APPROCH TO ASCITIC
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ascites" AND "management"
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have thorough material to give a complete, well-illustrated answer. Here is the full approach to ascites:
Approach to Ascites
Ascites is the pathological accumulation of fluid within the peritoneal cavity. It is the most common complication of cirrhosis and carries significant prognostic implications - median survival is ~2 years for non-malignant ascites and only ~4 months for malignant ascites.
1. Pathophysiology
~85% of all ascites cases are due to liver pathology (cirrhosis and portal hypertension).
In cirrhotic patients, collagen deposition causes post-sinusoidal vascular obstruction, raising the hepatic venous portal gradient (HVPG). Ascites develops once HVPG exceeds 10-12 mmHg through two parallel mechanisms:
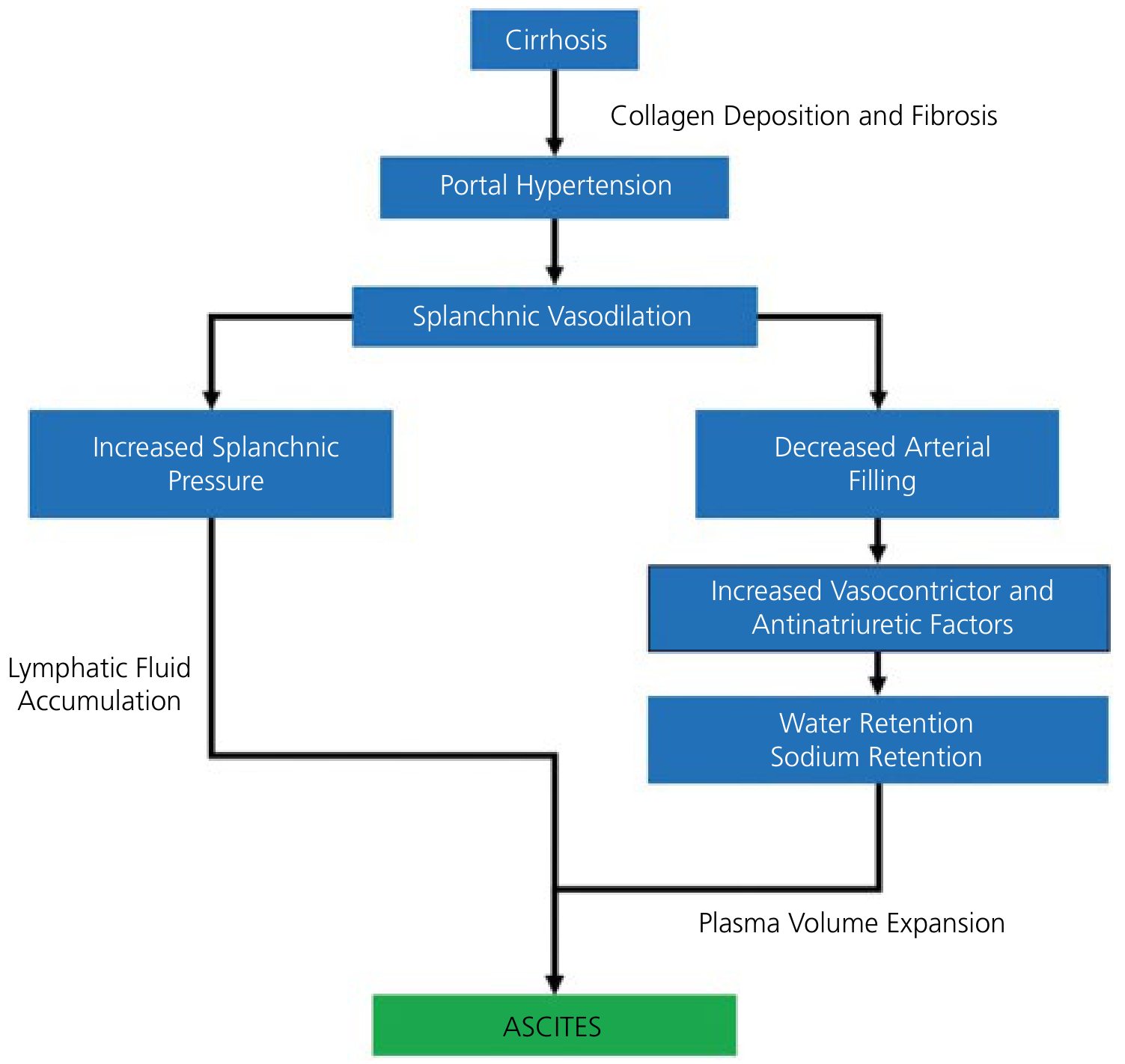
- Splanchnic vasodilation → increased hydrostatic pressure → fluid extravasation into peritoneum; when lymphatic return is overwhelmed, fluid accumulates
- Decreased arterial filling → activation of renin-angiotensin-aldosterone system → renal sodium and water retention → plasma volume expansion → further fluid accumulation
2. Causes of Ascites
Fluid in the peritoneal cavity is classified physiologically by the SAAG (Serum-Ascites Albumin Gradient):
SAAG ≥ 1.1 g/dL (Portal hypertension / Transudates)
| Cause | Notes |
|---|---|
| Cirrhosis | Most common overall cause |
| Alcoholic hepatitis | |
| Congestive heart failure | Light yellow fluid, low protein (<25 g/L) |
| Constrictive pericarditis | Simultaneous pleural effusions (Pick's disease) |
| Budd-Chiari syndrome | Hepatic vein thrombosis |
| Portal vein thrombosis | |
| Obstructive liver metastases | |
| Fatty liver of pregnancy | |
| Myxedema |
SAAG < 1.1 g/dL (Non-portal / Exudates)
| Cause | Notes |
|---|---|
| Peritoneal carcinomatosis | Dark yellow, blood-tinged, protein >25 g/L |
| Nephrotic syndrome | Low oncotic pressure |
| Tuberculous peritonitis | |
| Peritoneal mesothelioma | |
| Chylous ascites | Lymphoma, retroperitoneal tumors |
| Pancreatic ascites | |
| Bile ascites |
Note: Malignancy accounts for only ~10% of ascites; epithelial cancers (colon, gastric, pancreatic, ovary, breast, endometrial) cause 80% of malignant ascites.
Meigs' syndrome = benign ovarian fibroma + ascites + pleural effusion (both resolve with tumor excision).
3. Clinical Presentation
- Symptoms: Abdominal distension, discomfort, early satiety, dyspnea (respiratory compromise when severe)
- Signs:
- Shifting dullness (most reliable clinical sign; requires ~1.5 L of fluid)
- Fluid thrill (massive ascites)
- Bulging flanks
- Stigmata of chronic liver disease: spider nevi, palmar erythema, caput medusae (portosystemic shunt via umbilical vein), gynecomastia, testicular atrophy, Dupuytren's contracture
4. Diagnostic Approach
Step 1: History and Physical Examination
- History of liver disease, alcohol use, malignancy, cardiac disease, TB exposure
- Careful abdominal exam for shifting dullness, fluid thrill, hepatosplenomegaly
Step 2: Abdominal Imaging
CT scan (preferred for etiology, shown below) or ultrasound - detects ascites, liver morphology, portal hypertension features, masses
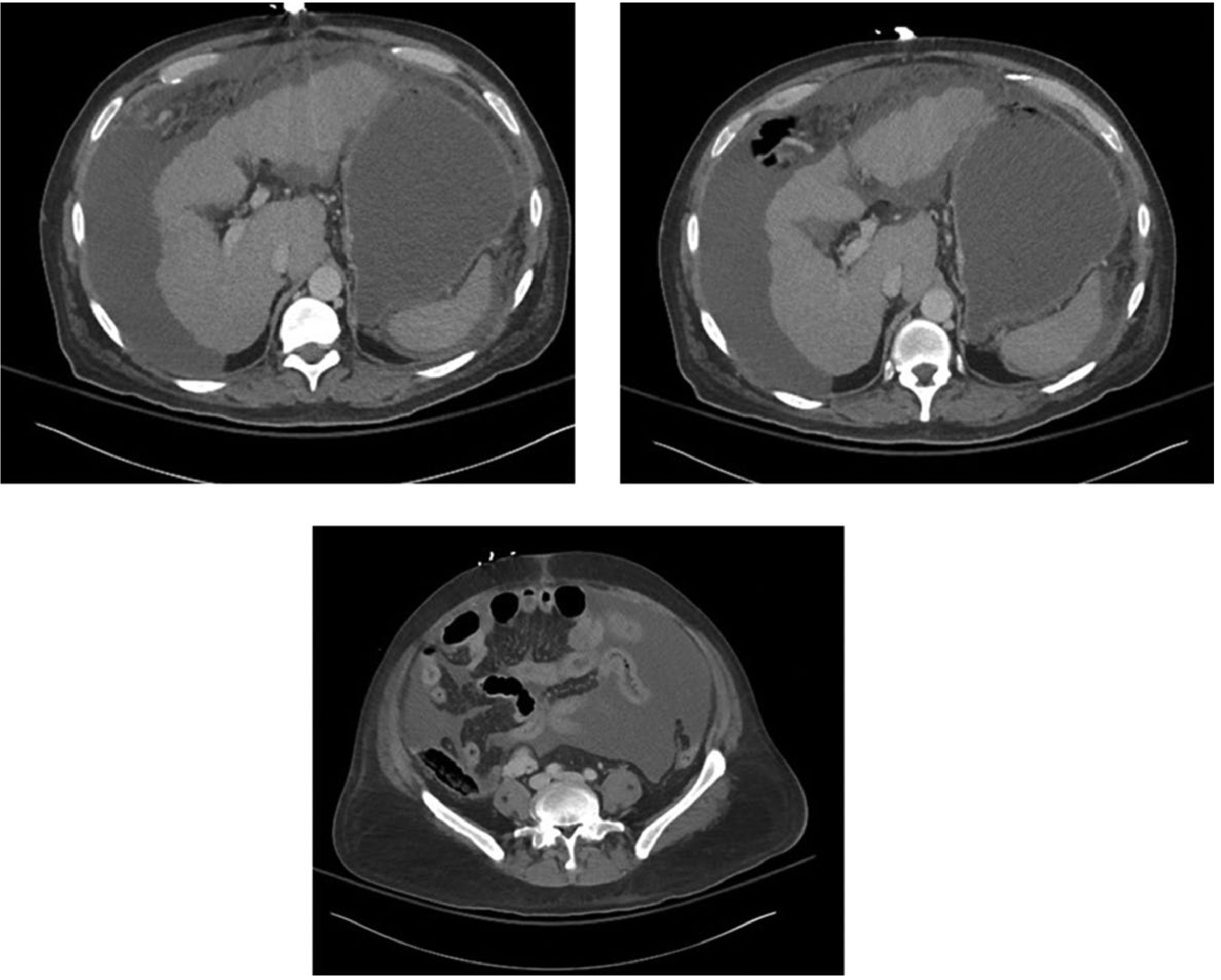
Ultrasound is the most practical bedside tool for detecting ascites and can guide paracentesis.
Step 3: Diagnostic Paracentesis (FIRST investigation in new ascites)
Paracentesis is the most rapid and cost-effective method for determining ascites etiology. It is safe even with mild coagulopathy in cirrhotic patients.
Routine ascitic fluid tests:
| Test | Purpose |
|---|---|
| Cell count with differential | PMN >250/mL = SBP |
| Albumin | For SAAG calculation |
| Total protein | Transudate vs. exudate |
| Gram stain + culture | Infection |
| Glucose | Decreased in infection/malignancy |
| LDH | Elevated in malignancy, secondary peritonitis |
Selective tests (based on clinical suspicion):
| Test | Indication |
|---|---|
| Cytology | Suspected malignancy |
| Triglycerides | Suspected chylous ascites |
| Amylase | Suspected pancreatic ascites |
| Bilirubin | Suspected bile ascites |
| TB culture + PCR | Suspected TB peritonitis |
Step 4: Calculate the SAAG
SAAG = Serum albumin - Ascitic fluid albumin
- SAAG ≥ 1.1 g/dL → Portal hypertension (97% accuracy)
- SAAG < 1.1 g/dL → Non-portal hypertensive cause
This is the single most reliable test for categorizing ascites etiology and has superseded the older transudate/exudate classification.
5. Management
A. Cirrhotic Ascites (Mainstay)
-
Sodium restriction - 2 g/day (2000 mg). More restrictive diets are not recommended as they compromise nutrition.
-
Diuretics:
- Spironolactone (aldosterone antagonist) - start 100 mg/day, increase every 3-4 days up to 400 mg/day maximum. More effective than loop diuretics as first agent.
- Furosemide - start 40 mg/day, increase to 160 mg/day maximum. Add if ascites is tense, weight loss is inadequate, or hyperkalemia develops.
- Target weight loss: 1 kg in week 1, then 2 kg/week
- Do NOT exceed 0.5 kg/day (without peripheral edema) or 1 kg/day (with peripheral edema)
- Avoid ACEIs, ARBs, and NSAIDs (impair renal function and worsen hemodynamics)
-
Albumin infusion:
- Acute infusion alone is of no benefit and risks pulmonary edema
- Long-term albumin (40 g twice weekly × 2 weeks, then 40 g weekly) + spironolactone + furosemide reduces recurrent ascites and improves 18-month survival
B. Refractory Ascites (10-20% of patients)
- Large-volume paracentesis (LVP): Remove all or most fluid
- Give albumin 6-8 g IV per liter removed, especially when >5 L removed, to prevent paracentesis-induced circulatory dysfunction (PICD)
- TIPS (Transjugular Intrahepatic Portosystemic Shunt):
- More effective than LVP + albumin for preventing recurrent ascites
- Associated with higher encephalopathy rate
- PTFE-covered TIPS improves survival in patients requiring LVP >2×/month
- Peritoneovenous shunt: Subcutaneous silicone tube transferring peritoneal fluid to systemic circulation - for patients not candidates for TIPS or transplantation
- Automated flow pump (alfapump): Transfers ascitic fluid to bladder; reduces LVP need and improves QOL; requires surgical placement; risk of infection
- Liver transplantation: Definitive treatment
C. Spontaneous Bacterial Peritonitis (SBP)
- Infection of ascitic fluid without an identifiable surgical source (perforation, abscess, etc.)
- Mechanism: bacterial translocation from gut → mesenteric lymph nodes → bacteremia → ascitic fluid colonization (impaired Kupffer cells due to portosystemic shunting)
- Risk factors: low ascitic fluid complement, reduced immune defenses, intestinal bacterial overgrowth
- Most common organisms: Gram-negative aerobes (E. coli, Klebsiella)
- Clinical features: Fever, abdominal pain, jaundice, tenderness ± rebound; up to one-third are initially asymptomatic and present with encephalopathy, AKI, or sepsis
- Diagnosis: Ascitic fluid PMN count >250 cells/mL on diagnostic paracentesis
- Treatment: Broad-spectrum antibiotics (covering gram-negatives and anaerobes), tailored to culture results; IV albumin reduces risk of hepatorenal syndrome
D. Associated Complications
- Hepatorenal syndrome (HRS): Functional AKI from hemodynamic dysfunction in end-stage liver disease; treated with vasoconstrictors (terlipressin), albumin; indication for transplantation priority
- Hyponatremia: Fluid restrict to 1.5 L/day for serum Na <130 mEq/L; tolvaptan only as bridge to transplantation (risk of hepatotoxicity)
- Hepatic hydrothorax: Ascitic fluid migrates to pleural space (usually right side) via diaphragmatic defects
6. Summary Algorithm
New-onset ascites
↓
History + Exam + Imaging (USS/CT)
↓
Diagnostic paracentesis (all new ascites)
↓
Calculate SAAG
┌──────────────┐
↓ ↓
SAAG ≥1.1 SAAG <1.1
(portal HTN) (non-portal)
↓ ↓
Treat cause Cytology, TB screen,
(cirrhosis, lipids, amylase, etc.
cardiac, etc.)
↓
Cirrhotic ascites:
Na restriction + spironolactone ± furosemide
↓
Refractory → LVP + albumin → TIPS → Transplant
Key Points Summary
| Feature | Detail |
|---|---|
| Most common cause | Cirrhosis (~85%) |
| Key diagnostic test | SAAG (>1.1 portal; <1.1 non-portal) |
| First-line diuretic | Spironolactone (up to 400 mg/day) |
| Add loop diuretic | Furosemide (up to 160 mg/day) |
| Albumin post-LVP | 6-8 g/L removed (mandatory >5 L) |
| SBP diagnosis | PMN >250 cells/mL in ascitic fluid |
| SBP treatment | Broad-spectrum antibiotics + albumin |
| Refractory ascites | LVP ± TIPS ± liver transplant |
| Malignant ascites prognosis | Median survival ~4 months |
Sources: Yamada's Textbook of Gastroenterology 7e; Goldman-Cecil Medicine; Sleisenger & Fordtran's GI and Liver Disease; Rosen's Emergency Medicine; Bailey & Love's Short Practice of Surgery 28e
This is a shared conversation. Sign in to Orris to start your own chat.