ultt for radial nerve and its components
Reading File
search_medical_text
upper limb tension test radial nerve ULTT3
search_medical_text
radial nerve anatomy components superficial radial nerve posterior interosseous nerve
search_medical_image
upper limb tension test radial nerve position
GradeResponse
GradeResponse
GradeResponse
Here is a comprehensive breakdown of the Upper Limb Tension Test for the Radial Nerve (ULTT 2b / ULNT Radial Bias):
Radial Nerve – Relevant Anatomy
The radial nerve (C5–T1) winds around the proximal humerus in the spiral groove, travels down the lateral arm, and divides in the forearm into two main components (Harrison's, p. 12707):
| Component | Type | Territory |
|---|---|---|
| Superficial radial nerve | Purely sensory | Dorsal web space between thumb and index finger; dorsal radial hand |
| Posterior interosseous nerve (PIN) | Purely motor | Wrist/finger extensors, thumb abduction |
The radial nerve proper (proximal to the division) supplies triceps, brachioradialis, and wrist extensors, and gives sensory branches to the posterior arm/forearm.
ULTT for the Radial Nerve (ULTT 2b)
This test selectively loads the radial nerve by combining movements that progressively elongate the nerve's entire course from the cervical spine to the dorsum of the hand.
Sensitizing Sequence (step-by-step)
| Step | Movement | Structure Loaded |
|---|---|---|
| 1 | Shoulder girdle depression | Elongates the brachial plexus proximally |
| 2 | Shoulder abduction (~10°) | Positions the nerve |
| 3 | Shoulder internal rotation | Moves the nerve anteriorly, increasing tension |
| 4 | Elbow extension | Stretches the radial nerve along the lateral arm |
| 5 | Wrist + finger flexion + ulnar deviation | Tensions the superficial radial nerve distally |
| 6 | Thumb flexion into palm | Final distal sensitizer |
The complete end position: patient supine, shoulder depressed and slightly abducted, shoulder internally rotated, elbow extended, forearm pronated, wrist and fingers flexed with ulnar deviation.
Differentiation Between Components
Because the radial nerve has two terminal branches, the position of the wrist/forearm allows some differentiation:
| Variation | Target |
|---|---|
| Wrist flexion + ulnar deviation (standard ULTT 2b) | Superficial radial nerve (sensory) |
| Maintain full pronation + wrist flexion | Posterior interosseous nerve (motor) — resisted supination or pronation can further stress the PIN at the arcade of Frohse |
Sensitizing / Desensitizing Maneuvers
- Contralateral cervical lateral flexion (away from the tested arm) → increases symptom intensity → implicates a neural/cervical component
- Ipsilateral cervical lateral flexion (toward the tested arm) → decreases tension → confirms neural mechanosensitivity
- Shoulder depression can be added or released to differentiate brachial plexus vs. peripheral nerve involvement
Positive Test
- Reproduction of the patient's concordant symptoms (pain, paraesthesia, or numbness along the radial nerve territory — lateral forearm, dorsal thumb/web space)
- Symptoms are altered by cervical side-flexion (sensitized or relieved)
- Asymmetry compared with the contralateral side (>10° range-of-motion difference is clinically meaningful)
Clinical Relevance by Component
| Nerve Segment | Pathology Implicated | Key Symptoms |
|---|---|---|
| Radial nerve proper (spiral groove) | Humeral shaft fracture, "Saturday night palsy" | Wrist drop, weak finger extension, intact triceps |
| Superficial radial nerve | Wartenberg's syndrome (compression by brachioradialis/ECRL) | Dorsal radial hand paraesthesia, no motor loss |
| Posterior interosseous nerve | Entrapment at arcade of Frohse (proximal forearm) | Finger/thumb extension weakness, no wrist drop (ECRL spared), no sensory loss |
ULNT Positions at a Glance
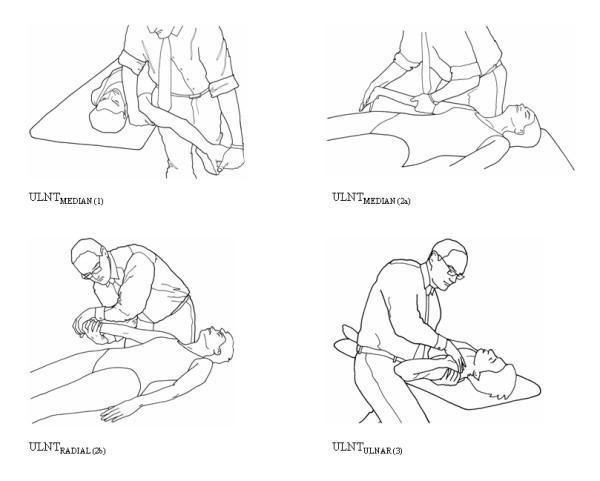
ULNT 2b (Radial) is shown third — note shoulder internal rotation, elbow extension, and wrist/finger flexion.
Key point: ULTT 2b is the standard radial nerve bias test. Differentiating the superficial radial nerve from the PIN requires correlating ULTT findings with motor testing, sensory mapping, and provocation at specific compression sites (Wartenberg's vs. arcade of Frohse).
This is a shared conversation. Sign in to Orris to start your own chat.