Recurrent patella dislocation
Reading File
Finding Sources
Finding Sources
Searching PubMed
"patellar dislocation" AND "recurrent" AND treatment
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative sources. Let me compile a thorough clinical answer.
Recurrent Patellar Dislocation
Definition and Epidemiology
Recurrent patellar dislocation refers to repeated lateral displacement of the patella out of the trochlear groove. It most commonly affects adolescents and young adults engaged in athletic activities. Recurrence after an initial dislocation is reported in 15% to 75% of patients, with risk of recurrence particularly high in the skeletally immature (two thirds of dislocations in younger patients will recur).
- Campbell's Operative Orthopaedics 15th Ed 2026 (Ch. 52)
- Miller's Review of Orthopaedics 9th Edition
Pathomechanics
Patellar instability results from a valgus-producing force, either direct (blow to the medial patella) or indirect (twisting with planted foot). It is inherently multifactorial with a genetic predisposition.
Static stabilizers - MPFL (primary), medial retinaculum
Dynamic stabilizers - Vastus medialis obliquus (VMO)
Bony stabilizers - Trochlear groove (active from ~30° flexion onward)
The MPFL and VMO are the critical stabilizers in 0-20 degrees of flexion. Beyond 30 degrees the patella engages the trochlear groove and bony stability predominates. When patella alta or dysplasia is present, this bony engagement is delayed or absent, predisposing to instability.
With dislocation, the MPFL tears (most commonly at its patellar insertion on MRI) and chondral/osteochondral injury can occur at the medial patellar facet (shear during reduction) and/or the lateral femoral condyle (impaction during dislocation).
Risk Factors for Recurrence
| Factor | Threshold |
|---|---|
| Young age | < 15 years |
| Female sex | - |
| Trochlear dysplasia | Sulcus angle > 145°, depth ≥ 3 mm |
| Patella alta | Insall index > 1.3 |
| Elevated TT-TG distance | > 20 mm (normal 9-13 mm) |
| Ligamentous laxity / hypermobility | - |
| Positive family history | - |
| Femoral anteversion / external tibial torsion | Thigh-foot angle > 30° |
| Genu valgum | - |
The classic triad of highest risk is trochlear dysplasia + patella alta + skeletal immaturity.
- Campbell's Operative Orthopaedics 15th Ed 2026
Trochlear Dysplasia - Dejour Classification
The most important anatomical risk factor. Classified on lateral X-ray by the crossing sign (trochlear groove line crossing the anterior femoral cortex) and on CT/MRI.
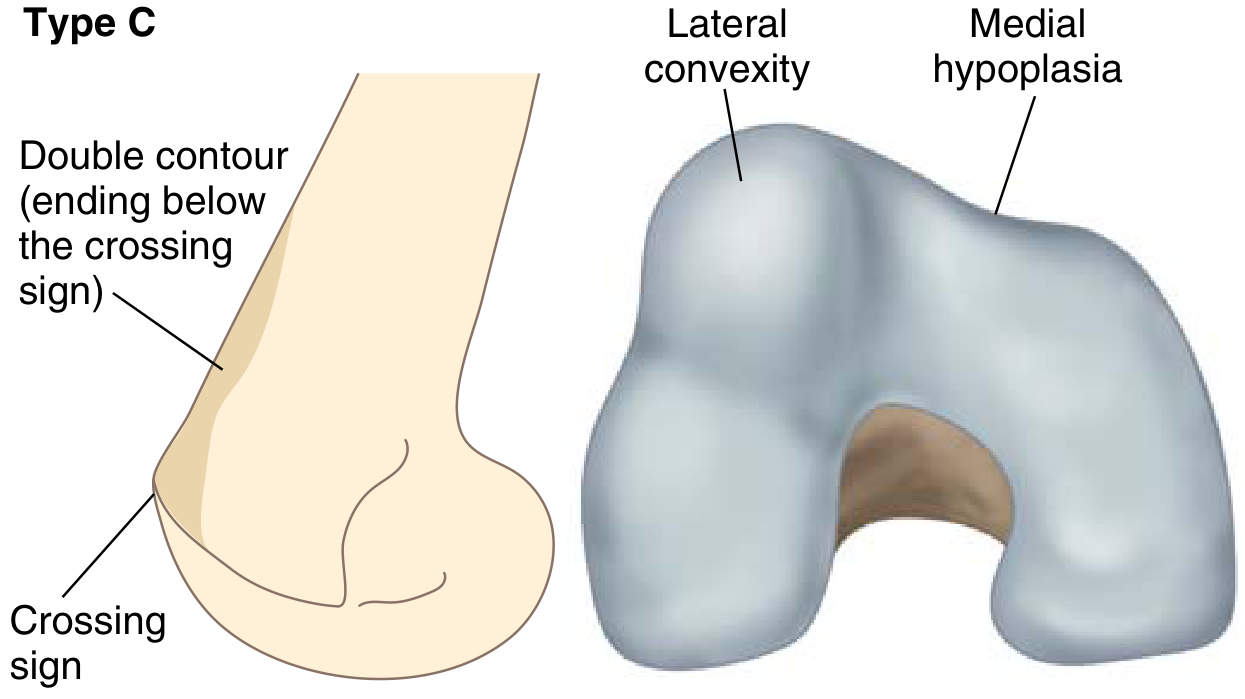
Dejour classification of trochlear dysplasia (from Miller's Review of Orthopaedics)
- Type A: Shallow trochlea (sulcus angle > 145°)
- Type B: Flat or convex trochlea + supratrochlear spur
- Type C: Asymmetric - lateral convexity + medial hypoplasia + double contour sign
- Type D: Combines B + C features (cliff pattern)
Clinical Assessment
History:
- Twisting mechanism or planted-foot rotation
- Audible/palpable "pop" followed by giving way - often confused with ACL injury in young patients
- Spontaneous reduction with knee extension is common
- Ongoing anterior knee pain ± instability
Physical Examination:
- Diffuse peripatellar swelling and tenderness (worse medially - MPFL injury)
- Positive patellar apprehension test (lateral translation at 0-30° flexion)
- J-sign: patella tracks laterally in full extension and reduces abruptly as flexion begins
- Lateral patellar glide > 3 quadrants (incompetent MPFL)
- Assess Q angle (> 20° abnormal), foot progression angle, femoral anteversion
- Quadriceps atrophy (thigh circumference)
- Examine for systemic hypermobility (Beighton score)
Imaging
X-rays (weight-bearing + axial views):
- Lateral view: crossing sign, trochlear bump (supratrochlear spur), patella alta assessment
- Merchant/axial view: sulcus angle (normal ~137°), congruence angle (normal −8°), lateral patellar tilt
- Patellar height indices: Insall-Salvati ratio (>1.2 = alta), Caton-Deschamps index (>1.2 = alta)
CT:
- Gold standard for TT-TG distance (tibial tubercle to trochlear groove distance)
- Normal: 9-13 mm
- 15-20 mm: borderline
-
20 mm: clearly abnormal, associated with instability
- Measures rotational deformities (femoral anteversion, tibial torsion)
MRI:
- Best for MPFL integrity (usually torn at patellar insertion)
- Characteristic "kissing contusion": lateral femoral condyle + medial patella bruising
- Articular cartilage damage assessment
- Can estimate TT-TG (but tends to underestimate vs. CT)
Management
Non-operative (First-line for first-time dislocation)
- Short immobilization (1-3 weeks), then patellar stabilizing brace
- Physiotherapy: VMO strengthening, hip abductor and core strengthening, proprioception training
- Activity modification; weight loss if applicable
- Return to sport: 6-12 weeks when functional milestones are met
- In patients with hypermobile joints, conservative management is the mainstay - surgery outcomes are poor in this group
Indications for Surgery
Urgent/acute:
- Associated osteochondral fracture (loose body)
Elective - strong indications:
- Recurrent instability (multiple events)
- First-time dislocation in high-risk anatomy (trochlear dysplasia + patella alta + young age)
- Contralateral recurrent instability
Surgical Treatment
The treatment framework is guided by the underlying pathoanatomy: containment (bony), alignment, and soft-tissue imbalance.
Treatment Table (Campbell's)
| Pathology | Finding | Procedure |
|---|---|---|
| Patella alta | Insall index > 1.3 | Distalization osteotomy |
| Trochlear dysplasia | Crossing sign, sulcus angle > 145° | MPFL reconstruction ± Trochleoplasty |
| Patellar dysplasia (Wiberg C) | - | MPFL reconstruction |
| Lateral TT displacement | TT-TG > 20 mm | Tibial tubercle anteromedialization |
| Femoral anteversion / genu valgum | Thigh-foot angle > 30° | Rotational osteotomy / epiphysiodesis |
| VMO dysfunction (dynamic) | TT-TG < 20 mm | Rehabilitation |
| Incompetent MPFL / hyperlaxity | Lateral glide 3+ quadrants | MPFL reconstruction |
| Excessive lateral tightness | Lateral tilt on axial views | Lateral release only |
Key Procedures
1. MPFL Reconstruction (Workhorse procedure - "Low risk, high reward")
- Primary procedure for recurrent MPFL deficiency ± trochlear dysplasia
- Graft: gracilis or semitendinosus autograft (or allograft)
- Femoral attachment at the Schottle point (1 mm anterior to posterior cortex line, 2.5 mm distal to posterior medial femoral condyle, proximal to Blumensaat line)
- Tunnel placement errors:
- Too proximal = tight in flexion
- Too distal = loose in flexion
- Key complication: medial patellar instability or medial facet OA from overtightening
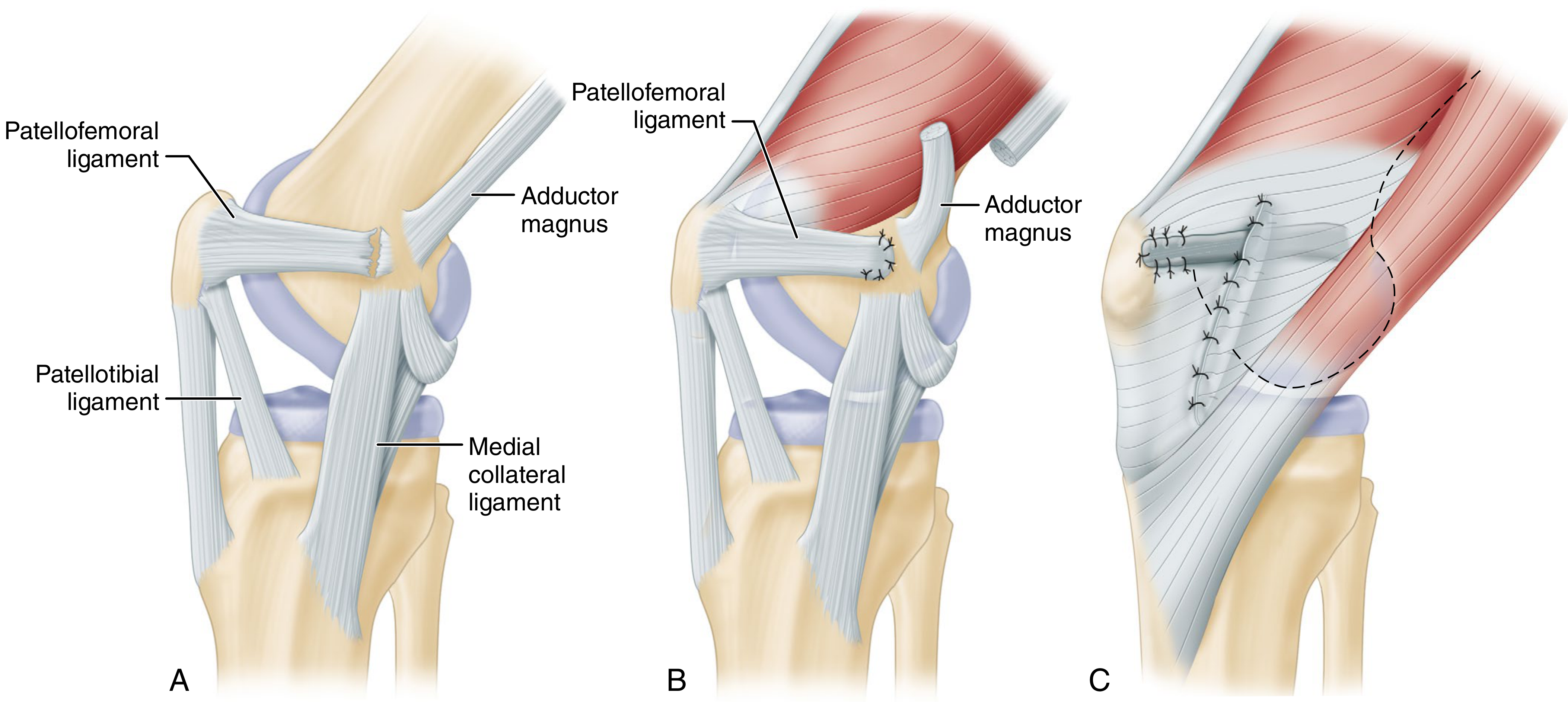
MPFL: A - anatomy showing patellofemoral and patellotibial ligaments. B - ligament reattachment. C - retinaculum duplication after reconstruction. (Campbell's 15th Ed)
2. Tibial Tubercle Anteromedialization (Fulkerson / Elmslie-Trillat)
- Indicated when TT-TG > 20 mm (or > 15 mm with trochlear dysplasia)
- Elmslie-Trillat: pure medialization - quicker healing, lower fracture risk
- Fulkerson: oblique osteotomy providing anteromedialization (30° = 1 mm anterior per 2 mm medial; 45° = 1:1 ratio)
- Best for lateral/distal facet chondral damage
- Contraindicated for proximal/medial facet arthritis
- Often combined with MPFL reconstruction
3. Trochleoplasty ("High risk, high reward")
- Indicated for severe trochlear dysplasia (convex/flat trochlea) unresponsive to other procedures
- Low recurrence rate but significant risk: osteonecrosis, arthrofibrosis, progressive DJD of lateral facet
4. 3-in-1 Procedure (Oliva) - for open physes / skeletally immature
- Lateral release + VMO advancement + transfer of medial third of patellar tendon to MCL
- Used when tibial tubercle transfer is unsafe (open physes)
- Steps: lateral retinacular release → mobilization of VMO insertion → medial 1/3 patellar tendon detached distally, transferred medially and fixed with suture anchors at 45° → VMO advanced 10 mm distally
5. Lateral Release - indicated ONLY for excessive lateral pressure syndrome
- Not indicated as isolated treatment for patellar instability
- May actually increase risk of both medial and lateral subluxation if used in isolation
Special Considerations
Pediatric / Open Physes
- Tibial tubercle osteotomy is contraindicated (physeal injury risk)
- MPFL reconstruction must avoid the physis
- 3-in-1 soft-tissue procedure or MQTFL (medial quadriceps tendon-femoral ligament) reconstruction preferred
- Epiphysiodesis for angular deformities
Hypermobility Syndromes
- Patellar instability in hypermobile joints is primarily managed conservatively
- Joint hypermobility is a poor prognostic indicator for operative outcomes
- Surgery should not be the mainstay of treatment in this group
"Miserable Malalignment Syndrome"
- Combination of femoral anteversion + genu valgum + external tibial torsion + pronated feet
- Exacerbates patellar instability in adolescents
- May require rotational osteotomy in severe cases
Complications of Recurrent Dislocation
- Articular cartilage damage (medial patellar facet - most common site)
- Osteochondral fractures and loose bodies
- Progressive patellofemoral osteoarthritis
- Ongoing anterior knee pain
- Quadriceps inhibition and muscle atrophy
Recent Evidence (2024-2026)
A 2024 systematic review (PMID 39260775) confirmed that distal femoral osteotomies improve recurrent patellar instability in patients with genu valgum, supporting the role of addressing coronal plane deformity.
A 2025 systematic review (PMID 40744396) found that females experience higher rates of recurrent dislocation following MPFL reconstruction, highlighting the need for careful patient selection and potentially addressing additional anatomic risk factors (trochlear dysplasia, patella alta) in female patients rather than isolated MPFL reconstruction.
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 (Ch. 38 & 52); Miller's Review of Orthopaedics 9th Ed; Rheumatology 2-Volume Set 2022 (Elsevier)
Ctev
Finding Sources
Finding Sources
Searching PubMed
"clubfoot" AND "Ponseti" AND treatment
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
I now have comprehensive information. Let me compile the full answer.
Congenital Talipes Equinovarus (CTEV / Clubfoot)
Definition
CTEV is a complex congenital foot deformity present at birth characterized by four components summarized by the mnemonic CAVE:
| Component | Description |
|---|---|
| C - Cavus | High arch (plantar flexion of forefoot on hindfoot) |
| A - Adductus | Forefoot adduction (medial deviation) |
| V - Varus | Hindfoot varus (inversion) |
| E - Equinus | Plantarflexion deformity at ankle |
The deformity is corrected in exactly this CAVE order during treatment.
Epidemiology
- Incidence: ~1 in 1,000 live births
- Boys affected twice as often as girls
- 50% of cases are bilateral
- Most common serious congenital foot anomaly
Pathoanatomy
The primary structural abnormality is talar neck deformity - medial and plantar deviation of the talar neck, with secondary:
- Medial rotation of the calcaneus under the talus
- Medial displacement of the navicular (onto the medial aspect of the talar head)
- Medial displacement of the cuboid
- Shortening/contracture of: Achilles tendon, tibialis posterior, FHL, FDL, intrinsic muscles, joint capsules, ligaments, and plantar fascia
The anterior tibial artery is often absent or diminutive - this is an important surgical consideration (dorsalis pedis may be insufficient as sole blood supply).
Etiology
| Type | Details |
|---|---|
| Idiopathic (majority) | Genetic predisposition via PITX1-TBX4 transcriptional pathway |
| Neurogenic | Myelomeningocele (30-50% of MMC patients have clubfoot), spinal cord anomalies |
| Syndromic | Arthrogryposis, diastrophic dwarfism, prune-belly syndrome, tibial hemimelia |
| Constriction band | Streeter dysplasia |
Syndromic and neurogenic clubfeet are more rigid, have higher recurrence rates, and respond less well to conservative management than idiopathic forms.
Clinical Assessment
History
- Visible foot deformity at birth
- Family history (genetic predisposition)
- Prenatal diagnosis often possible on USS (~ 20 weeks)
Examination
- Rigid vs. positional (postural) clubfoot - distinguish by gentle manipulation
- Check for associated spine (MMC), hip dysplasia
- Assess skin creases: deep medial and posterior creases indicate severity
- In older/untreated: weight-bearing on dorsolateral foot, callosities, short leg, calf atrophy
Severity Scoring
Pirani Score (0-6, most widely used)
Six clinical signs, each scored 0 (normal), 0.5 (moderate), or 1 (severe):
Midfoot signs (0-3):
- Curved lateral border
- Medial crease
- Lateral talar head coverage
Hindfoot signs (0-3):
4. Posterior crease
5. Rigid equinus
6. Empty heel
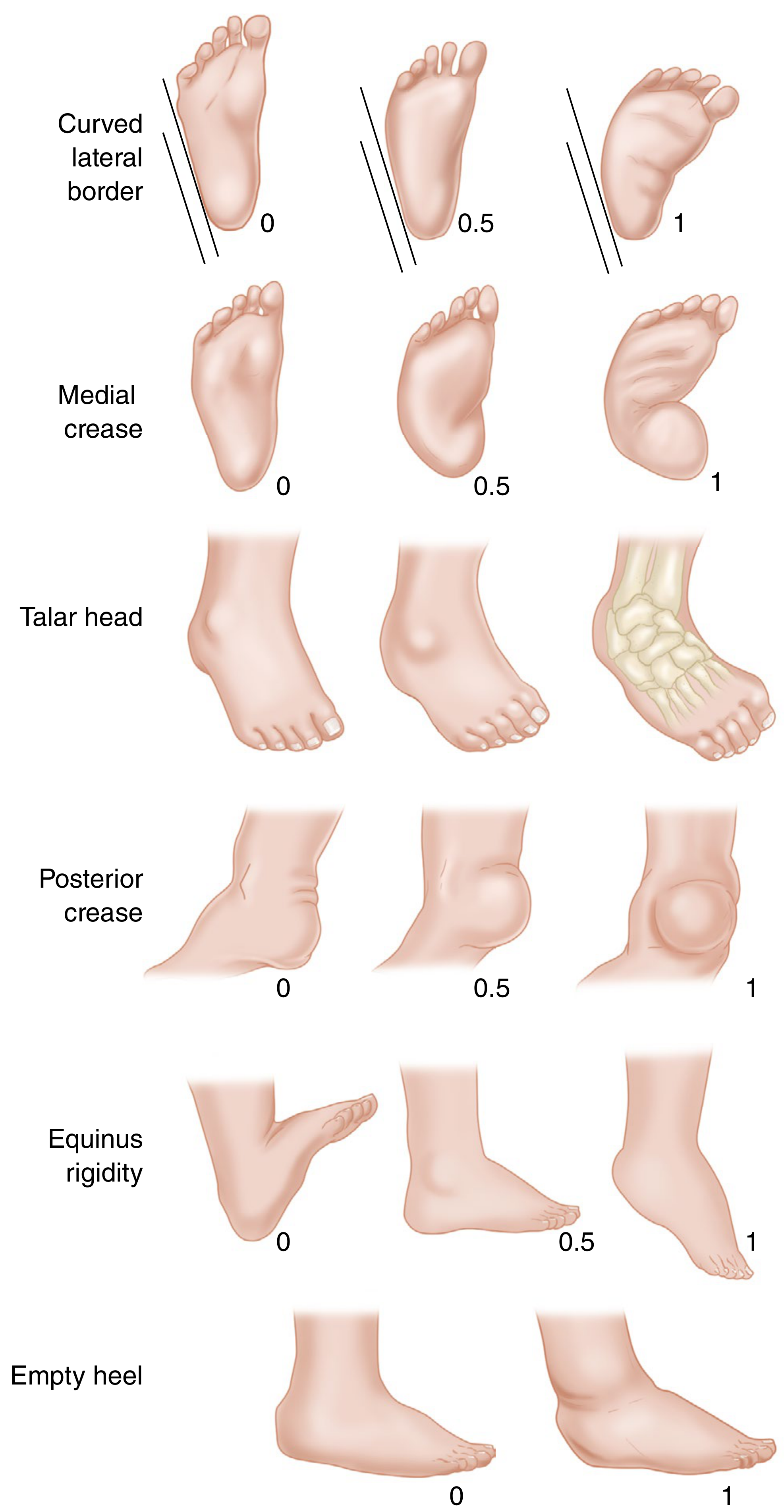
Pirani classification - Campbell's Operative Orthopaedics 15th Ed
Dimeglio Classification (0-20)
- Grade I (Benign): 0-5 pts
- Grade II (Moderate): 6-10 pts
- Grade III (Severe): 11-15 pts
- Grade IV (Very Severe): 16-20 pts
Both Pirani and Dimeglio scores correlate with the number of Ponseti casts required.
Radiographic Features
Minimal ossification in the neonate makes X-rays less useful in early infancy. When obtained:
- AP view (Kite angle - talocalcaneal angle): Normal 20-40°; reduced (<20°) in CTEV due to parallelism of talus and calcaneus
- Lateral/Turco view (dorsiflexion lateral): Talocalcaneal angle < 35° (normal)
- Talus-1st metatarsal angle (AP): Negative in CTEV (normally 0-20°)
- Key radiographic sign: "Parallelism" - talus and calcaneus axes run parallel rather than diverging
Treatment
Treatment begins as early as possible - ideally within the first 2-4 weeks of life.
1. Ponseti Method (Gold Standard - First-line)
Principles:
- Serial weekly gentle manipulation and long-leg plaster casting
- Corrects deformities in the CAVE sequence
- Uses the lateral talar head as a fulcrum for adduction/varus correction
- Supinates forefoot (do NOT pronate - creates rocker-bottom)
Casting sequence:
| Cast No. | Correction Achieved |
|---|---|
| 1st cast | Corrects cavus - supinate forefoot, dorsiflex 1st ray |
| 2nd-4th casts | Correct adductus and varus - lateral pressure on distal talar head as fulcrum, abduct forefoot |
| 5th-6th cast | Correct equinus - dorsiflexion (after tenotomy) |
- Total: typically 5-6 casts required
- Final cast placed in 70° of abduction
- >90% success in children under 2 years, even after previous unsuccessful treatment
Percutaneous Achilles Tenotomy:
- Required in ~90% of patients to fully correct equinus
- Done under local anesthesia (office/clinic) before final cast application
- Prevents rocker-bottom deformity (do not dorsiflex through midfoot before varus corrected)
- Cast then worn for 3 more weeks post-tenotomy
Maintenance Phase - Foot Abduction Brace (Denis Browne / FAB):
- Mandatory - most important factor in preventing recurrence
- Full-time for 3 months, then during sleep and naps for 3-4 years
- Brace: shoes set at 60-70° abduction bilaterally (40° for unilateral)
- Recurrence is most strongly associated with brace non-compliance
Recurrence rates: 10-30%; most recurrences can be retreated with recasting ± Achilles tenotomy
Modifications showing equivalent results:
- Accelerated biweekly casting (faster correction)
- Fiberglass casting = plaster results
- Bracing to age 4 may be superior to stopping at age 3
2. Anterior Tibial Tendon Transfer (ATTT)
- Indicated for dynamic supination deformity (residual or recurrent varus driven by anterior tibialis over-activity)
- Transfer of the anterior tibial tendon from its lateral cuneiform insertion to the middle/lateral cuneiform or cuboid
- Usually combined with recasting
- Typically performed at age 2.5-4 years (when child begins walking consistently)
3. Operative Treatment
Reserved for resistant/refractory clubfeet (~5% of idiopathic cases) or older children at presentation.
Posteromedial Release (PMR) - Turco / Cincinnati approach
- Tendon lengthening (Achilles, tibialis posterior, FHL, FDL) + capsulotomy (subtalar, tibiotalar, talonavicular joints) + realignment
- Posterior tibial artery must be carefully protected (anterior tibial artery often absent)
- Typically performed at 6-12 months
- Now largely replaced by Ponseti method; reserved for true failures
For Older Children (3-10 years) with Residual Deformity:
- Medial opening-wedge osteotomy or lateral column shortening (cuboid decancellation/cuneiform osteotomy) - for residual adductus
- Calcaneal osteotomy - for residual varus/valgus
For Late-Presenting / Severe Neglected Clubfoot:
- Triple arthrodesis (subtalar + talonavicular + calcaneocuboid) - for children presenting late (adolescence/adults)
- Contraindicated in insensate feet (risk of ulceration from rigidity)
- Talectomy - salvage for severely deformed rigid clubfoot in older child
- Complete talus removal required (any remnant regrows and causes recurrence)
- Achilles tendon may also need resection after talectomy
- Ilizarov frame - for complex recurrent/neglected deformities
Complications
| Complication | Cause |
|---|---|
| Recurrence | Most common; primarily from brace non-compliance |
| Rocker-bottom deformity | Dorsiflexion through midfoot before varus corrected |
| Flat-top talus | Aggressive dorsiflexion causing talar dome flattening |
| Overcorrection | Excessive lateral column procedures |
| Dorsal bunion | After clubfoot surgery; from strong tibialis anterior + FHB/abductor hallucis imbalance |
| Vascular injury | PMR - anterior tibial artery often absent |
| Wound dehiscence | Posterior skin under tension (especially in MMC clubfeet) |
| Avascular necrosis of talus | Extensive surgical dissection |
Special Populations
Myelomeningocele-associated Clubfoot
- 30-50% of MMC children affected; deformity is more rigid, resembles arthrogryposis
- Ponseti method still first-line but: 68% early relapse, 33% require surgical release, 10% no improvement
- Surgery: radical posteromedial-lateral release via Cincinnati incision at 10-12 months
- Active anterior tibial tendon should be tenotomized to prevent recurrent supination
- Insensate feet are a contraindication to triple arthrodesis
Arthrogryposis
- Very rigid; requires more aggressive casting and higher surgical rates
Recent Evidence (2024-2026)
- A 2024 network meta-analysis (PMID 38015923) in JBJS confirmed Ponseti casting as the optimal treatment for idiopathic clubfoot across outcomes compared to other methods.
- A 2026 systematic review (PMID 40888800) found fiberglass and plaster casts produce equivalent outcomes in the Ponseti method, supporting use of either material.
- A 2024 systematic review (PMID 39365806) confirmed Ponseti method is effective even in myelodysplastic clubfeet, though with higher recurrence.
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 (Ch. 31 & 36); Miller's Review of Orthopaedics 9th Edition; Schwartz's Principles of Surgery 11th Ed
Acl reconstruction
Finding Sources
Searching PubMed
"anterior cruciate ligament reconstruction" AND graft
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I have a very comprehensive picture. Let me now compile the full answer.
ACL Reconstruction
Background
Primary repair of mid-substance ACL tears routinely fails (myofibroblasts coat the torn ends, preventing primary healing). Reconstruction - replacing the ACL with a graft - is therefore the standard for patients who want to return to pivoting/cutting sports.
Goals of surgery:
- Restore normal knee kinematics (anterior translation + rotation)
- Return patient to full activity
- Prevent secondary meniscal/chondral injury and progressive arthrosis
Indications for Reconstruction
- Young, active patients wishing to return to pivoting/cutting sports
- Acute ACL tear with concomitant repairable meniscal tear
- Chronic ACL insufficiency with functional instability
- First-time dislocation with osteochondral fracture (relative)
- Pediatric patients (special considerations apply - physeal-sparing techniques)
Timing: Early reconstruction is preferred for return to sport and decreased risk of secondary injury. However, full ROM must be achieved before surgery to minimize arthrofibrosis risk - reconstruction in the acute inflammatory phase increases stiffness risk significantly.
Graft Selection
Biomechanical Strength Comparison (Ultimate Load to Failure)
| Graft | Strength (N) | Stiffness (N/mm) |
|---|---|---|
| Native ACL | 2160 | 242 |
| Central 1/3 patellar tendon (BPTB) | 2977 | 455 |
| Quadruple hamstring (ST+G) | 4140 | 807 |
| Quadriceps tendon | 2353 | 326 |
| Native PCL | 1867 | - |
- Campbell's Operative Orthopaedics 15th Ed 2026, Table 56.2
1. Bone-Patellar Tendon-Bone (BPTB) Autograft
Advantages:
- Bone-to-bone healing (fastest incorporation - ~6 weeks)
- High strength and stiffness
- Lower retear rate in young athletes
- More likely to achieve: normal Lachman, normal pivot shift, KT-1000 side-to-side difference < 3 mm
Disadvantages:
- Anterior knee pain (kneeling pain - "kneeler's pain")
- Patellar tendinitis
- Patellar fracture risk (especially if graft too deep)
- Greater risk of extension loss
- Higher patellofemoral pain
- Some studies show higher arthritis risk at 5-7 years vs. hamstring
2. Four-Strand Hamstring (Semitendinosus ± Gracilis) Autograft
Advantages:
- Highest biomechanical strength (quadrupled)
- Less anterior knee pain/kneeling pain
- Less extension loss
- Lower patellofemoral crepitance
Disadvantages:
- Graft creep/relaxation over time (more than ligamentous grafts)
- Slower soft-tissue tunnel incorporation (2-3 weeks longer than bone plug)
- Hamstring weakness (~20% loss of knee flexion/internal rotation strength)
- Saphenous nerve branch injury risk
- Must be ≥ 8 mm diameter - smaller grafts have significantly higher revision rates (0.82× lower revision risk per 0.5 mm increase from 7-9 mm)
3. Quadriceps Tendon Autograft
- Growing in popularity, especially with bone plug from patella
- Strength intermediate between BPTB and hamstring
- Avoids anterior knee pain of BPTB while providing bone-to-bone fixation option
- Patellar fracture risk similar to BPTB
4. Allograft
Advantages: Less donor morbidity, better cosmesis, shorter operative time, preserves extensor mechanism
Disadvantages:
- Failure rates 2-5 times higher than autograft in young/active patients
- Slower incorporation into bone tunnels
- Not recommended in young patients (age < 34 years)
- Acceptable in older/lower-demand patients (no difference in retear > age 34)
- Infection risk: Clostridium, hepatitis, HIV (1:1.5-6 million)
- Chemically processed/irradiated allografts have higher failure rates than fresh-frozen
Bottom line: BPTB and hamstring autografts produce equivalent long-term outcomes (laxity, ROM, subjective scores, OA rates at 10-17 years). BPTB may have slightly lower early retear; hamstring has less anterior knee pain.
Surgical Technique
Tunnel Placement - The Critical Variable
Femoral tunnel:
- Anatomic reconstruction targets the center of the femoral ACL footprint (10- or 2-o'clock position, or "low and deep" on the posterior condyle)
- Achieved via independent femoral drilling (outside-in or accessory medial portal) rather than transtibial technique
- More horizontal graft position reduces rotational instability
- Single-bundle vs. double-bundle: currently no difference in patient-reported outcomes
Tibial tunnel:
- Aim: center of the tibial ACL footprint (lateral to PCL, anterior to posterior horn of lateral meniscus)
- Angle: typically 55-65° to the tibial plateau
Fixation Methods
- Bone-to-bone (BPTB): Interference screws - provide excellent fixation if properly placed
- Soft-tissue grafts (hamstring): Interference screws (BioScrew) + tunnel compaction + secondary fixation (cortical buttons, cross-pins)
- Bone plug incorporation: ~6 weeks; soft-tissue graft incorporation: 8-12 weeks
- Tunnel widening: aperture widening occurs up to 6 weeks, then narrows by 12 weeks
Anterolateral Ligament (ALL) Reconstruction - Augmentation
- Indicated for high-risk patients: 3+ pivot shift, hyperextension > 5°, high-demand athletes
- ACL + ALL reconstruction reduces failure rate to < 3%, which is:
- 2.5× lower than isolated BPTB
- 3.1× lower than isolated hamstring reconstruction
- Medial meniscal repair failure also 2× lower with combined reconstruction
- Technique: gracilis autograft fixed 8 mm proximal and 4.3 mm posterior to lateral epicondyle (femur), and 22 mm posterior to Gerdy's tubercle (tibia)
Physeal-Sparing Techniques (Pediatric)
- All-epiphyseal or combined physeal-sparing techniques to avoid growth disturbance
- Soft-tissue fixation preferred over bone plugs crossing physis
- MQTFL/MPFL-type reconstruction approaches used in some cases
Complications
Tunnel Malposition (Most Common Technical Error)
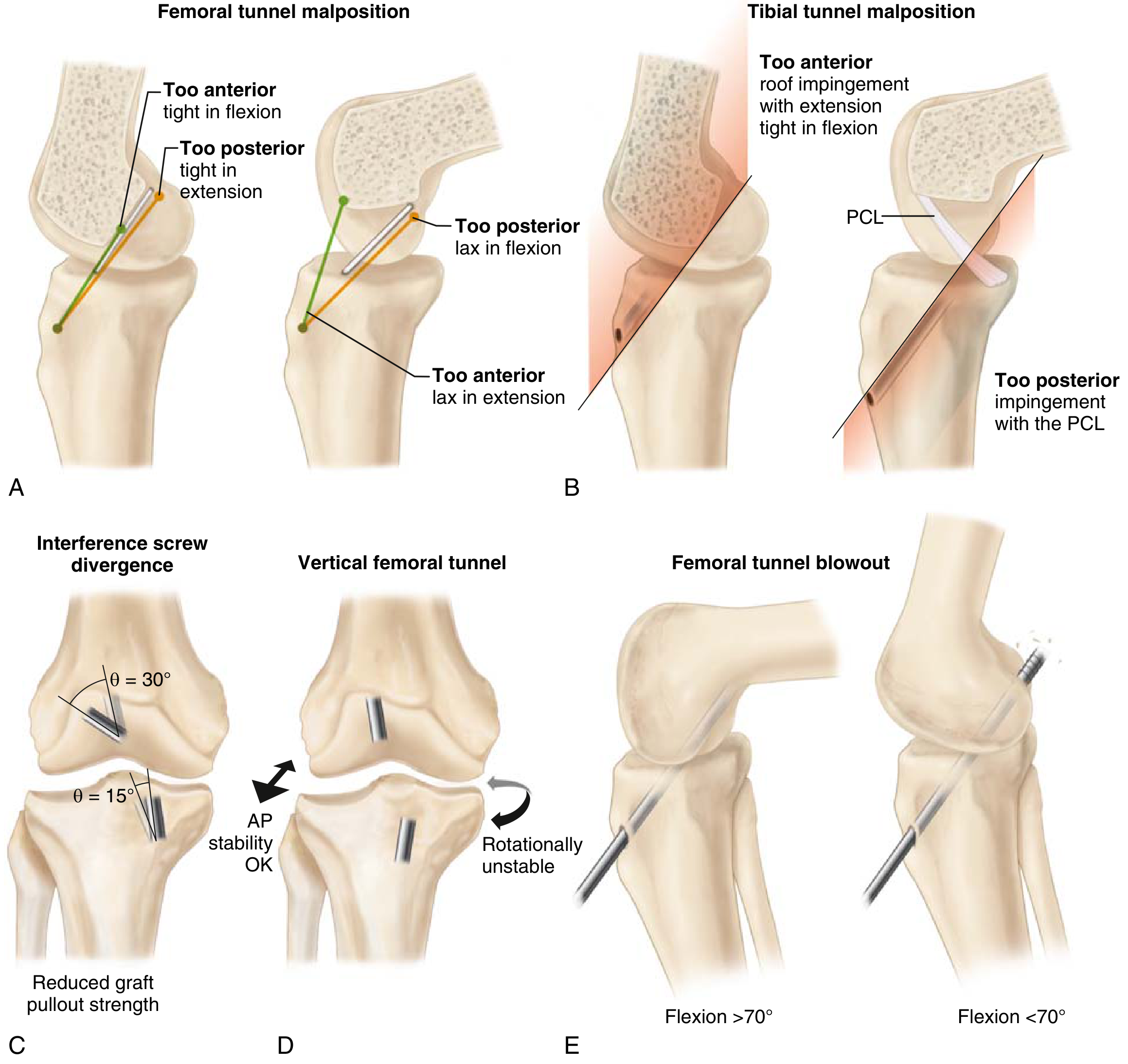
Common complications of ACL reconstruction - Miller's Review of Orthopaedics 9th Ed
| Error | Consequence |
|---|---|
| Femoral tunnel too anterior | Tight in flexion → flexion loss |
| Femoral tunnel too posterior | Lax in extension → instability |
| Tibial tunnel too anterior | Roof impingement with extension, tight in flexion |
| Tibial tunnel too posterior | PCL impingement |
| Vertical graft | AP stability preserved but rotationally unstable (pivot shift not corrected) |
| Femoral tunnel blowout | Risk at flexion < 70° if drilling with knee insufficiently flexed |
Interference Screw Errors
- Femoral divergence > 30°: reduced pullout strength
- Tibial divergence > 15°: reduced pullout strength
Other Complications
| Complication | Key Points |
|---|---|
| Arthrofibrosis | Most common overall complication; risk minimized by achieving full ROM before surgery; avoid reconstruction in acute phase |
| Graft failure/retear | Technical (tunnel malposition, vertical graft), biological (poor incorporation), patient factors (young age, early return to sport) |
| Infection | Irrigation + debridement with graft retention successful in ~85% of cases |
| Patellar fracture | BPTB harvest; avoided with careful technique |
| Saphenous nerve injury | Hamstring harvest |
| Donor site pain | BPTB: anterior knee/kneeling pain; hamstring: flexion weakness |
| OA progression | Radiographic OA appears in > 50% of patients 10-20 years post-reconstruction; ACL reconstruction does NOT reduce OA risk |
Rehabilitation
Key Principles
| Phase | Focus |
|---|---|
| Immediate | Early knee extension (heel elevated), immediate partial weight bearing with crutches, cold therapy |
| Early (0-6 weeks) | Full ROM - emphasis on extension; avoid open chain extension (OKC) which stresses graft especially near full extension |
| Strengthening | Closed chain exercises preferred (lower patellofemoral pain, better KT-1000 scores, higher satisfaction); hamstring-dominant exercises early |
| Proprioception | Begin within first 2 weeks; combine with strength training |
| Bracing | Postoperative bracing NOT proven beneficial except in downhill skiers |
Return to Sport Criteria
- Minimum 6 months after surgery (animal studies suggest 6-12 months for graft maturation)
- ≥ 80% quadriceps strength symmetry vs. contralateral limb
- Early return to high-level sport is a significant risk factor for ACL reconstruction failure
- Prehabilitation (pre-operative rehab) improves short- and long-term outcomes
Blood Flow Restriction (BFR) Training
- Air tourniquet proximally during therapy
- Low-intensity exercise with vascular occlusion promotes muscle hypertrophy
- Attenuates quadriceps atrophy post-operatively
Exercise Guidance
- Avoid: Open kinetic chain (OKC) extension in last degrees of extension, especially in first 6 weeks
- Prefer: Closed kinetic chain (CKC) exercises (squats, leg press, cycling)
- CPM machines: not routinely recommended (no proven benefit)
- No difference between accelerated and standard rehabilitation programs
Results
| Metric | Data |
|---|---|
| Stability restoration | 90-95% achieve KT-1000 side-to-side difference ≤ 3 mm |
| OA at 10-20 years | > 50% develop radiographic OA (reconstruction does not prevent this) |
| Young age | Independent risk factor for reconstruction failure |
| Pivot shift preop 3+ | Significantly increases failure rate |
Revision ACL Reconstruction
Causes of graft failure to consider:
- Technical: tunnel malposition (most common), vertical graft placement, poor fixation
- Missed concomitant injuries: posterolateral corner, MCL, ALL
- Alignment: varus alignment or excessive posterior tibial slope increases graft stress
- Biological: poor graft incorporation
- Patient factors: young age, early return to sport, hyperextension laxity > 5°
Workup: prior operative notes, CT for tunnel assessment, full-length alignment films.
Recent Evidence (2023-2026)
- A 2025 systematic review/meta-analysis (PMID 39836368) comparing BPTB vs. hamstring autograft found no significant difference in return to sport or graft failure rates, supporting equipoise in graft selection.
- A 2023 meta-analysis (PMID 36189967) identified young age, hamstring graft, and small graft diameter as risk factors for revision/rerupture.
- A 2025 systematic review (PMID 40276858) confirmed prehabilitation before ACL reconstruction is safe and provides short- and long-term benefits.
Sources: Campbell's Operative Orthopaedics 15th Ed 2026 (Ch. 50 & 56); Miller's Review of Orthopaedics 9th Edition; Rockwood and Green's Fractures 10th Ed 2025
This is a shared conversation. Sign in to Orris to start your own chat.