Respiratory system clinical anatomy
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
I now have comprehensive content to write a detailed answer. Let me compile everything into a well-structured response.
Respiratory System - Clinical Anatomy
Overview
The respiratory system is divided into the upper airway (nose, mouth, pharynx, larynx) and the lower airway (trachea, bronchial tree, lungs). Clinically, anatomy is best organized into four functional units: the thoracic cage & muscles, the tracheobronchial tree, the alveolar unit, and the pulmonary circulation.
1. Thoracic Cage & Muscles of Respiration
The rib cage houses both lungs, each surrounded by its own pleura. The apex is small - admitting only the trachea, esophagus, and great vessels. The base is formed by the diaphragm.
Diaphragm
The diaphragm is the principal muscle of respiration, responsible for 75% of the change in chest volume during quiet breathing. Its contraction causes the thoracic base to descend 1.5 to 7 cm, expanding lung volume.
Accessory Muscles
| Muscle Group | Role |
|---|---|
| External intercostals | Assist inspiration (upward/outward rib movement) |
| Sternocleidomastoid | Elevates rib cage during forced inspiration |
| Scalene muscles | Prevent inward displacement of upper ribs |
| Pectoralis (with fixed arms) | Assists chest expansion |
| Abdominal muscles (rectus, obliques, transversus) | Active expiration |
| Internal intercostals | Assist downward rib movement (expiration) |
Clinical point: Expiration is passive in the supine position but becomes active in the upright position and with increased effort.
Pharyngeal Muscles & Airway Patency
The genioglossus maintains tonic inspiratory activity to keep the tongue away from the posterior pharyngeal wall. The levator palati, tensor palati, palatopharyngeus, and palatoglossus prevent the soft palate from falling back, especially in the supine position. Loss of this tone is a major factor in obstructive sleep apnea.
2. Tracheobronchial Tree
Trachea
- Begins at the lower border of the cricoid cartilage (the narrowest part of the adult airway: ~17 mm in men, ~13 mm in women)
- Extends to the carina - average length 10-13 cm
- Composed of C-shaped cartilaginous rings - anterior and lateral walls are cartilaginous; posterior wall is membranous
- Bifurcates at the sternal angle (angle of Louis) into right and left mainstem bronchi
Right vs. Left Mainstem Bronchus
| Feature | Right | Left |
|---|---|---|
| Angle with trachea | More linear (steeper takeoff ~25°) | More angular (~45°) |
| Length to first branch | ~2.0 cm (men), ~1.5 cm (women) to RUL | 5.0 cm (men), 4.5 cm (women) |
| Clinical implication | Foreign bodies more commonly enter right bronchus | Longer - more time for endobronchial tube malposition |
Clinical point: Because the right mainstem bronchus is more in line with the trachea, aspirated foreign bodies, malpositioned endotracheal tubes, and inadvertent endobronchial intubation most commonly affect the right lung.
Dichotomous Branching - 23 Generations
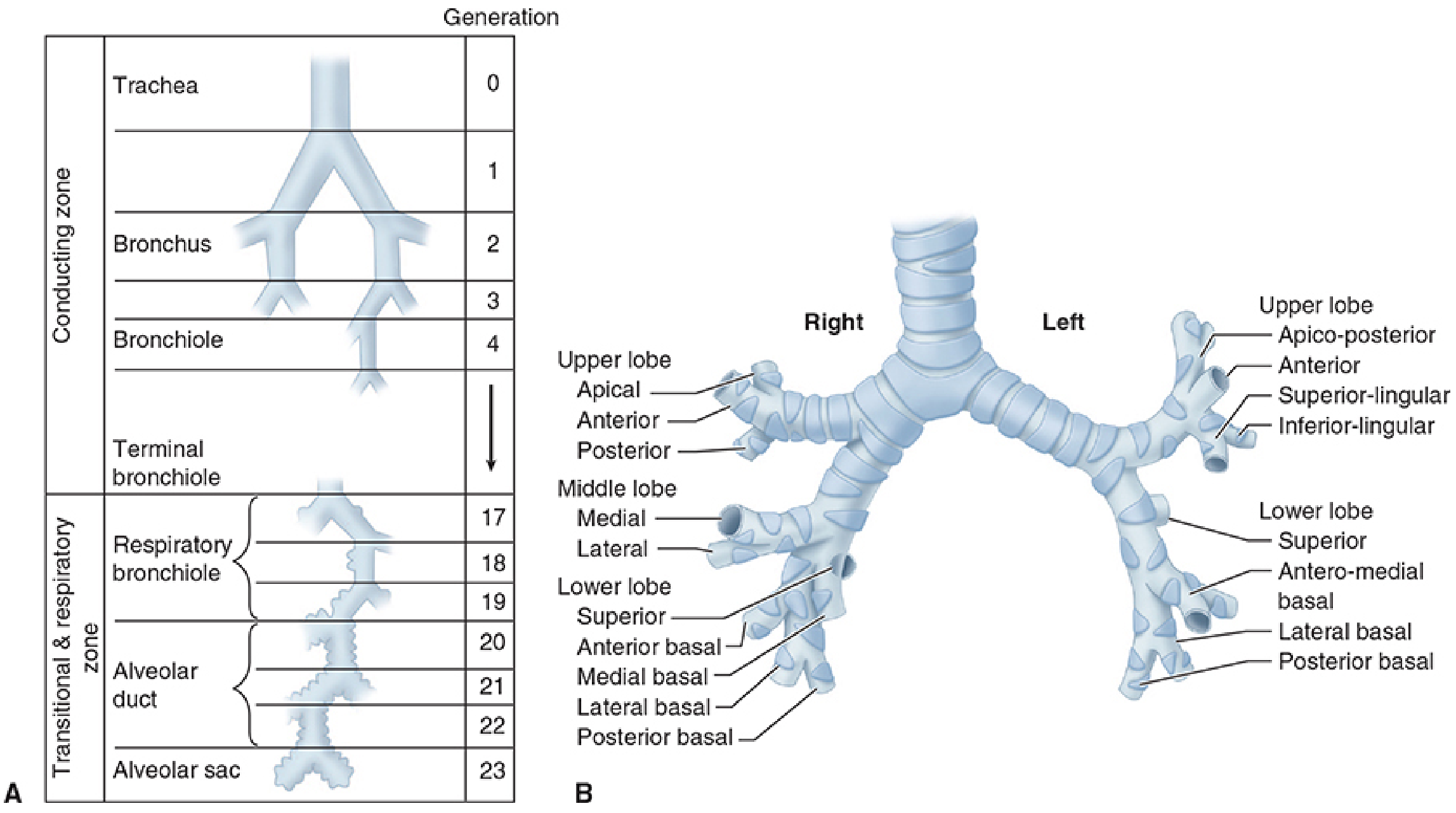
The airway divides through approximately 23 generations from trachea (generation 0) to alveolar sac (generation 23):
| Zone | Generations | Structures | Function |
|---|---|---|---|
| Conducting zone | 0-16 | Trachea → bronchi → bronchioles → terminal bronchioles | Gas conduction only (anatomical dead space) |
| Transitional & respiratory zone | 17-23 | Respiratory bronchioles → alveolar ducts → alveolar sacs | Gas exchange begins |
- Each generation approximately doubles the number of airways
- Cartilaginous support disappears at the bronchiolar level; smaller airways then depend on radial traction from surrounding parenchymal elastic recoil to stay patent
- Mucosa transitions from ciliated columnar epithelium (upper airways) → cuboidal → flat type I alveolar epithelium (gas exchange zones)
Lobar & Segmental Anatomy
- Right lung: 3 lobes (upper, middle, lower), 10 segments
- Upper lobe: Apical, Anterior, Posterior
- Middle lobe: Lateral, Medial
- Lower lobe: Superior, Anterior basal, Medial basal, Lateral basal, Posterior basal
- Left lung: 2 lobes (upper, lower), 8-9 segments (apical and posterior are fused as apico-posterior; lingual replaces middle lobe)
- Upper lobe: Apico-posterior, Anterior, Superior lingular, Inferior lingular
- Lower lobe: Superior, Antero-medial basal, Lateral basal, Posterior basal
3. The Alveolar Unit
There are an estimated 300-500 million alveoli, providing a gas-exchange surface area of 50-100 m².
Alveolar Cell Types
| Cell | Description | Function |
|---|---|---|
| Type I pneumocyte | Flat, form tight 1-nm junctions | Primary gas-exchange surface; barrier prevents albumin leak |
| Type II pneumocyte | Round, contain lamellar bodies; more numerous | Produce surfactant; can divide and regenerate type I cells |
| Pulmonary alveolar macrophages | Mobile | Innate immune defense |
| APUD cells, mast cells, lymphocytes | Present in lower airways | Immune/neuroendocrine functions |
Clinical point: Type II pneumocytes are the progenitor cells of the alveolar epithelium. Surfactant deficiency (as in premature neonates) leads to neonatal respiratory distress syndrome. Loss of type I cells in injury (e.g., ARDS) must be repaired via type II cell differentiation.
Alveolar-Capillary Membrane
The blood-gas barrier consists of (thin to thick sides):
- Flat type I pneumocyte + fused basement membranes + capillary endothelium (thin "gas-exchanging" side)
- A thick side containing the interstitial space (fluid accumulates here first in pulmonary edema before flooding alveoli)
4. Pulmonary Circulation & Lymphatics
The lungs receive a dual blood supply:
Pulmonary Circulation (Gas Exchange)
- Right ventricle → pulmonary artery → right and left branches → pulmonary capillaries → four pulmonary veins → left atrium
- Pulmonary capillaries average ~10 μm in diameter - barely enough for a single red cell to pass
- Pulmonary vessels have thinner walls and less smooth muscle than systemic vessels - hence lower resistance and pressures (normal mPAP ~15 mmHg vs. systemic ~93 mmHg)
Bronchial Circulation (Nutrition)
- Arises from the thoracic aorta and intercostal arteries
- Supplies the walls of the tracheobronchial tree as far as the terminal bronchioles
- Accounts for <4% of cardiac output
- Anastomoses with the pulmonary circulation - contributes to normal venous admixture ("physiological shunt")
Lymphatics
- The lungs have an extensive lymphatic network draining to hilar and mediastinal nodes
- Clinically relevant in pulmonary edema (lymphatics can compensate up to a point before fluid floods the interstitium and alveoli), and in spread of lung carcinoma
5. Respiratory Control - Neuroanatomy
The ventilatory pump is regulated by a distributed neural network:
| Component | Location | Function |
|---|---|---|
| Voluntary control | Parietal cortex → corticospinal tracts | Volitional breathing (speech, breath-holding) |
| Automatic control | Pons (pneumotaxic & apneustic centers) + medulla (pre-Bötzinger complex) | Rhythm and drive to breathe |
| Spinal cord | Reticulospinal tracts → anterior horn cells | Conducts impulses to respiratory muscles |
| Phrenic nerve | C3, C4, C5 ("C3, 4, 5 keeps the diaphragm alive") | Diaphragm innervation |
| Feedback receptors | Peripheral chemoreceptors (carotid/aortic bodies), central chemoreceptors (medulla), lung stretch receptors | Fine-tuning based on PaO₂, PaCO₂, pH, and lung volume |
Clinical point: Cervical spinal cord injuries at or above C3 will paralyze the diaphragm and require mechanical ventilation. Injuries between C3-C5 may allow partial diaphragm function.
6. Key Clinical Correlates
| Anatomical Feature | Clinical Significance |
|---|---|
| Right mainstem bronchus more vertical | Right-sided endobronchial intubation; right-sided aspiration pneumonia |
| Cricoid - narrowest adult airway | Cricoid pressure (Sellick maneuver) to prevent aspiration; narrowest in children is subglottic |
| Diaphragm - phrenic nerve (C3-C5) | High cervical cord injury → respiratory failure |
| Type II pneumocytes produce surfactant | RDS in prematurity; loss in ARDS |
| Pulmonary capillaries ~10 μm | Fat emboli, thromboemboli can obstruct |
| Pleural space is potential space | Pneumothorax, hemothorax, pleural effusion all occur here |
| 23 airway generations | Generations 0-16 = anatomical dead space (~150 mL in adults) |
| Right lung 3 lobes, Left lung 2 lobes | Surgical resections: pneumonectomy, lobectomy, segmentectomy |
Sources:
- Morgan and Mikhail's Clinical Anesthesiology, 7e - Functional Respiratory Anatomy, pp. 910-915
- Murray & Nadel's Textbook of Respiratory Medicine - Functional Anatomy of the Respiratory System, Ch. 130
Clinical physiology of respiratory system
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content across all major physiological topics. Let me compile the full detailed answer.
Clinical Physiology of the Respiratory System
Overview
Respiratory physiology encompasses the mechanics of breathing, gas exchange, lung volumes, ventilation-perfusion relationships, oxygen transport, control of breathing, and the response to pathological states. Each topic has direct clinical implications.
1. Mechanics of Breathing
Inspiration (Active Process)
Muscular contraction causes the diaphragm to descend and ribs to pivot outward, expanding the thoracic cavity. This generates negative intrapleural pressure (drops from -5 to -8 or -9 cm H₂O during inspiration), which lowers alveolar pressure below atmospheric, establishing a gradient that drives airflow inward.
Transpulmonary pressure (P_TP):
P_TP = P_alveolar - P_intrapleural
At end-expiration: P_TP = 0 - (-5) = +5 cm H₂O
Expiration (Passive at Rest)
Elastic recoil of the previously expanded lung parenchyma drives gas out. No muscular work is required during quiet breathing. Active expiration recruits abdominal muscles and internal intercostals.
Clinical point: Normal spontaneous breathing spends more time in exhalation (Te) than inspiration (Ti) because a compliant lung fills quickly. An I:E ratio of 1:2 is the normal baseline.
Minute Ventilation (V̇E)
V̇E = Respiratory Rate × Tidal Volume
Normal = 6-8 L/min at rest.
2. Elastic Properties - Compliance & Surface Tension
Compliance
Compliance (C) = ΔVolume / ΔPressure - the ease of lung distension.
| Component | Normal Value | Notes |
|---|---|---|
| Lung compliance (CL) | 150-200 mL/cm H₂O | Reduced by fibrosis, edema, ARDS |
| Chest wall compliance (CW) | 200 mL/cm H₂O | Reduced by obesity, ascites, supine position |
| Total compliance (lung + chest wall) | ~100 mL/cm H₂O | 1/C_total = 1/CL + 1/CW |
Clinical point: A stiff lung (low compliance) requires greater effort or pressure to achieve the same tidal volume. In ARDS, lung compliance drops dramatically - ventilating these patients with low tidal volumes (6 mL/kg IBW) protects against barotrauma.
Surface Tension & Surfactant
The air-fluid interface in alveoli behaves like a bubble, obeying Laplace's Law:
Pressure = 2 × Surface tension / Radius
Without surfactant, smaller alveoli (higher pressure due to smaller radius) would empty into larger ones - causing alveolar collapse. Surfactant (produced by type II pneumocytes) reduces surface tension in proportion to its concentration:
- As alveoli shrink → surfactant becomes more concentrated → surface tension falls → prevents further collapse
- As alveoli enlarge → surfactant becomes more dilute → surface tension rises → prevents overdistension
This mechanism stabilizes alveolar size and prevents atelectasis.
Clinical point: Surfactant deficiency in premature neonates causes Neonatal Respiratory Distress Syndrome (NRDS). In ARDS, damaged type II cells cannot maintain surfactant, worsening alveolar collapse.
3. Lung Volumes & Capacities
| Parameter | Abbreviation | Normal (Adult) | Definition |
|---|---|---|---|
| Tidal Volume | VT | ~500 mL | Volume per normal breath |
| Inspiratory Reserve Volume | IRV | ~3000 mL | Extra volume above VT |
| Expiratory Reserve Volume | ERV | ~1200 mL | Extra volume exhaled beyond VT |
| Residual Volume | RV | ~1200 mL | Volume remaining after maximal exhalation (cannot be measured by spirometry) |
| Inspiratory Capacity | IC | VT + IRV | Max inspired from FRC |
| Functional Residual Capacity | FRC | ERV + RV (~2400 mL) | Volume at end-expiration at rest |
| Vital Capacity | VC | IRV + VT + ERV (~4600 mL) | Max volume from full expiration to full inspiration |
| Total Lung Capacity | TLC | ~6000 mL | All four volumes combined |
| Forced Expiratory Volume (1 sec) | FEV₁ | >80% of FVC | Key spirometric parameter |
| FEV₁/FVC ratio | - | >0.7 (>70%) | <70% = obstructive defect |
Clinical point: FRC is the lung volume at rest where elastic inward recoil of the lung balances elastic outward recoil of the chest wall. FRC falls in supine position, obesity, pregnancy, and with general anesthesia (by ~15-20%). A reduced FRC below closing capacity (CC) causes small airway closure during tidal breathing, leading to intrapulmonary shunting and hypoxemia.
Obstructive vs. Restrictive Patterns
| Feature | Obstructive (e.g., COPD, Asthma) | Restrictive (e.g., fibrosis, obesity) |
|---|---|---|
| FVC | Normal or ↓ | ↓↓ |
| FEV₁ | ↓↓ | ↓ |
| FEV₁/FVC | <0.7 | Normal or ↑ |
| TLC | ↑ (air trapping) | ↓ |
| RV | ↑ | ↓ |
4. Airway Resistance
Normal total airway resistance: 0.5-2 cm H₂O/L/s
The largest contribution comes from medium-sized bronchi (generation 4-7) - not from large or small airways.
Flow Types
- Laminar flow: Concentric cylinders; governed by Hagen-Poiseuille law (resistance ∝ 1/r⁴); occurs in small airways (<1 mm)
- Turbulent flow: Random movement; resistance ∝ gas density / r⁵; occurs in large airways at high flow rates
Reynolds number predicts flow type:
Re = (velocity × diameter × density) / viscosity
- Re < 1000 → laminar
- Re > 1500 → turbulent
Clinical point: Helium has a lower density-to-viscosity ratio than oxygen. A Heliox (He-O₂) mixture reduces turbulent flow and airway resistance in upper airway obstruction (e.g., croup, subglottic stenosis) - a useful temporizing bridge.
Factors Increasing Airway Resistance
- Bronchospasm (asthma)
- Mucosal edema (anaphylaxis, infection)
- Secretions
- Low lung volume (loss of radial traction on small airways) - corrected by PEEP
5. Ventilation-Perfusion (V̇/Q̇) Relationships
The cornerstone of clinical respiratory physiology.
Normal V̇/Q̇ = 0.8
(Total alveolar ventilation ~4 L/min; total perfusion ~5 L/min)
Gravity-Dependent Zonal Differences (West's Zones)
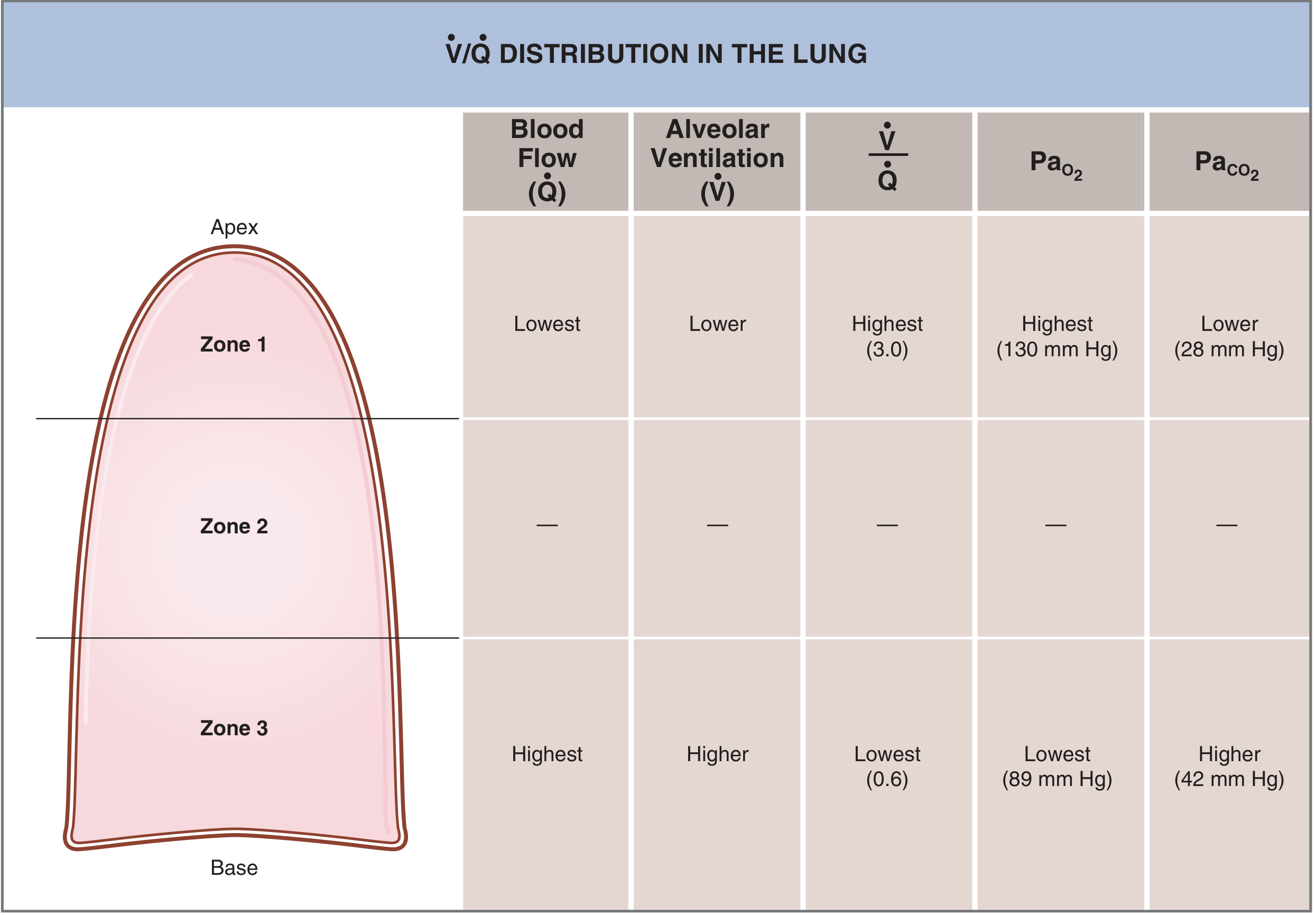
In the upright lung:
| Zone | Location | V̇/Q̇ | PaO₂ | PaCO₂ | Mechanism |
|---|---|---|---|---|---|
| Zone 1 (apex) | Upper | 3.0 (highest) | 130 mmHg | 28 mmHg | Minimal perfusion; relative over-ventilation |
| Zone 2 (mid) | Middle | ~1.0 | - | - | Balanced ventilation and perfusion |
| Zone 3 (base) | Lower | 0.6 (lowest) | 89 mmHg | 42 mmHg | Highest perfusion; relative under-ventilation |
Clinical relevance: Tuberculosis preferentially affects the lung apex (Zone 1 - high V̇/Q̇, high O₂ tension) because M. tuberculosis is an obligate aerobe that thrives in oxygen-rich environments.
V̇/Q̇ Extremes - Spectrum of Defects
| V̇/Q̇ | Condition | Cause | Gas exchange effect |
|---|---|---|---|
| V̇/Q̇ = ∞ | Dead space | No perfusion (PE, shock) | PAO₂ = 150 mmHg; PACO₂ = 0; wasted ventilation |
| V̇/Q̇ high | High V̇/Q̇ | Reduced perfusion | High PO₂, low PCO₂ in capillary blood |
| V̇/Q̇ = 0.8 | Normal | Matched V/Q | Normal gas exchange |
| V̇/Q̇ low | Low V̇/Q̇ | Reduced ventilation (mucus plugging, partial obstruction) | Low PO₂, high PCO₂ in capillary blood |
| V̇/Q̇ = 0 | Shunt | No ventilation (consolidation, atelectasis, R→L cardiac shunt) | PaO₂ = 40 mmHg; PaCO₂ = 46 mmHg (same as mixed venous) |
Key Clinical Distinction: Dead Space vs. Shunt
- Dead space (high V̇/Q̇): hypercapnia dominates; CO₂ rises because it cannot be eliminated. Example: pulmonary embolism
- Shunt (V̇/Q̇ = 0): hypoxemia that is refractory to supplemental O₂ (blood bypasses alveoli entirely). Example: lobar pneumonia, ARDS, ASD with Eisenmenger
Key point: Low V̇/Q̇ (not absolute shunt) can be at least partially corrected by increasing FiO₂. True shunt cannot - this is the clinical basis for the 100% O₂ test.
Venous Admixture (Physiologic Shunt Equation)
$$\frac{\dot{Q}_S}{\dot{Q}_T} = \frac{Cc'O_2 - CaO_2}{Cc'O_2 - C\bar{v}O_2}$$
Where Cc'O₂ = ideal pulmonary end-capillary O₂ content; CaO₂ = arterial O₂ content; CvO₂ = mixed venous O₂ content
Normal shunt fraction = <5%
6. Gas Exchange & the Alveolar Gas Equation
Alveolar Gas Equation
$$P_AO_2 = F_iO_2 \times (P_{atm} - P_{H_2O}) - \frac{P_aCO_2}{R}$$
Where R = respiratory quotient (~0.8); PH₂O = 47 mmHg at 37°C
At sea level breathing room air (FiO₂ = 0.21):
PAO₂ = 0.21 × (760 - 47) - 40/0.8 = ~100 mmHg
Alveolar-Arterial (A-a) Gradient
A-a gradient = PAO₂ - PaO₂
- Normal A-a gradient: 5-15 mmHg in young adults (increases with age and FiO₂)
- Estimated normal: ~(Age/4) + 4 mmHg
Elevated A-a gradient causes of hypoxemia:
- V̇/Q̇ mismatch
- Right-to-left shunt
- Diffusion impairment (rare at rest; occurs with exercise or thickened membrane)
Normal A-a gradient causes of hypoxemia:
- Hypoventilation (PaCO₂ rises, O₂ is displaced from alveoli)
- Low inspired FiO₂ (altitude)
Diffusion
Gas exchange follows Fick's Law of Diffusion:
Volume of gas transferred ∝ (Area × ΔP × Diffusion coefficient) / Thickness
- CO₂ diffuses 20× faster than O₂ despite similar partial pressure gradients
- Therefore, diffusion impairment causes hypoxemia before hypercapnia
- DLCO (diffusing capacity for CO) is the clinical test - reduced in emphysema, ILD, pulmonary hypertension
7. Oxygen Transport
The Oxygen Cascade
PO₂ falls stepwise: Atmosphere (160 mmHg) → Trachea (149 mmHg) → Alveolus (~100 mmHg) → Arterial blood (~95 mmHg) → Tissue (~40 mmHg) → Mitochondria (~5 mmHg)
Oxygen Content of Blood (CaO₂)
CaO₂ = (Hb × 1.34 × SaO₂) + (0.003 × PaO₂)
- Hb-bound O₂ dominates (1.34 mL O₂/g Hb)
- Dissolved O₂ (0.003 × PaO₂) is minor under normal conditions but critical with hyperbaric O₂ therapy
Oxygen-Hemoglobin Dissociation Curve
The sigmoidal shape has major clinical implications:
| Segment | Clinical significance |
|---|---|
| Flat upper portion (PaO₂ >60 mmHg) | SaO₂ stays >90% even with significant drop in PaO₂ - protects against mild hypoxemia |
| Steep lower portion (PaO₂ <60 mmHg) | Small drop in PaO₂ causes large drop in SaO₂ - the "cliff" below which O₂ delivery crashes |
Bohr Effect - Rightward shift (↑ P50, ↓ O₂ affinity, ↑ O₂ unloading at tissues):
- ↑ Temperature, ↑ PCO₂, ↑ [H⁺] (acidosis), ↑ 2,3-DPG
- Physiologically appropriate during exercise (tissues get more O₂)
Leftward shift (↓ P50, ↑ O₂ affinity, ↓ tissue unloading):
- ↓ Temperature, ↓ PCO₂, alkalosis, ↓ 2,3-DPG, fetal Hb (HbF), CO poisoning, methemoglobinemia
Clinical point: Stored blood has low 2,3-DPG, shifting the curve left - massive transfusion patients may have impaired O₂ delivery to tissues despite adequate hemoglobin.
Causes of Hypoxemia - Summary Table
| Mechanism | PaO₂ | PaCO₂ | A-a gradient | Response to O₂ |
|---|---|---|---|---|
| Hypoventilation | ↓ | ↑ | Normal | Good |
| Low FiO₂ (altitude) | ↓ | ↓ | Normal | Good |
| V̇/Q̇ mismatch (low V̇/Q̇) | ↓ | Normal/↑ | ↑ | Partial |
| Shunt (V̇/Q̇ = 0) | ↓↓ | Normal | ↑ | Poor |
| Diffusion impairment | ↓ (exercise) | Normal | ↑ | Good |
8. Control of Breathing
Central Controllers
| Center | Location | Function |
|---|---|---|
| Pre-Bötzinger complex | Medulla | Primary rhythm generator (automatic breathing) |
| Dorsal respiratory group | Medulla | Inspiration timing |
| Ventral respiratory group | Medulla | Expiration and forced breathing |
| Pneumotaxic center | Upper pons | Limits inspiration, promotes rate |
| Apneustic center | Lower pons | Prolongs inspiration |
| Cortex | Parietal lobe | Voluntary breathing (speech, breath-holding) |
Chemoreceptors
Central chemoreceptors (medulla):
- Respond to CO₂/pH in CSF (CO₂ crosses BBB and forms H⁺ + HCO₃⁻)
- Primary driver of ventilatory drive under normal conditions
- Not directly sensitive to O₂
Peripheral chemoreceptors (carotid & aortic bodies):
- Respond to ↓ PaO₂ (primary), ↑ PaCO₂, ↑ [H⁺]
- Carotid bodies are the more important clinical ones (glossopharyngeal nerve, CN IX)
- Drive the hypoxic ventilatory response - activated when PaO₂ falls below ~60 mmHg
Critical clinical point: In COPD patients with chronic hypercapnia, central chemoreceptors become desensitized to CO₂. These patients rely on the hypoxic drive (peripheral chemoreceptors) to maintain ventilation. Giving high-flow O₂ without monitoring can blunt this drive and cause CO₂ narcosis. Target SpO₂ 88-92% in known hypercapnic COPD.
Mechanical Receptors
- Pulmonary stretch receptors (Hering-Breuer reflex): Activated by lung inflation; inhibit further inspiration - prevent over-inflation
- Irritant receptors: Respond to dust, smoke, noxious gases → cough, bronchoconstriction
- J-receptors (juxtacapillary): Stimulated by pulmonary congestion, edema → rapid shallow breathing and dyspnea in heart failure
9. Hypoxic Pulmonary Vasoconstriction (HPV)
A unique property of pulmonary vessels (opposite to systemic circulation):
- Low alveolar PO₂ → local vasoconstriction → diverts blood away from poorly ventilated areas → maintains V̇/Q̇ matching
- Mediators: inhibition of K⁺ channels, membrane depolarization, Ca²⁺ influx in pulmonary arterial smooth muscle
- HPV is inhibited by volatile anesthetic agents (clinically relevant during one-lung ventilation)
Clinical point: In chronic hypoxia (e.g., high altitude, COPD), generalized HPV → global pulmonary hypertension → right ventricular hypertrophy → cor pulmonale.
10. CO₂ Transport
CO₂ is transported in three forms:
| Form | % of Total | Notes |
|---|---|---|
| Bicarbonate (HCO₃⁻) | ~70% | CO₂ + H₂O → H₂CO₃ → H⁺ + HCO₃⁻ (carbonic anhydrase in RBCs); HCO₃⁻ exits RBC in exchange for Cl⁻ (chloride shift) |
| Dissolved CO₂ | ~10% | PaCO₂ = 40 mmHg |
| Carbamino compounds | ~20% | CO₂ bound to Hb and plasma proteins |
Haldane Effect: Deoxygenated Hb binds CO₂ more efficiently than oxygenated Hb - explains why venous blood carries more CO₂ than arterial blood at the same PCO₂.
Clinical Summary: Putting It Together
| Physiological Concept | Clinical Condition | Key Mechanism |
|---|---|---|
| Low compliance | ARDS, fibrosis | High ventilating pressures needed; risk of barotrauma |
| Surfactant loss | NRDS, ARDS | Alveolar collapse, worsened by Laplace |
| Dead space ↑ | Pulmonary embolism | Wasted ventilation, ↑ PaCO₂, ↑ A-a gradient |
| Shunt | Consolidation, atelectasis | Hypoxemia refractory to O₂ |
| Low V̇/Q̇ | COPD, asthma | Partial O₂ response; chronic hypercapnia |
| HPV suppression | Volatile anesthetics | V̇/Q̇ mismatch during one-lung ventilation |
| Loss of hypoxic drive | High-flow O₂ in COPD | CO₂ retention, respiratory acidosis |
| FRC < closing capacity | Supine, obese, elderly | Dynamic airway collapse, shunt, hypoxemia |
Sources:
- Morgan & Mikhail's Clinical Anesthesiology, 7e - Ch. 23: Respiratory Physiology & Anesthesia, pp. 910-960
- Fischer's Mastery of Surgery, 8e - Normal Pulmonary Physiology, p. 264
- Costanzo Physiology, 7th Edition - V/Q Defects and Control of Breathing, pp. 234-240
This is a shared conversation. Sign in to Orris to start your own chat.