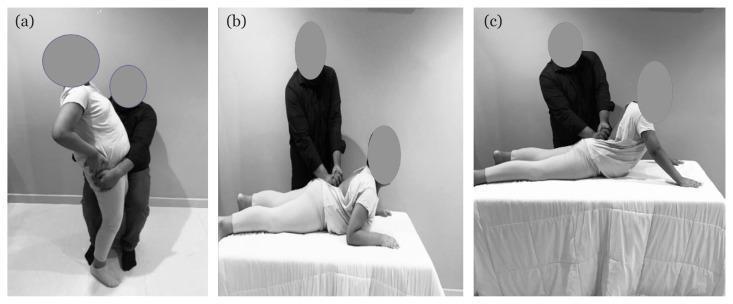
Stage 5 — Side Glide (Lateral Shift Correction)
- If patient has visible lateral shift (lean to one side)
- Stand sideways to wall; hip against wall
- Push hips toward wall while shoulders go away
- Corrects lateral shift before extension becomes effective
- Must be corrected first or extension will peripheralise
Stage 6 — Therapist-Assisted Techniques
- Passive extension mobilisations in prone
- Posterior-anterior (PA) pressures over spinous processes
- Combined with patient's own press-up movement
- Maitland grades I–IV can be layered onto McKenzie postures
When to Use Flexion Instead (McKenzie)
- Single or double knee-to-chest in supine
- Sitting forward bend
- Flexion in standing
- Used when extension peripheralises symptoms
Dosage & Frequency
| Parameter | Recommendation |
|---|---|
| Repetitions per set | 10–15 |
| Sets per session | 2–3 |
| Frequency | Every 2 hours during the day (key McKenzie principle) |
| Duration of programme | 4–6 weeks minimum |
| Home exercise | Critical — patient independence is the goal |
Part 4: Full Physiotherapy Programme for Disc Patients
| Phase | Goals | Interventions |
|---|---|---|
| Acute (0–2 weeks) | Pain relief, reduce inflammation, prevent neurological worsening | Relative rest, ice/heat, McKenzie prone lying/press-up, TENS/IFT, positioning advice |
| Subacute (2–6 weeks) | Restore range of motion, centralise symptoms | McKenzie extension progression, lateral shift correction, gentle neural mobilisation |
| Recovery (6–12 weeks) | Restore function, nerve gliding, core stability | McKenzie + core activation (transversus abdominis, multifidus), neural flossing |
| Maintenance | Prevent recurrence | Lumbar stabilisation programme, postural education, ergonomic advice |
Adjunct Physiotherapy Modalities
| Modality | Role |
|---|---|
| Traction (mechanical/manual) | Decompresses disc; reduces intradiscal pressure; useful for protrusion/extrusion |
| IFT | Deep pain relief, muscle spasm reduction |
| TENS | Nerve pain, radicular symptoms |
| Ultrasound | Periarticular soft tissue healing |
| Hot pack / SWD | Muscle relaxation before exercise |
| Neural mobilisation (nerve flossing) | Reduces intraneural adhesions in radiculopathy (SLR slump technique) |
| Dry needling | Lumbar multifidus and paraspinal trigger points |
Red Flags — Immediate Surgical Referral
- Cauda equina syndrome — bilateral leg pain, bladder/bowel dysfunction, saddle anaesthesia → surgical emergency
- Progressive neurological deficit (worsening foot drop)
- Severe pain not relieved at all with any position
- Cancer, infection, fracture suspected
Summary
DISC PATHOLOGY SPECTRUM:
Bulge → Protrusion → Extrusion/Prolapse → Sequestration
(contained) (free fragment)
Increasing severity ↑ | Better spontaneous resorption of extruded material ↑
McKENZIE PRINCIPLE:
Most posterior disc herniations → Extension is the directional preference
Extension loading shifts nucleus anteriorly → centralises pain → decompresses root
Test first: if extension centralises symptoms → continue extension programme
If extension peripheralises → check for lateral shift first, or try flexion
KEY EXERCISES:
Prone lying → Prone on elbows → Prone press-up (10× every 2 hrs)
→ Standing extension → Lateral shift correction → Stabilisation
Post op knee half squat,Full squat,lunges,hopes biomechanics,muscle work ,proper form to do and not to do ,when avoid or stop
squat biomechanics knee joint forces patellofemoral tibiofemoral post operative rehabilitation
lunge exercise biomechanics knee hip muscle activation rehabilitation
hop test single leg hop ACL return to sport knee rehabilitation criteria
full squat deep squat knee forces patellofemoral meniscus posterior cruciate ligament biomechanics
Post-Op Knee: Half Squat, Full Squat, Lunges & Hops — Biomechanics, Muscle Work, Form & Safety
Key Anatomical Context — Forces Acting on the Post-Op Knee
| Knee Flexion | Patellofemoral Joint Reaction Force (PFJRF) | Tibiofemoral Contact Force | ACL Stress | PCL Stress |
|---|---|---|---|---|
| 0–30° | Low (0.5× BW) | Low | High (anterior shear) | Low |
| 30–60° | Moderate (1–2× BW) | Moderate | Moderate | Low |
| 60–90° | High (3–4× BW) | High | Low | Moderate |
| >90° (deep squat) | Very High (6–8× BW) | Very High | Low | High (posterior tibial translation) |
- Post ACL reconstruction: avoid deep knee flexion early; more risk in 0–30° open chain extension (OKC) than in closed chain
- Post TKR (total knee replacement): patellofemoral stress is the limiting factor; avoid >90° loading early
- Post patellofemoral surgery / chondroplasty: minimise PFJRF — avoid full squats, stairs, lunges early
- Post PCL reconstruction: avoid deep flexion >70° early (PCL under maximum tension)
- Post meniscectomy / meniscal repair: deep squat increases compressive and shear stress on meniscal remnant — progress cautiously
1. HALF SQUAT (0–60° Knee Flexion)
Biomechanics
- A closed kinetic chain (CKC) exercise — foot fixed to ground, force transmitted through the entire chain
- At 0–60°: moderate quadriceps demand, low PFJRF, low ACL stress (compared to open chain extension in same range)
- Tibiofemoral compression moderate; meniscal load manageable
- Hip extensors (gluteus maximus) share significant load — co-contraction of hamstrings stabilises the knee
- Centre of mass stays over base of support
Primary Muscles Working
| Muscle Group | Role |
|---|---|
| Quadriceps (vastus medialis, lateralis, intermedius, rectus femoris) | Primary knee extensor; eccentrically controls descent |
| Gluteus maximus | Hip extension, posterior pelvic stability |
| Hamstrings (semimembranosus, semitendinosus, biceps femoris) | Co-contraction, posterior tibial stabilisation, ACL protection |
| Gastrocnemius / Soleus | Ankle stability, plantarflexion moment |
| Gluteus medius | Frontal plane hip stability, prevents knee valgus |
| Tibialis anterior | Controls ankle dorsiflexion |
| Core (transversus abdominis, multifidus) | Lumbopelvic stability |
Proper Form ✅
- Feet shoulder-width apart, toes slightly out (10–15°)
- Descend slowly and controlled (3 seconds down, 2 up)
- Knees track over 2nd–3rd toe — do not cave inward (valgus)
- Weight evenly distributed across entire foot — not on toes
- Trunk slight forward lean (normal hip hinge) — but spine neutral, no rounding
- Lower to 60° only — hip crease does NOT pass below knees in a half squat
- Eyes forward, chin neutral
Form Errors to Avoid ❌
- Knee valgus (knees diving inward) — overloads medial compartment and patellofemoral joint
- Heels lifting — ankle stiffness shifts load anteriorly; fix with heel wedge or ankle mobility work
- Forward trunk collapse — overloads lumbar spine, reduces quadriceps engagement
- Rapid uncontrolled descent — eccentric control is critical for joint protection
- Knee shooting past toes excessively — increases patellofemoral stress (some forward travel is normal)
- Holding breath / Valsalva — raises intra-abdominal pressure; exhale on ascent
Post-Op Application
- ✅ First closed-chain exercise introduced in most protocols (TKR, ACL, meniscal, patellofemoral)
- Typically introduced at 2–6 weeks depending on surgery
- Start with wall squat (wall behind back for guidance) or chair squat (sit-to-stand)
- Add resistance band above knees for VMO activation cue
- Progress: bodyweight → resistance band → goblet squat with load

2. FULL SQUAT (>90° to Full Flexion)
Biomechanics
- At >90° flexion: PFJRF rises steeply to 6–8× body weight
- Tibiofemoral compressive forces at maximum — greatest load on menisci and articular cartilage
- PCL under high tension (posterior drawer force on tibia)
- Hamstrings near full shortening — reduce active co-contraction capacity
- Calf-thigh contact at full flexion creates a "wrap-around" compressive force on posterior capsule
- Ankle dorsiflexion requirement: >35° — limited mobility → heel rise → increased anterior shear
Primary Muscles Working
Proper Form ✅
- Wide stance (slightly wider than shoulder width) aids depth without heel rise
- Deep squat requires full ankle dorsiflexion — address mobility first
- Maintain lumbar lordosis throughout — do NOT allow posterior pelvic tilt ("butt wink") at depth
- Knees remain over toes throughout
- Chest up, thoracic extension maintained
- Controlled tempo throughout — no bouncing at the bottom
Form Errors to Avoid ❌
- "Butt wink" (posterior pelvic tilt) at the bottom — collapses lumbar spine; increases disc and SI joint stress
- Heel rise — forced by ankle restriction; shifts knees forward, increases PFJRF dramatically
- Knee hyperextension on ascent — locks out joint, impaction injury to posterior structures
- Medial knee collapse throughout the movement
- Rapid "bounce" at the bottom — extreme compressive spike on menisci and cartilage
Post-Op Application
| Surgery | Full Squat Guidance |
|---|---|
| ACL reconstruction | Avoid until graft maturation (~4–6 months); introduce after half squat mastered and 90°+ ROM achieved |
| TKR / UKR | Typically limited to 90–100° by implant design; full deep squat rarely recommended |
| PCL reconstruction | Contraindicated early (high PCL strain >70°); introduce only after 4–6 months |
| Meniscal repair | Avoid until meniscus healed (~3–4 months); high compressive risk at depth |
| Meniscectomy (partial) | Earlier introduction (6–8 weeks) but watch for pain and effusion |
| Patellofemoral chondroplasty | Avoid or significantly limit — PFJRF very high; may never be appropriate |
3. LUNGES
Biomechanics
- A unilateral, single-leg-dominant CKC exercise
- Greater demand on hip extensors and frontal plane stability compared to squats
- Introduces lateral and rotational forces on the knee — tests dynamic stabilisers
- Front knee: quadriceps-dominant, 70–90° flexion → moderate-high PFJRF
- Rear knee: hip flexor stretch (iliopsoas, rectus femoris) + minor weight bearing
- Step length determines force distribution: short step → more knee-dominant (quad); long step → more hip-dominant (glute)
- Trunk position modulates load: upright = more quad; lean forward = more hip/glute
Primary Muscles Working
| Muscle | Front Leg Role | Rear Leg Role |
|---|---|---|
| Gluteus maximus | Primary hip extensor for ascent | Hip flexor stretch, minor push |
| Quadriceps | Knee extension, eccentric control of descent | Minor role |
| Hamstrings | Co-contraction, posterior tibial stability | Hip extension assist |
| Gluteus medius | Frontal plane stability — prevents hip drop | Stabilises pelvis |
| Gastrocnemius/Soleus | Ankle stability | Plantarflexion |
| Core | Trunk stability throughout | — |
Lunge Variations & Post-Op Relevance
| Type | Knee Angle | Difficulty | Best Post-Op Use |
|---|---|---|---|
| Static / Split squat | Fixed stance, 70–90° | Easiest | Early stage (4–8 weeks) |
| Forward lunge | 80–90° front knee | Moderate | Mid-stage (8–12 weeks) |
| Reverse lunge | 60–80° front knee | Lower PFJRF | Earlier than forward lunge — better control |
| Lateral lunge | Variable | High frontal plane demand | Late stage — tests MCL/LCL stability |
| Walking lunge | Dynamic 80–90° | Most advanced | Pre-return-to-sport stage |
Proper Form ✅
- Step forward so front shin remains roughly vertical (knee behind or at toes)
- Front knee tracks over 2nd–3rd toe
- 90° at front knee AND rear knee at bottom
- Trunk erect and vertical — avoid leaning over front knee
- Lower rear knee to ~2 cm above floor, then drive back up
- Push through front heel, not toes, to ascend
- Hips level throughout — no hip hike or drop
Form Errors to Avoid ❌
- Front knee diving past toes excessively → increases PFJRF
- Knee valgus (medial cave) — most common and most dangerous post-op
- Trunk lean forward — reduces quad engagement, increases knee stress
- Hip drop/Trendelenburg — gluteus medius weakness; increases ITB and lateral knee stress
- Pushing from rear leg rather than front — doesn't achieve intended strengthening
- Inadequate step length — makes it a knee-dominant mini-squat instead
Post-Op Application
- Start with split squat (static) — both feet stay fixed
- Progress to reverse lunge before forward lunge
- Add side step-up as an alternative if lunge loading is too great
- Walking lunge introduced at 3–4 months (ACL), 4–6 months (meniscal repair)
4. HOPS — Biomechanics & Return-to-Sport Role
- Rapid force generation (concentric)
- Shock absorption (eccentric deceleration)
- Dynamic joint stability under impact
- Neuromuscular control and reactive stiffness
Types of Hop Tests / Exercises
| Hop Type | Description | What It Tests |
|---|---|---|
| Single-leg hop for distance (SLHD) | Hop as far forward as possible on one leg, land and hold | Power, stability, confidence |
| Triple hop for distance | Three consecutive hops, hold on 3rd landing | Repeated power output |
| Crossover hop | Hop diagonally over a line 3 times | Lateral control, frontal plane stability |
| 6-metre timed hop | Hop 6 metres on one leg as fast as possible | Speed, reactive stiffness |
| Vertical hop / CMJ (countermovement jump) | Vertical jump single-leg or bilateral | Explosive power |
| Side hop | Lateral hops over a line | Rotational and valgus control |

Biomechanics of Hopping
- Take-off phase: Rapid concentric triple extension (hip, knee, ankle) — demands full strength of quadriceps, hamstrings, glutes, and calf
- Flight phase: Prepares for landing — pre-activation of stabilisers
- Landing phase (MOST CRITICAL post-op): Eccentric deceleration; GRF 3–5× body weight in <200ms; dynamic valgus at landing = most common ACL re-injury mechanism
Proper Landing Mechanics ✅ (Soft Landing Technique)
- Land with soft knees — do not land stiff-legged
- Simultaneous triple flexion at ankle, knee, and hip on contact
- Knee aligned over 2nd toe — no dynamic valgus
- Quiet landing — loud landing = poor eccentric control
- Hold landing for 3 seconds without hopping or staggering
- Trunk slightly forward over landing foot
Form Errors to Avoid ❌
- Stiff-legged landing — massive impact force through articular cartilage
- Knee valgus at landing — primary mechanism of ACL re-rupture
- Asymmetric landing (favouring the non-operated leg) — detected by Limb Symmetry Index (LSI)
- Trunk rotation or lateral lean on landing
- Looking down — impairs balance and dynamic alignment
Limb Symmetry Index (LSI) — Return-to-Sport Criterion
LSI = (Operated limb performance ÷ Non-operated limb) × 100
- LSI ≥90% across all four hop tests is the standard return-to-sport threshold (ACL)
- LSI <90% = not cleared for unrestricted sport return
5. When to AVOID or STOP — Red Flags & Clinical Criteria
Stop the Exercise Immediately If:
Contraindications by Surgery Stage
| Stage | Avoid |
|---|---|
| 0–2 weeks post-op | All squat/lunge/hop exercises; unprotected weight-bearing |
| 2–6 weeks (ACL, meniscal repair) | Full squat, lunge, any hopping; OKC extension 0–60° |
| TKR first 6 weeks | Deep flexion >90°, high-impact activities, uneven surfaces |
| 6–12 weeks | Plyometrics, running, hops, full-depth squats (until cleared) |
| Active infection / wound dehiscence | All weight-bearing exercise |
| Haemarthrosis / significant effusion | Any loaded knee exercise until effusion controlled |
| DVT | All lower limb exercise; refer urgently |
| Hardware failure / implant loosening symptoms | All exercise; refer urgently |
The "2-Hour Pain Rule" (Clinical Standard)
- If pain after exercise persists >2 hours or is worse next morning than before: load was too high
- Regress the exercise, reduce repetitions/sets, or reduce depth
- This rule applies to post-op knee rehabilitation universally
Effusion Grading — Exercise Modification Guide
| Effusion Grade | Finding | Exercise |
|---|---|---|
| 0 | No swelling | Progress normally |
| Trace | Minimal — just detectable | Proceed with caution |
| 1+ | Moderate swelling | Reduce load, no plyometrics |
| 2+ | Significant visible swelling | Regression, RICE, physiotherapy assessment |
| 3+ | Severe, tense | Stop all exercise, medical review |
6. Progressive Post-Op Knee Exercise Roadmap
WEEK 0–2: Isometrics (quad sets, SLR, VMO activation)
Heel slides, ankle pumps, CPM
WEEK 2–6: Mini squat (0–45°), wall slides
Terminal knee extension (TKE) with band
Step-up (low step, 5–10 cm)
Stationary bike (low resistance)
WEEK 6–12: Half squat (0–60°), sit-to-stand
Split squat / static lunge
Reverse lunge
Step-up (higher step, 15–20 cm)
Swimming, deep water running
MONTH 3–4: Half squat with load
Forward lunge
Lateral lunge
Leg press (full range, controlled)
Introduce jogging on flat
MONTH 4–6: Full squat (if ROM allows and cleared)
Walking lunge
Single-leg squat
Box step-down (eccentric control)
Begin hop training: bilateral → single-leg
MONTH 6+: Hop tests (LSI assessment)
Plyometrics, agility drills
Sport-specific return criteria
(LSI ≥90%, psychological readiness, strength ≥90%)
Summary Table
| Exercise | Knee Angle | PFJRF | Key Muscles | Post-Op Introduction | Avoid When |
|---|---|---|---|---|---|
| Half squat | 0–60° | Low–moderate | Quads, glutes, hamstrings | 2–6 weeks | Acute effusion, wound issues |
| Full squat | >90° | Very high | Quads, glutes, adductors, calves | 4–6 months | PCL recon, patellofemoral Sx, TKR |
| Lunge (static) | 70–90° | Moderate | Quads, glutes, hamstrings | 4–8 weeks | Valgus instability, effusion |
| Lunge (walking) | 80–90° dynamic | Moderate–high | Full lower chain + core | 3–4 months | Early post-op, instability |
| Hops | Variable (landing) | High (impact) | Full chain eccentric + reactive | 4–6 months | Before LSI ≥90%, effusion, pain |
Rabies,post exposure vaccine treatment
rabies post exposure prophylaxis WHO guidelines 2024 2025 vaccine schedule
Rabies & Post-Exposure Prophylaxis (PEP)
1. The Virus
"Rabies virus is a lyssavirus that infects a broad range of mammals and causes serious neurologic disease when transmitted to humans." — Harrison's Principles of Internal Medicine, 22nd Ed.
2. Epidemiology
- ~59,000 human deaths annually worldwide; >99% occur in Asia and Africa from dog bites
- More than 15 million people receive PEP annually (WHO)
- In the USA: endemic canine rabies eliminated; wildlife (bats, raccoons, skunks, foxes) are the primary reservoir; bats are the most common source of indigenously acquired human rabies
- Rabies-free zones: Hawaii, UK, Australia/New Zealand, Antarctica, Japan, most Pacific islands
| Vector | Region |
|---|---|
| Dogs | Asia, Africa, Latin America (>99% global deaths) |
| Bats | North & Latin America, Europe |
| Raccoons | Eastern USA |
| Skunks | Midwestern USA |
| Foxes | Europe, Arctic, North America |
| Mongoose | Asia, Africa, Caribbean |
3. Pathophysiology — How Rabies Kills
"After a bite, saliva containing infectious rabies virus is deposited in muscle and subcutaneous tissues. The virus remains close to the site of exposure for the majority of the long incubation period (typically 20–90 days). Rabies virus binds to the nicotinic acetylcholine receptor in muscle... Subsequently, the virus spreads across the motor end plate and ascends and replicates along the peripheral nervous axoplasm to the dorsal root ganglia, the spinal cord, and the CNS." — Tintinalli's Emergency Medicine
- Inoculation → virus in muscle/subcutaneous tissue at bite site
- Binding → nicotinic acetylcholine receptor at neuromuscular junction
- Retrograde axonal transport → ascent along peripheral nerves → spinal cord → brain
- CNS replication → limbic system, brainstem, cerebellum
- Centrifugal spread → outward to salivary glands, skin, cornea, heart, adrenals

4. Clinical Stages
| Stage | Duration | Features |
|---|---|---|
| Incubation | 20–90 days (range: days to years) | No symptoms; virus travelling along nerves |
| Prodrome | 2–10 days | Fever, malaise, anorexia, nausea/vomiting; paraesthesias, pain, or pruritus at the wound site (pathognomonic early sign) |
| Acute neurological — Encephalitic (80%) | 2–7 days | Anxiety, agitation, hyperactivity, bizarre behaviour, hallucinations, autonomic dysfunction, hydrophobia, aerophobia |
| Acute neurological — Paralytic (20%) | 2–10 days | Flaccid paralysis ascending from bite site → quadriparesis → facial palsy (resembles Guillain-Barré) |
| Coma → Death | 0–14 days | Virtually universal once symptoms appear |
Recovery is rare. — Harrison's Principles of Internal Medicine, 22nd Ed.
Hydrophobia — The Hallmark
- Attempts to swallow water trigger violent spasms of the throat and inspiratory muscles
- Caused by viral involvement of the brainstem (nucleus ambiguus, respiratory centres)
- Also aerophobia (spasms triggered by a puff of air on face)
- Hypersalivation + inability to swallow = classic "foaming at the mouth"
Incubation Determinants
- Short (days–weeks): bites to head, face, neck; deep wounds; multiple bites; high viral inoculum
- Long (months–years): bites to distal extremities; minor wounds; low viral inoculum
5. WHO Exposure Classification
| Category | Type of Exposure | Action |
|---|---|---|
| I | Touching/feeding animals; licks on intact skin | No PEP required |
| II | Nibbling of uncovered skin; minor scratches/abrasions without bleeding | Immediate vaccination only |
| III | Transdermal bites or scratches (bleeding); contamination of mucous membrane with saliva; licks on broken skin; exposure to bats | Immediate vaccination + Rabies Immunoglobulin (RIG) |
6. Post-Exposure Prophylaxis (PEP) — Step by Step
STEP 1: Immediate Wound Washing (Most Critical First Step)
"Elimination of rabies virus at the site of the infection by chemical or physical means is an effective mechanism of protection." — WHO
- Wash vigorously with soap and water for at least 15 minutes
- Then apply: povidone-iodine (10%), 70% ethyl alcohol, or aqueous iodine solution
- This single measure can markedly reduce the viral load and significantly decrease the risk of infection
- Do NOT suture the wound immediately — allows virus escape; if suturing needed, do so after local RIG infiltration
STEP 2: Rabies Immunoglobulin (RIG) — Passive Immunisation
| Product | Dose | Route |
|---|---|---|
| Human Rabies Immunoglobulin (HRIG) | 20 IU/kg body weight | Infiltrate as much as possible directly into and around wound(s); remainder IM at site distant from vaccine |
| Equine Rabies Immunoglobulin (ERIG) | 40 IU/kg body weight | Same as HRIG |
- Give on Day 0 (same day as first vaccine dose) — provides immediate passive protection while vaccine-induced immunity develops (takes 7–14 days)
- Do NOT give in the same syringe or site as the vaccine
- Do NOT give more than the calculated dose — excess RIG suppresses the active vaccine immune response
- If Day 0 has passed but vaccine series has begun, RIG can still be given up to Day 7 if not yet administered
- Not needed if previously vaccinated (immune memory provides rapid anamnestic response)
STEP 3: Rabies Vaccine — Active Immunisation
Modern Cell-Culture Vaccines (WHO-recommended — replacing nerve tissue vaccines)
| Vaccine | Cell Substrate |
|---|---|
| HDCV — Human Diploid Cell Vaccine | Human diploid lung cells (MRC-5) |
| PCECV — Purified Chick Embryo Cell Vaccine | Chick embryo cells |
| PVRV — Purified Vero Cell Rabies Vaccine (VERORAB) | Vero cells |
| PDEV — Purified Duck Embryo Vaccine | Duck embryo cells |
WHO strongly recommends the discontinuation of production and use of nerve tissue vaccines (Semple vaccine, suckling mouse brain vaccine) and their replacement by modern cell culture vaccines. — WHO
PEP Vaccine Schedules
A. Never Previously Vaccinated (Standard)
| Regimen | Doses | Days | Route | Site |
|---|---|---|---|---|
| Zagreb (2-1-1) | 4 doses total | 0, 0, 7, 21 | IM | Day 0: one dose each arm; Days 7 & 21: one dose |
| Essen (5-dose) | 5 doses | 0, 3, 7, 14, 28 | IM | Deltoid (adults); anterolateral thigh (children) |
| USA/CDC 4-dose | 4 doses | 0, 3, 7, 14 | IM | Deltoid |
| Immunocompromised | 5 doses | 0, 3, 7, 14, 28 | IM | + check antibody titre post-series |
| Regimen | Doses | Days | Volume per site |
|---|---|---|---|
| Updated Thai Red Cross (TRC) 2-site ID | 0, 3, 7, 28 | 0.1 mL × 2 sites | Days 0, 3, 7: 2 sites; Day 28: 1 site |
| WHO 4-site ID (4-4-4-4-1-1) | — | 0, 3, 7, 14, 28, 90 | 0.1 mL × 4 sites on days 0, 3, 7 |
B. Previously Vaccinated (Booster / Re-exposure)
| Regimen | Doses | Days |
|---|---|---|
| 2-dose IM | 2 | 0 and 3 |
| 1-site ID × 2 days | 2 | 0 and 3 |
STEP 4: Is PEP Still Effective If Delayed?
- PEP should be started as soon as possible
- However, it can still be initiated even weeks after exposure — as long as the patient shows NO symptoms of rabies (once symptoms appear, no treatment is effective)
- The sooner started, the better; delay is never a reason to withhold PEP
7. Risk Assessment — When Is PEP Needed?
| Situation | PEP Decision |
|---|---|
| Dog/cat/ferret bite — animal healthy, available for observation | Observe animal for 10 days; start PEP only if animal develops signs of rabies OR cannot be observed |
| Wild animal bite (bat, raccoon, skunk, fox) | Start PEP immediately unless animal tested negative |
| Rodent or rabbit bite (squirrels, hamsters, guinea pigs) | Almost never require PEP — these animals virtually never transmit rabies |
| Bat in room — sleeping person, child, intoxicated person (may not know if bitten) | Consider PEP — bat bites can be imperceptible |
| Intact skin contact only | No PEP |
| Person-to-person (except organ transplant) | No PEP |
| Bite in rabies-free country by known vaccinated pet | Risk very low; assess individually |
8. Pre-Exposure Prophylaxis (PrEP)
| Schedule | Doses | Days |
|---|---|---|
| IM (USA 2-dose updated ACIP) | 2 | 0 and 7 |
| IM (older 3-dose) | 3 | 0, 7, 21 or 28 |
| ID 2-dose | 2 | 0 and 7 |
9. Diagnosis (Clinical)
| Test | Specimen | Notes |
|---|---|---|
| Direct fluorescent antibody (DFA) | Brain tissue (post-mortem) | Gold standard |
| RT-PCR | Saliva, CSF, skin biopsy (neck), corneal impressions | Best antemortem test |
| Negri bodies (histology) | Brain | Classic but less sensitive |
| Serum neutralising antibodies | Blood | Diagnostic in unvaccinated; may be absent early |
| CSF antibodies | CSF | More specific than serum |
| MRI brain | — | Brainstem/grey matter signal changes; non-specific |
"A diagnosis of rabies often is not considered until relatively late in the clinical course... This diagnosis should be considered in patients presenting with acute atypical encephalitis or acute flaccid paralysis." — Harrison's Principles of Internal Medicine, 22nd Ed.
10. Treatment of Clinical Rabies
- Supportive ICU care: sedation, analgesia, mechanical ventilation
- Milwaukee Protocol (experimental): induced coma + antiviral therapy — very rare survivors reported; not widely adopted
- Palliative care is the mainstay
"No specific treatment is available. Vaccination immediately after animal bites prevents rabies disease." — Sherris & Ryan's Medical Microbiology
11. PEP Summary Card
ANIMAL BITE / EXPOSURE
↓
1. WASH WOUND — soap & water 15 min + povidone-iodine
↓
2. ASSESS EXPOSURE CATEGORY (WHO I / II / III)
↓
Category I → No PEP
Category II → Vaccine only (Days 0, 3, 7, 14)
Category III → RIG (20 IU/kg infiltrated into wound)
+ Vaccine (Days 0, 3, 7, 14)
↓
3. ASSESS PREVIOUS VACCINATION STATUS
Previously vaccinated → 2 vaccine doses only (Day 0 + 3), NO RIG
Never vaccinated → Full PEP as above
↓
4. ASSESS ANIMAL
Dog/cat/ferret — healthy → observe 10 days
Wild animal / bat → treat as rabid until proven otherwise
Rodents/rabbits → PEP rarely needed
↓
5. NEVER inject vaccine in GLUTEAL region
NEVER give RIG in same syringe as vaccine
NEVER withhold PEP because of delay — start even weeks later
↓
REMEMBER: Once symptoms appear → NO PEP is effective
54 year Male history of 1 year ago hamaragic stroke , RA,Gout, Hypothyroidism was able to flexion his shoulder 10 days ago but currently he is not able to lift the shoulder and complain of affected side extreme pain
Clinical Analysis: Acute Loss of Shoulder Flexion + Extreme Pain (10-Day Decline)
The Clinical Problem at a Glance
1. Priority Differential Diagnosis (Most to Least Urgent)
🔴 URGENT — Must Rule Out First
A. Acute Rotator Cuff Tear (Full-Thickness)
- The shoulder has been biomechanically vulnerable for 1 year — muscle imbalance, altered mechanics, disuse
- RA causes progressive rotator cuff tendon erosion — the supraspinatus, infraspinatus, and subscapularis tendons are destroyed by synovial pannus from within
- Even a trivial movement or minor fall can trigger acute complete tear through an already RA-eroded tendon
- Hypothyroid myopathy further weakens proximal muscles (elevated CK, non-inflammatory weakness) — reduces tendon protection
- Result: patient had partial function (compensated partial tear) → sudden complete rupture → complete inability to initiate active abduction/flexion (classic "drop arm")
- Inability to actively lift arm against gravity — but passive range may be preserved
- Severe acute pain, especially at night and with any movement
- Supraspinatus fossa atrophy if chronic component existed
- Drop arm sign positive — patient cannot hold arm elevated if passively placed there
"RA causes rotator cuff tears due to direct invasion by synovial pannus and indirect weakening of tendon vascularity — the shoulder joint is affected in up to 90% of patients with longstanding RA."
B. Glenohumeral Joint Dislocation / Subluxation (Acute)
- Stroke patients already have chronic inferior glenohumeral subluxation due to flaccid paralysis of periscapular muscles
- A fall, forceful passive range-of-motion exercise, or pulling on the arm can cause acute complete dislocation
- Presents with: marked pain, visual step deformity, complete loss of active motion, arm held in fixed position
- Check clinically for step deformity and compare shoulder contour bilaterally
C. Acute Septic Arthritis of the Glenohumeral Joint
- RA patients on DMARDs or steroids are immunosuppressed — high risk for septic arthritis
- Gout medications (colchicine, NSAIDs) do not protect against infection
- Presentation: acute severe joint pain, fever, warmth, erythema, inability to move
- This is a surgical emergency — joint destruction occurs in hours
- Red flags: fever, rigors, systemically unwell, hot/red/swollen joint, raised WBC/CRP/ESR
D. Acute Gout Attack — Shoulder (Tophaceous/Crystal Arthropathy)
- Gout can affect any joint, including the shoulder — often overlooked at this site
- Immobility (stroke) reduces urate clearance from the joint → crystal accumulation
- Diuretics (often used post-stroke for hypertension) raise uric acid
- Presents with: acute severe pain, swelling, warmth — episodic, may wake from sleep
- MSU crystals in joint fluid on aspiration (needle-shaped, negatively birefringent)
E. New Neurological Event / Recurrent Stroke
- Second haemorrhagic stroke (hypertension remains the dominant risk factor) affecting the motor cortex or corticospinal tract could cause acute worsening of hemiplegia
- Critical red flag if accompanied by: new facial droop, speech change, new headache, confusion, new leg weakness
- This is a neurological emergency — requires immediate CT head
🟡 IMPORTANT — Likely Contributing / Compounding Causes
F. Acute RA Flare — Glenohumeral Joint
- RA can flare acutely in the glenohumeral joint — synovial inflammation, joint effusion, severe pain
- Immobilised joints in stroke patients are prone to disuse synovitis and worsening RA activity
- Presents with: morning stiffness >1 hour, warmth, swelling, raised CRP/ESR, RF/anti-CCP elevation
- May cause pain-inhibited inability to move (pseudoparesis) rather than true structural failure
G. Spasticity-Related Shoulder Pain with Contracture Worsening
"Some 40–60% of patients develop shoulder pain after a stroke. The mechanism is not clear, but a strong association exists between pain and an abnormal shoulder joint examination, ipsilateral sensory abnormalities, and arm weakness. It is postulated that the pain is due to inflammation in the joint secondary to immobilisation and joint contracture (frozen shoulder syndrome)." — Bradley and Daroff's Neurology in Clinical Practice
- Over 1 year post-stroke, spasticity transitions from flaccid → spastic phase in most patients
- Increasing spasticity of pectoralis major, subscapularis, and biceps → internal rotation contracture
- The shoulder is held in adduction/internal rotation → severe pain with any attempt at flexion or abduction
- This can worsen suddenly after a period of reduced therapy, intercurrent illness, or painful stimulus
H. Adhesive Capsulitis (Frozen Shoulder) — Acute Phase
- Post-stroke immobility is the single biggest risk factor for adhesive capsulitis
- Stage 1 (Freezing): Extreme pain, global loss of movement — this matches the presentation
- The "freezing" phase can feel like a sudden deterioration after a period of limited function
- RA is an independent risk factor for adhesive capsulitis
- Hypothyroidism is an independent and well-established risk factor for adhesive capsulitis (connective tissue mucopolysaccharide deposition)
I. Hypothyroid Myopathy — Acute Worsening
"Patients with severe hypothyroidism can experience a non-inflammatory myopathy with proximal muscle weakness and an elevated creatine kinase level, which may be confused clinically with polymyositis." — Goldman-Cecil Medicine
- If the patient's hypothyroidism is undertreated or TSH has drifted high (common with medication compliance issues post-stroke), proximal myopathy worsens
- Presents with: proximal shoulder girdle and hip girdle weakness, elevated CK, fatigue
- Would cause bilateral proximal weakness — but on the already-weaker stroke side, it becomes clinically apparent on that side first
- Painless weakness typically, but if combined with other pathology, can amplify pain
J. Complex Regional Pain Syndrome (CRPS) Type 1
- Shoulder-hand syndrome post-stroke is a recognised form of CRPS
- Presents as: severe burning pain, allodynia, autonomic changes (colour, temperature, sweating) in hand and shoulder
- Usually develops 1–3 months post-stroke but can evolve or worsen at any time
- Immobility and repeated minor trauma (aggressive passive ROM) are triggers
2. Red Flag Assessment
| Red Flag | Suspected Diagnosis |
|---|---|
| Fever, rigors, systemically unwell, hot/red/swollen joint | Septic arthritis → EMERGENCY |
| New facial droop, speech change, new leg weakness, headache | Recurrent stroke → EMERGENCY |
| Visual step deformity at shoulder | Dislocation → URGENT |
| Passive ROM also completely blocked | Dislocation, septic arthritis, severe adhesive capsulitis |
| Passive ROM preserved, active lost | Rotator cuff tear (complete) |
| Severe warmth and swelling | Gout attack, RA flare, septic arthritis |
| Systemically well, gradual worsening over days | RA flare, adhesive capsulitis, spasticity |
3. Immediate Investigations
First-line (Emergency)
| Investigation | Purpose |
|---|---|
| X-ray shoulder AP + axillary | Dislocation, subluxation, glenohumeral joint space, RA erosions, calcification |
| CT head (urgent if new neuro signs) | Recurrent haemorrhagic stroke |
| FBC, CRP, ESR, WBC | Infection (septic arthritis), RA activity |
| Serum uric acid | Gout |
| Joint aspiration (if effusion present) | Microscopy for MSU crystals (gout), WBC count/culture (septic arthritis) |
| Serum CK | Hypothyroid myopathy |
| TSH, free T4 | Is hypothyroidism adequately controlled? |
Second-line (Guided by First-Line Results)
| Investigation | Purpose |
|---|---|
| MRI shoulder | Rotator cuff tear, tendon integrity, capsulitis, labral pathology |
| Ultrasound shoulder | Rotator cuff tear, effusion, subacromial bursitis (faster and cheaper than MRI) |
| Bone scan / SPECT | CRPS, occult fracture |
| RF, anti-CCP, ESR | RA disease activity |
4. Management — By Most Likely Diagnosis
If Septic Arthritis (Rule Out First)
- Urgent surgical washout/aspiration + IV antibiotics (do not delay)
- Anti-staphylococcal cover (flucloxacillin or vancomycin if MRSA risk)
- Do not start physiotherapy until infection controlled
If Acute Complete Rotator Cuff Tear
- Orthopaedic referral for surgical repair consideration
- Acute pain management: NSAIDs (caution post-stroke/renal), analgesics, suprascapular nerve block
- Physiotherapy: gentle passive ROM only until surgical decision made; no active loading of the torn tendon
- Post-repair: phased rehabilitation programme
If Glenohumeral Dislocation
- Immediate closed reduction under sedation/anaesthesia
- Post-reduction X-ray to confirm
- Arm sling for 2–3 weeks, then graduated physiotherapy
If Acute Gout Attack
- Colchicine 0.5 mg BD (first-line if no contraindication) OR
- NSAIDs short course (caution: post-stroke, renal function)
- Intra-articular corticosteroid if joint accessible — fastest relief
- Ice, rest, elevation
- Long-term: start/optimise allopurinol once attack settles
If Acute RA Flare
- Intra-articular corticosteroid injection (methylprednisolone 40–80 mg) — excellent for monoarticular flare
- Short course oral prednisolone if systemic flare
- Review DMARD therapy — may need escalation or biological agent
- Physiotherapy: gentle active-assisted ROM, TENS/IFT for pain, avoid aggressive stretching during active inflammation
If Adhesive Capsulitis (Frozen Shoulder)
- Pain management first: analgesics, NSAIDs, intra-articular steroid injection
- Hydrodilatation (distension arthrography) — highly effective for frozen shoulder
- Physiotherapy: gentle pendulum exercises, pain-free passive ROM — do NOT force movement
- Suprascapular nerve block for refractory pain
- Timeline: 12–18 months for natural resolution; intervention shortens this
If Spasticity-Related
- Botulinum toxin A injection to subscapularis, pectoralis major — gold standard for spastic shoulder
- Baclofen (oral or intrathecal for severe cases)
- Physiotherapy: stretching, positioning, splinting, IFT/TENS
- Shoulder sling with proper positioning during rest
If Hypothyroid Myopathy (Undercontrolled Hypothyroidism)
- Optimise levothyroxine dose — check TSH, target 0.5–2.5 mIU/L
- Weakness and CK elevation reverse with adequate thyroid hormone replacement
- Physiotherapy: gentle progressive resistive exercises as thyroid function normalises
5. Physiotherapy Approach (After Medical Diagnosis Confirmed)
DO NOT do until diagnosis is clear:
Safe to do while awaiting diagnosis:
Once diagnosis confirmed and acute phase managed:
| Goal | Intervention |
|---|---|
| Pain relief | TENS, IFT, ultrasound, heat/cold |
| Restore ROM | Passive → active-assisted → active ROM exercises |
| Prevent subluxation | Positioning, shoulder sling, taping |
| Rebuild strength | Rotator cuff strengthening (pendulum → isometric → isotonic) |
| Spasticity | Botox + stretching programme + positioning |
| Function | Task-specific training (reaching, dressing) |
| CRPS if present | Desensitisation, mirror therapy, graded motor imagery |
6. Summary — Priority Action List
STEP 1 — RULE OUT EMERGENCIES FIRST:
→ Check: Fever? New neuro signs? Joint hot/red/swollen?
→ X-ray shoulder + CT head (if any new neuro signs)
→ Blood: FBC, CRP, ESR, uric acid, CK, TSH
STEP 2 — ASSESS SHOULDER:
→ Active vs passive ROM comparison
Active lost + Passive preserved → Rotator cuff tear
Both lost → Adhesive capsulitis, dislocation, septic arthritis
→ Look for step deformity (dislocation)
→ Joint aspiration if effusion present
STEP 3 — TREAT CAUSE:
→ Septic arthritis → IV antibiotics + washout (EMERGENCY)
→ Dislocation → Reduction
→ Rotator cuff tear → Ortho referral + pain management
→ Gout → Colchicine + intra-articular steroid
→ RA flare → Intra-articular steroid + DMARD review
→ Spasticity → Botulinum toxin
→ Hypothyroid → Optimise levothyroxine
→ Adhesive capsulitis → Steroid injection + hydrodilatation
STEP 4 — PHYSIOTHERAPY:
→ Only after medical diagnosis confirmed
→ Start gentle, progress guided by pain and tissue healing
70 year old male having disc bulge or back pain and currently on cancer treatment with radio or chemotherapy having back to leg pain and not able to walk or stand or sit to stand role of physiotherapy
70-Year-Old Male: Disc Bulge/Back Pain + Active Cancer (Radio/Chemotherapy) + Leg Pain + Inability to Walk/Stand/Sit-to-Stand
⚠️ CRITICAL FIRST ALERT — This Is NOT Simply "Disc Bulge" Until Proven Otherwise
"Approximately 90% of patients with malignant spinal cord compression will have back pain... individuals with known cancer and back pain should undergo radiographic imaging." — Tintinalli's Emergency Medicine
"A recent onset of persistent back pain, particularly if in the thoracic spine, should prompt consideration of vertebral metastasis." — Harrison's Principles of Internal Medicine, 22nd Ed.
1. The Real Diagnostic Picture — What Is Causing This?
Layer 1: Pre-existing Disc Bulge (Known)
- Degenerative lumbar disc pathology at age 70 is near-universal
- Disc bulge causes back pain, radicular leg pain via nerve root compression
- BUT: disc bulge does NOT typically cause sudden inability to walk and stand in a patient who previously had some function
Layer 2: Cancer-Related Spinal Pathology (Must Rule Out Urgently)
🔴 A. Malignant Spinal Cord Compression (MSCC) — NEUROLOGICAL EMERGENCY
"Up to 20% of cancer patients will develop neoplastic involvement of the vertebral column, and 3–6% will develop spinal cord compression. Most cases are due to metastases to vertebral bodies from solid organ tumors, with the thoracic vertebrae being the most common location." — Tintinalli's Emergency Medicine
- Tumour metastasises to vertebral body → erodes cortex → enters spinal canal → compresses spinal cord or cauda equina
- The cancers most associated: breast, lung, prostate, kidney, lymphoma, myeloma
- Prostate and ovarian cancer preferentially spread to lumbar and sacral vertebrae via Batson's venous plexus
| Feature | This Patient |
|---|---|
| Known cancer on treatment | ✅ |
| Back pain | ✅ |
| Radicular leg pain | ✅ |
| Progressive proximal leg weakness | ✅ (can't walk/stand) |
| Inability to perform sit-to-stand | ✅ |
- Bladder dysfunction (urinary retention or incontinence)
- Bowel dysfunction (faecal incontinence or constipation)
- Saddle anaesthesia (numbness around perineum, inner thighs)
- Bilateral leg weakness (as opposed to one-sided)
"Weakness is most apparent in the proximal extremity musculature and may progress to complete paralysis. Urinary retention (with overflow incontinence), fecal incontinence, and impotence are late manifestations." — Tintinalli's Emergency Medicine
🔴 B. Cauda Equina Syndrome (CES) — SURGICAL EMERGENCY
- Severe bilateral leg pain and weakness
- Saddle anaesthesia
- Bladder and bowel dysfunction
- This can result from both disc herniation AND tumour compression — in a cancer patient, tumour cause must be assumed until proven otherwise
"Motor deficits (paraplegia or quadriplegia), once established for >12 h, do not usually improve, and beyond 48 h, the prognosis for substantial motor recovery is poor." — Harrison's Principles of Internal Medicine, 22nd Ed.
🟡 C. Pathological Vertebral Fracture
- Cancer metastases weaken vertebral bodies → collapse under normal weight-bearing loads
- A vertebral compression fracture causes acute severe back pain, neurological deterioration
- Can occur during something as minor as sitting down, coughing, or turning in bed
- Must assess spinal stability before ANY physiotherapy
🟡 D. Radiation Myelopathy
- If spine has been within the radiation field, radiation myelopathy can occur months to years after treatment
- Presents as progressive leg weakness, sensory loss, bowel/bladder dysfunction
- On MRI: T2 hyperintensity within the cord at the irradiated level
- Irreversible once established
🟡 E. Chemotherapy-Induced Peripheral Neuropathy (CIPN)
- Drugs like paclitaxel, oxaliplatin, vincristine, cisplatin cause dose-dependent peripheral neuropathy
- Presents as: bilateral distal sensory loss, burning pain, weakness in hands and feet
- Can significantly impair balance, gait, and standing ability
- Usually distal (stocking-glove distribution), not radicular
- Contributes to falls risk and functional deterioration
- This compounds any structural spinal pathology
🟡 F. Cancer-Related Fatigue and Deconditioning
- One of the most disabling consequences of chemotherapy and radiotherapy
- Profound proximal muscle weakness, fatigue, sarcopenia (cancer cachexia)
- Inability to generate enough force to stand or perform sit-to-stand
- Anorexia → protein deficiency → accelerated muscle loss
- Pain-induced immobility worsens deconditioning in a vicious cycle
🟡 G. Pre-existing Lumbar Disc Bulge — Now Worsened
- The known disc bulge is likely contributing to back and leg pain
- But in a cancer patient with worsening neurological function, it cannot be the only explanation
- Disc bulge + tumour = compound mechanical and compressive pathology
2. Immediate Medical Priority — Before Physiotherapy Resumes
Step 1 — Urgent Investigations
| Investigation | Purpose | Priority |
|---|---|---|
| MRI whole spine with gadolinium | MSCC, vertebral metastases, cauda equina compression, radiation myelopathy | URGENT — same day |
| CT spine | If MRI contraindicated; bone destruction, pathological fracture | Urgent |
| Bone scan / SPECT-CT | Extent of skeletal metastases | Urgent |
| Neurological examination | Motor power (MRC scale), sensory level, reflexes, anal tone, perineal sensation | Immediate |
| Bladder scan / urinalysis | Urinary retention | Immediate |
| Blood: FBC, CRP, Ca²⁺, ALP, LDH, PSA (if prostate) | Bone metastasis markers, infection | Same day |
| X-ray spine | Quick screen for vertebral collapse (less sensitive) | Immediate |
Step 2 — Emergency Medical Treatment (If MSCC Confirmed)
"Glucocorticoids (typically dexamethasone, 10 mg intravenously) can be administered before an imaging study if there is clinical suspicion of cord compression and continued at a lower dose (4 mg every 6 h orally) until definitive treatment." — Harrison's Principles of Internal Medicine, 22nd Ed.
| Treatment | Details |
|---|---|
| Dexamethasone | 10 mg IV stat → 4 mg every 6 hours; reduces cord oedema, may temporarily improve function |
| Radiotherapy | Standard treatment for MSCC; beneficial in ~70%; initiated as early as possible |
| Stereotactic body radiotherapy (SBRT) | For radioresistant tumours or re-irradiation |
| Surgery (selected cases) | Decompression + spinal fixation if: unstable spine, fracture, radioresistant tumour, worsening despite RT |
| Spinal bracing / orthosis | If spinal instability confirmed |
"A good response to therapy can be expected in individuals who are ambulatory at presentation... Treatment usually prevents new weakness, and some recovery of motor function occurs in up to one-third of patients." — Harrison's Principles of Internal Medicine, 22nd Ed.
3. Spinal Stability Assessment — SINS Score
| SINS Score | Stability Status | Physiotherapy Permission |
|---|---|---|
| 0–6 | Stable | Yes — physiotherapy can proceed with normal precautions |
| 7–12 | Potentially unstable | Physiotherapy with precautions; orthopaedic/oncology clearance required |
| 13–18 | Unstable | Spinal fixation required before any rehabilitation |
4. Role of Physiotherapy — Phased Approach
PHASE 0 — Pre-Clearance (While Awaiting Diagnosis)
PHASE 1 — Post-Diagnosis, Medically Stable (1–4 weeks)
A. Pain Management
| Modality | Application |
|---|---|
| TENS | Lumbar/leg pain; non-invasive; avoids systemic drugs |
| IFT (Interferential Therapy) | Deeper pain relief if no metal implants; reduces muscle spasm |
| Heat therapy (warm pack) | Paraspinal muscle spasm relief |
| Cold therapy | Acute inflammatory flare |
| Positioning | Semi-reclined, pillows under knees to reduce lumbar load; side-lying with pillow between knees |
| TENS caution | Do NOT use over or near the tumour site, over active cancer tissue |
B. Bed Mobility Training
- Rolling technique — log-rolling to maintain spinal alignment
- Pressure relief education — prevent sacral/heel pressure sores
- Bed transfers with spinal precautions
C. Respiratory Physiotherapy
- Incentive spirometry
- Active cycle of breathing techniques
- Prevent hypostatic pneumonia (major risk in bedbound patients on chemotherapy)
D. Circulatory/DVT Prevention
- Ankle pumps, calf exercises in bed
- Compression stockings (TED stockings) if medically approved
- Coordinate with medical team on anticoagulation status
PHASE 2 — Rehabilitation Phase (Post-Treatment Stabilisation)
A. Sitting Tolerance Programme
- Elevated head of bed (30° → 45° → 60° → 90°) — assess for orthostatic hypotension
- Sitting at edge of bed with support — 5 min → 10 min → 20 min
- Sitting in chair with armrests
- Assess sitting balance — static → dynamic
B. Sit-to-Stand Training
- Critical exercise for functional independence
- Begin with high seat (adjusted bed/chair height) + armrests → reduces hip/knee demand
- Use raised toilet seat aids in home environment
- Progress: high seat → standard chair → without arm support
- Technique: edge forward, feet under hips, lean forward from hips ("nose over toes"), push through arms and legs together
- Avoid Valsalva manoeuvre — raises intracranial and intrathoracic pressure (concern in known cancer)
- Use belt or gait belt for safety during early training
C. Standing Programme
- Tilt table — gradual upright positioning (30° → 45° → 60° → 90°) — avoids sudden postural hypotension
- Standing frame (standing aids) — maintains weight-bearing, reduces disuse osteoporosis
- Parallel bars standing — supported static → weight shift → stepping
- Zimmer frame walking — most stable initial walking aid post-MSCC
D. Gait Retraining
- Ankle-foot orthosis (AFO) — if foot drop present (L4/L5 compression)
- Rollator / wheeled Zimmer frame — for bilateral leg weakness
- Functional electrical stimulation (FES) — for foot drop from cord/root compression
- Gait pattern: short steps, wide base, weight through frame
- Progress: frame → elbow crutches → walking stick (if appropriate)
E. Lower Limb Strengthening (Spinal-Safe)
| Exercise | Technique | Precaution |
|---|---|---|
| Ankle pumps | In bed; calf pump | Safe at all stages |
| Quad sets (isometric) | Supine, press knee into bed | Safe |
| Straight leg raise | Supine; only if spinal stability confirmed | Assess SINS first |
| Hip abduction in lying | Side-lying | Safe if stable |
| Bridging | Supine, feet flat, lift hips | Only if stable spine, no fracture risk |
| Seated knee extension | In chair, resistance band | Safe seated |
| Sit-to-stand | As above | Progress carefully |
PHASE 3 — Maintenance and Functional Independence
A. Fatigue Management (Cancer-Related Fatigue)
- Energy conservation techniques — prioritise activities, pace throughout the day
- Rest-activity cycle — alternate active and rest periods (30 min activity : 30 min rest principle)
- Gentle aerobic exercise (short walks, stationary cycling) — proven to reduce cancer-related fatigue
- Avoid both complete bed rest (worsens fatigue) and overexertion (exhaustion)
B. CIPN Management (Chemotherapy-Induced Peripheral Neuropathy)
- Balance retraining — proprioceptive exercises; standing on foam, eyes closed progression
- Desensitisation — graduated tactile stimulation to feet
- Falls prevention — home hazard assessment, grab rails, non-slip footwear
- Hydrotherapy — reduces load through joints, improves proprioception in warm water
C. Psychological Support
- Cancer + chronic pain + disability → depression, anxiety are almost universal
- Physiotherapist's role: motivational interviewing, goal-setting, normalising limitations
- Coordinate with oncological psychologist/social worker
D. Equipment and Aids
| Aid | Purpose |
|---|---|
| Rollator / walking frame | Mobility with stability |
| Wheelchair | For long distances / high-fatigue periods |
| AFO | Foot drop correction |
| Raised toilet seat | Safe sit-to-stand in toilet |
| Perching stool | Activities of daily living while partially weight-bearing |
| Hospital bed at home | Height adjustment for transfers |
| TENS unit (home) | Ongoing pain management |
| Bath board/shower chair | Safe bathing |
5. Precautions Specific to Cancer Physiotherapy
| Precaution | Reason |
|---|---|
| Check platelet count before exercise | Chemotherapy causes thrombocytopenia; exercise risk for bleeding if platelets <50×10⁹/L |
| Check haemoglobin/anaemia level | Cancer anaemia → severe fatigue and exercise intolerance; physiotherapy may need modification |
| Avoid bone metastasis sites under impact or resistance | Pathological fracture risk |
| No spinal manipulation or high-velocity thrust | Vertebral involvement, fracture risk |
| No TENS/electrotherapy over tumour site or implanted devices | Contraindicated |
| Immune status — infection precautions | Chemotherapy → neutropenia; exercise in clean environments; physiotherapist hygiene critical |
| DVT vigilance | Cancer is a prothrombotic state + immobility; calf pain/swelling = stop, refer |
| Bone pain flare after radiotherapy | Temporary worsening 2–7 days post-RT (radiation flare); reduce intensity, reassess |
| Orthostatic hypotension | Common post-radiotherapy, opioids, bedrest; always check BP on standing |
6. Interdisciplinary Team — The Physiotherapist's Collaborators
| Team Member | Role |
|---|---|
| Oncologist | Cancer treatment plan, spinal stability clearance |
| Spine surgeon / Orthopaedic | Surgical decompression, spinal fixation, fracture management |
| Radiation oncologist | Radiotherapy planning for MSCC |
| Palliative care physician | Pain management, goals of care |
| Occupational therapist | ADL assessment, home modification, splinting |
| Dietitian | Nutritional support, address sarcopenia/cachexia |
| Pain specialist | Epidural steroid injections, nerve blocks for radicular pain |
| Neurologist | CIPN assessment, radiation myelopathy |
| Psychologist / Social worker | Coping, depression, discharge planning |
7. Summary — Priority Decision Tree
70M + CANCER (on radio/chemo) + BACK & LEG PAIN + CANNOT WALK/STAND
STEP 1 — RULE OUT EMERGENCY:
→ Bladder/bowel dysfunction? Saddle numbness?
YES → CAUDA EQUINA / MSCC → EMERGENCY IMAGING NOW
→ New neurological deterioration?
YES → MRI WHOLE SPINE WITH CONTRAST → SAME DAY
STEP 2 — ASSESS SPINAL STABILITY (SINS SCORE):
→ Unstable → Surgical consult before any rehab
→ Stable → Proceed with precautioned physiotherapy
STEP 3 — MEDICAL TREATMENT OF CAUSE:
→ MSCC → Dexamethasone + Radiotherapy ± Surgery
→ Pathological fracture → Surgical fixation
→ CIPN → Adjust chemo + neuropathic agents (gabapentin)
→ Deconditioning + fatigue → Physiotherapy + nutrition
STEP 4 — PHYSIOTHERAPY (PHASED):
Phase 0: No axial loading; bed exercises; prevent complications
Phase 1: Sitting tolerance; bed mobility; pain management
Phase 2: Sit-to-stand; standing; gait with aids
Phase 3: ADL independence; fatigue management; community mobility
ALWAYS: Check platelets, Hb, bone stability before advancing exercises
NEVER: Spinal manipulation, traction, extension loading without clearance
"A good response to therapy can be expected in individuals who are ambulatory at presentation... Motor deficits, once established for >12 h, do not usually improve, and beyond 48 h, the prognosis for substantial motor recovery is poor." — Harrison's Principles of Internal Medicine, 22nd Ed.
Women in her period what to do to comfort her ,reduce mood swings,pain
Supporting a Woman During Her Period — Pain, Mood Swings & Comfort
1. What Is Actually Happening — The Science
Why Pain Occurs (Dysmenorrhea)
"The etiology of primary dysmenorrhea includes excessive or imbalanced amounts of prostanoids secreted from the endometrium during menstruation. The prostanoids result in increased uterine contractions with a dysrhythmic pattern, increased basal tone, and increased active pressure. Uterine hypercontractility, decreased uterine blood flow, and increased peripheral nerve hypersensitivity contribute to pain." — Berek & Novak's Gynecology
- Cause the uterus to contract powerfully and irregularly
- Cut off blood flow to the uterine muscle (ischaemia) → cramping pain
- Cause systemic effects: nausea, diarrhoea, headache, fatigue, lower back pain, inner thigh pain
"NSAIDs successfully inhibit the formation of these prostaglandins and so relieve dysmenorrhea in 75–85% of cases." — Katzung's Basic & Clinical Pharmacology, 16th Ed.
Why Mood Swings Occur (PMS/PMDD)
- Low serotonin → irritability, sadness, low mood, anxiety, crying easily
- Low progesterone → reduced GABA activity → increased anxiety and tension
- Rising prostaglandins → fatigue, headache, and general discomfort amplify emotional reactivity
- Bloating and physical discomfort compound psychological distress
2. Pharmacological Relief — What Works
NSAIDs — First-Line, Most Effective for Pain
"Over-the-counter NSAIDs, which inhibit prostaglandin synthase (e.g., naproxen, ibuprofen), should be started as soon as bleeding or cramping begins and continued for up to 3 days." — Goldman-Cecil Medicine
| Drug | Dose | Notes |
|---|---|---|
| Ibuprofen | 400 mg every 6–8 hours with food | Best-evidence; start at first sign of cramps |
| Naproxen sodium | 500 mg every 12 hours | Longer-acting; fewer doses per day |
| Mefenamic acid | 500 mg loading → 250 mg every 8 hrs | Also reduces heavy flow |
| Diclofenac | 50 mg every 8 hours | Prescription; effective |
Paracetamol (Acetaminophen)
- Second-line if NSAIDs not tolerated
- 500–1000 mg every 4–6 hours (max 4 g/day)
- Less effective than NSAIDs for prostaglandin-mediated pain but useful combined with NSAIDs
Antispasmodics
- Hyoscine butylbromide (Buscopan) — reduces uterine spasm; effective for cramping
- 10–20 mg as needed
3. Non-Pharmacological Comfort Measures — Highly Effective
A. Heat Therapy — As Effective as Ibuprofen for Mild-Moderate Pain
- Hot water bottle or heating pad on the lower abdomen or lower back
- Maintain at ~40°C for 20–30 minutes
- Heat relaxes uterine smooth muscle, increases local blood flow, reduces ischaemia
- Research shows continuous low-level heat = comparable to ibuprofen for mild dysmenorrhea
- Warm baths or showers — whole-body muscle relaxation + heat effect
B. Transcutaneous Electrical Nerve Stimulation (TENS)
- A TENS unit placed on the lower abdomen/sacrum provides excellent non-drug pain relief
- High-frequency TENS (conventional) activates gate control mechanism → blocks pain signals
- Safe, drug-free, can be used continuously during the day
C. Massage
- Lower abdominal massage with gentle circular movements — reduces prostaglandin-mediated spasm
"The pain of dysmenorrhea is colicky in nature and, unlike abdominal pain caused by peritonitis, is relieved by abdominal massage, counterpressure, or movement of the body." — Berek & Novak's Gynecology
- Lower back massage — especially effective for back-referred menstrual pain
- Essential oils (lavender, clary sage, marjoram) in a carrier oil have evidence for reducing period pain when massaged abdominally
D. Exercise
- Light aerobic exercise — walking, gentle yoga, swimming — releases endorphins, reduces prostaglandin effects, improves pelvic circulation
- This feels counter-intuitive when fatigued but is evidence-backed
- Yoga poses particularly helpful:
- Child's pose (Balasana) — stretches lower back and pelvis
- Supine twist — relieves lower back tension
- Knees-to-chest — gentle uterine compression relief
- Cat-cow stretch — mobilises lumbopelvic region
E. Dietary Adjustments
| What Helps | Why |
|---|---|
| Omega-3 fatty acids (fish, flaxseed, walnuts) | Reduces PGE2 synthesis; studies show reduced dysmenorrhea severity |
| Magnesium (dark chocolate, nuts, leafy greens, or supplement 300–400 mg/day) | Reduces uterine smooth muscle spasm; also helps mood |
| Vitamin D (sunlight, supplementation) | Reduces prostaglandin production; deficiency linked to worse dysmenorrhea |
| Vitamin B1 (thiamine) 100 mg/day | Studies show significant reduction in dysmenorrhea |
| Ginger (tea or capsule 250 mg 4x/day) | Anti-prostaglandin effect; shown to reduce period pain similar to NSAIDs in some studies |
| Chamomile tea | Antispasmodic and anxiolytic; reduces uterine spasm |
| Turmeric (curcumin) | Anti-inflammatory; reduces prostaglandin pathway |
| What to Reduce | Why |
|---|---|
| Salt | Reduces bloating and water retention |
| Caffeine | Vasoconstricts blood vessels; increases pain sensitivity; worsens anxiety and irritability |
| Alcohol | Interferes with hormone balance; worsens mood the next day |
| Refined sugar | Spikes then crashes blood sugar → worsens mood swings |
| Processed/inflammatory foods | Increase prostaglandin production |
4. Managing Mood Swings Specifically
Understanding First
Practical Strategies
Nutrition for Mood
- Complex carbohydrates (oats, brown rice, sweet potato) — sustain serotonin levels throughout the day
- Protein at every meal — provides tryptophan for serotonin synthesis
- Magnesium-rich foods — natural muscle relaxant and mood stabiliser
- Avoid sugar crashes — eat small, frequent meals rather than skipping meals
Movement
- Even a 20-minute walk raises endorphins and stabilises mood
- Yoga and stretching reduce cortisol and promote parasympathetic (rest-and-digest) activity
Sleep
- Prioritise 7–9 hours of quality sleep — progesterone drop disrupts sleep; poor sleep dramatically worsens mood
- Warm bath before bed + no screens helps sleep onset
Stress Reduction
- Deep breathing exercises — box breathing (inhale 4 counts, hold 4, exhale 4, hold 4) activates the vagus nerve, calms the nervous system
- Mindfulness / meditation — even 10 minutes reduces cortisol and emotional reactivity
- Journalling — externalising frustration reduces its grip
Supplements with Evidence for PMS Mood
| Supplement | Dose | Evidence |
|---|---|---|
| Magnesium glycinate | 300–400 mg/day | Reduces irritability, bloating, low mood in PMS |
| Vitamin B6 (pyridoxine) | 50–100 mg/day | Supports serotonin and dopamine synthesis; reduces PMS mood symptoms |
| Calcium | 1000–1200 mg/day | Multiple RCTs show significant reduction in PMS symptoms including mood |
| Evening primrose oil | 1000–2000 mg/day | Reduces breast tenderness and mood symptoms |
| Agnus castus (Vitex) | 20–40 mg/day | Herbal; reduces PMS including mood swings in multiple trials |
5. How to Support Her — If You Are a Partner, Family Member, or Friend
What Helps Most
What NOT to Do
6. When to See a Doctor — Red Flags
- Pain is getting worse over years (not better)
- Pain begins days before the period (possible endometriosis)
- Pain occurs mid-cycle (possible ovarian cyst)
- Associated with heavy bleeding, clotting, irregular periods
- Pain during sex (dyspareunia) — suggests endometriosis or pelvic inflammatory disease
- NSAIDs provide no relief despite correct dosing
- Associated with fever or unusual discharge (possible PID/infection)
"If the dysmenorrhea persists, addition of an oral contraceptive to inhibit ovulation and limit the release of prostaglandin is generally effective. If pelvic pain remains intractable, additional evaluation is warranted." — Goldman-Cecil Medicine
Summary Card
PAIN RELIEF:
→ Ibuprofen 400mg every 6-8hrs (start early, with food)
→ Heat pad on lower abdomen (40°C, 20-30 min)
→ Abdominal + lower back massage
→ TENS unit (sacral/lower abdominal placement)
→ Ginger tea, chamomile tea
MOOD SUPPORT:
→ Magnesium + B6 + Calcium supplementation
→ Small frequent meals with complex carbs + protein
→ Reduce caffeine, sugar, alcohol
→ Gentle walk / yoga / movement
→ Deep breathing / mindfulness
→ Prioritise sleep
COMFORT FROM OTHERS:
→ Believe the pain
→ Ask what she needs
→ Reduce her load
→ Warm food, hot water bottle, quiet environment
→ Gentle physical presence (if wanted)
→ Do NOT minimise, dismiss, or argue
23 year girl sometime get pain before 3 days period starts have some belly fat, also fat around chin area ,some time thirsty
23-Year-Old Female: Pre-Period Pain, Belly Fat, Fat Around Chin, Occasional Thirst
1. Putting the Symptoms Together — What the Pattern Suggests
| Symptom | What It Suggests |
|---|---|
| Pain 3 days before period | PMS/premenstrual dysphoric disorder (PMDD) or prostaglandin-driven dysmenorrhea; also seen in PCOS due to irregular ovulation |
| Belly fat (central/abdominal adiposity) | Insulin resistance, PCOS, hypothyroidism, or cortisol excess |
| Fat around the chin/jaw area | Subcutaneous facial fat deposition — seen in PCOS (androgenic fat distribution), insulin resistance, Cushing syndrome (moon face), or hypothyroid |
| Occasional thirst | Insulin resistance/early pre-diabetes, increased blood glucose, or simply dehydration — but worth investigating |
2. Most Likely Primary Diagnosis: PCOS (Polycystic Ovary Syndrome)
What Is PCOS?
"PCOS may be defined as LH-dependent hyperandrogenism. The Rotterdam criteria require the presence of at least two of the following: oligo- or anovulation, clinical and/or biochemical signs of hyperandrogenism, and polycystic ovaries." — Berek & Novak's Gynecology
Why These Symptoms Fit PCOS
"The prevalence of obesity is high in PCOS and significantly increases the risk of comorbidities including metabolic syndrome, type 2 diabetes, dyslipidemia, hypertension, and cardiovascular disease." — Harrison's Principles of Internal Medicine, 22nd Ed.
"Insulin resistance, especially in skeletal muscle and adipose tissue, also contributes to increased insulin-stimulated ovarian androgen production." — Harrison's Principles of Internal Medicine, 22nd Ed.
| Feature | How PCOS Explains It |
|---|---|
| Belly fat | Insulin resistance → excess insulin → fat stored preferentially around abdomen (visceral and central adiposity) |
| Fat around chin/jaw | Androgen excess → fat distribution changes; also insulin-driven facial fat deposition |
| Pre-period pain | Irregular ovulation → abnormal progesterone decline → exaggerated prostaglandin release → pain before AND during periods |
| Thirst | Insulin resistance → mild hyperglycaemia → osmotic thirst |
The Hormonal Cascade in PCOS
High LH → Ovaries produce excess androgens (testosterone)
↓
Insulin resistance → Excess insulin → More androgen production
↓
Disrupted ovulation → Irregular periods / pre-period pain
↓
Excess androgens → Central fat, facial fat changes, acne, facial hair
↓
Metabolic effects → Pre-diabetes risk, thirst, fatigue
Other PCOS Features to Look For (History)
- Are periods regular? Or irregular (coming early/late/skipping)?
- Any unusual facial or body hair (above upper lip, chin, chest)?
- Any acne, especially on the jaw and chin?
- Any hair thinning on the scalp?
- Any skin darkening in neck folds, armpits, groin? (Acanthosis nigricans — a sign of insulin resistance)
3. Other Conditions to Consider
Hypothyroidism
- The thyroid gland slows down → reduced metabolism → weight gain (especially around the belly)
- Associated with: fatigue, cold intolerance, constipation, heavy or irregular periods, dry skin, hair loss, brain fog
- Very common in young women; easy to screen (TSH blood test)
- Can coexist with PCOS or mimic it
"Hypothyroidism should be excluded as a cause of irregular menses and hyperandrogenism before confirming PCOS diagnosis." — Harrison's Principles of Internal Medicine, 22nd Ed.
Insulin Resistance / Pre-Diabetes
- At 23, with belly fat, thirst, and possible PCOS, insulin resistance is very likely
- The body produces insulin but cells don't respond properly → blood glucose drifts higher → thirst, fatigue, weight gain around the abdomen
- Does NOT require actual diabetes to cause these symptoms
- A fasting glucose, HbA1c, or 75g oral glucose tolerance test can diagnose this
Cushing Syndrome (Less Likely but Worth Considering)
"Patients with Cushing syndrome may present with central obesity, a round face (moon facies), and a fat pad at the back of the neck (buffalo hump)." — Lippincott Illustrated Reviews: Pharmacology
- Caused by excess cortisol (stress hormone) — from adrenal gland tumour, pituitary tumour, or steroid medication use
- The "fat around the chin/jaw" + belly fat + irregular periods could fit
- Distinguished from PCOS by: skin stretch marks (purple striae), easy bruising, muscle weakness, high blood pressure, 24-hour urinary cortisol
4. What Investigations Are Needed (See a Doctor)
Blood Tests (Fasting)
| Test | Purpose |
|---|---|
| TSH (Thyroid Stimulating Hormone) | Rule out hypothyroidism |
| Free T4 | Thyroid function |
| Fasting glucose + HbA1c | Pre-diabetes/insulin resistance |
| Fasting insulin | Insulin resistance (HOMA-IR calculation) |
| 75g Oral Glucose Tolerance Test (OGTT) | Gold standard for glucose metabolism |
| Total testosterone + free testosterone | PCOS androgen excess |
| LH:FSH ratio | Elevated LH (>2:1) suggests PCOS |
| Prolactin | Elevated prolactin can cause similar symptoms |
| DHEAS (dehydroepiandrosterone) | Adrenal androgen source |
| Fasting lipid profile | Cholesterol, triglycerides (often abnormal in PCOS) |
| Cortisol (AM) | If Cushing suspected |
Imaging
| Test | Purpose |
|---|---|
| Pelvic ultrasound (transvaginal preferred) | Polycystic ovaries — ≥20 antral follicles or ovarian volume ≥10 cm³ confirms PCOS |
Diagnosis of PCOS (Rotterdam Criteria 2023)
- Irregular periods (fewer than 8 per year, or cycles >35 days)
- Clinical or biochemical hyperandrogenism (elevated testosterone, acne, hirsutism)
- Polycystic ovaries on ultrasound OR elevated AMH
"PCOS is a diagnosis of exclusion — other etiologies (hypothyroidism, hyperprolactinemia, adrenal sources) must be excluded first." — Harrison's Principles of Internal Medicine, 22nd Ed.
5. Management — What Can Be Done
A. Lifestyle — The Most Powerful Treatment
"Lifestyle management should be recommended in all women with PCOS." — Harrison's Principles of Internal Medicine, 22nd Ed.
Diet
| What to Do | Why |
|---|---|
| Low glycaemic index (low-GI) diet | Keeps blood sugar stable → reduces insulin spikes → reduces androgen stimulation |
| High protein at every meal | Satiating, reduces insulin response, preserves muscle |
| Plenty of vegetables and fibre | Slows glucose absorption, feeds gut bacteria, reduces inflammation |
| Healthy fats (avocado, olive oil, nuts, fatty fish) | Anti-inflammatory; reduce PCOS symptoms |
| Reduce refined carbs (white bread, white rice, sugary drinks, sweets) | Major drivers of insulin spikes in PCOS |
| Reduce processed sugar | Directly drives insulin resistance |
| Stay hydrated (2–2.5L water/day) | Addresses thirst symptom; reduces cortisol; aids metabolism |
- Inositol (myo-inositol) — found in fruit, beans, grains; shown to reduce insulin resistance, restore ovulation, and reduce androgens in PCOS
- Cinnamon — improves insulin sensitivity
- Spearmint tea (2 cups/day) — shown to reduce androgen levels
Exercise
| Type | Frequency | Benefit |
|---|---|---|
| Aerobic exercise (walking, cycling, swimming, dancing) | 30 min, 5×/week | Reduces insulin resistance; burns visceral fat; improves mood |
| Resistance/strength training | 2–3×/week | Builds muscle → improves glucose uptake → reduces insulin |
| HIIT (High Intensity Interval Training) | 2–3×/week | Highly effective for PCOS metabolic features |
| Yoga | Daily if possible | Reduces cortisol, improves hormone balance, reduces period pain |
B. Medical Treatment
"The first-line treatment of women with PCOS not attempting pregnancy is combined hormonal contraceptives to regulate menstrual cycles and decrease serum androgens by increasing sex hormone-binding globulin levels." — Harrison's Principles of Internal Medicine, 22nd Ed.
| Treatment | Purpose | Notes |
|---|---|---|
| Combined oral contraceptive pill (OCP) | Regulates periods, reduces androgens, reduces acne/hirsutism | First-line medical treatment |
| Metformin | Reduces insulin resistance, restores ovulation, helps weight loss | Especially if glucose abnormal; started low, increased slowly |
| Spironolactone | Anti-androgen — reduces facial fat/hair, acne | Added if OCP insufficient after 6 months |
| Myo-inositol supplement (2–4g/day) | Reduces insulin resistance naturally; improves ovulation | Evidence-based, safe, available OTC |
| Vitamin D (if deficient) | Commonly low in PCOS; improves insulin sensitivity and mood | Check level first |
| Magnesium (300–400mg/day) | Reduces insulin resistance; also helps pre-period pain and mood | Very safe supplement |
- Ibuprofen 400mg every 6–8 hours starting 1–2 days before expected period
- Heat pad on lower abdomen
- Magnesium and B6 — reduce prostaglandin sensitivity and cramping
C. Emotional and Psychological Support
"There is a high prevalence of depression and anxiety disorders, as well as disordered eating and body image distress [in PCOS]." — Harrison's Principles of Internal Medicine, 22nd Ed.
- The belly fat and facial fat are not due to overeating or laziness — they are driven by hormonal and metabolic abnormalities. Understanding this reduces shame and self-blame.
- Seek support: a counsellor, a PCOS-knowledgeable doctor, an online community of women with PCOS
- Regular sleep (7–9 hours) significantly improves insulin sensitivity and hormone balance
- Stress management: high cortisol worsens insulin resistance and androgen production
6. Red Flags — Urgent Review Needed If:
7. Summary
LIKELY DIAGNOSIS: PCOS with Insulin Resistance
SYMPTOMS EXPLAINED:
Belly fat → Insulin resistance + androgenic fat distribution
Chin/jaw fat → Androgen-driven fat changes; insulin effect
Pre-period pain → Hormonal dysregulation; irregular ovulation
Thirst → Insulin resistance → mild blood glucose elevation
WHAT TO DO NOW:
1. See a doctor → Blood tests: TSH, fasting glucose, HbA1c,
testosterone, LH, FSH, insulin, prolactin
2. Pelvic ultrasound
3. Start lifestyle changes NOW (low-GI diet + daily exercise)
4. Consider myo-inositol 2g/day supplement
5. Discuss OCP + metformin with doctor if PCOS confirmed
FOR PRE-PERIOD PAIN:
→ Ibuprofen before pain peaks + heat pad + magnesium
FOR THIRST:
→ Increase plain water; reduce sugary drinks; check blood glucose