DNS from dhingra
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Excellent - both images retrieved. Now I have all the content needed for a comprehensive DNS answer in Dhingra style. Here is the complete write-up:
Deviated Nasal Septum (DNS)
Definition
Deviated nasal septum is a displacement of the nasal septum from the midline, causing partial or complete obstruction of one or both nasal passages. It is one of the most common causes of unilateral nasal airway obstruction.
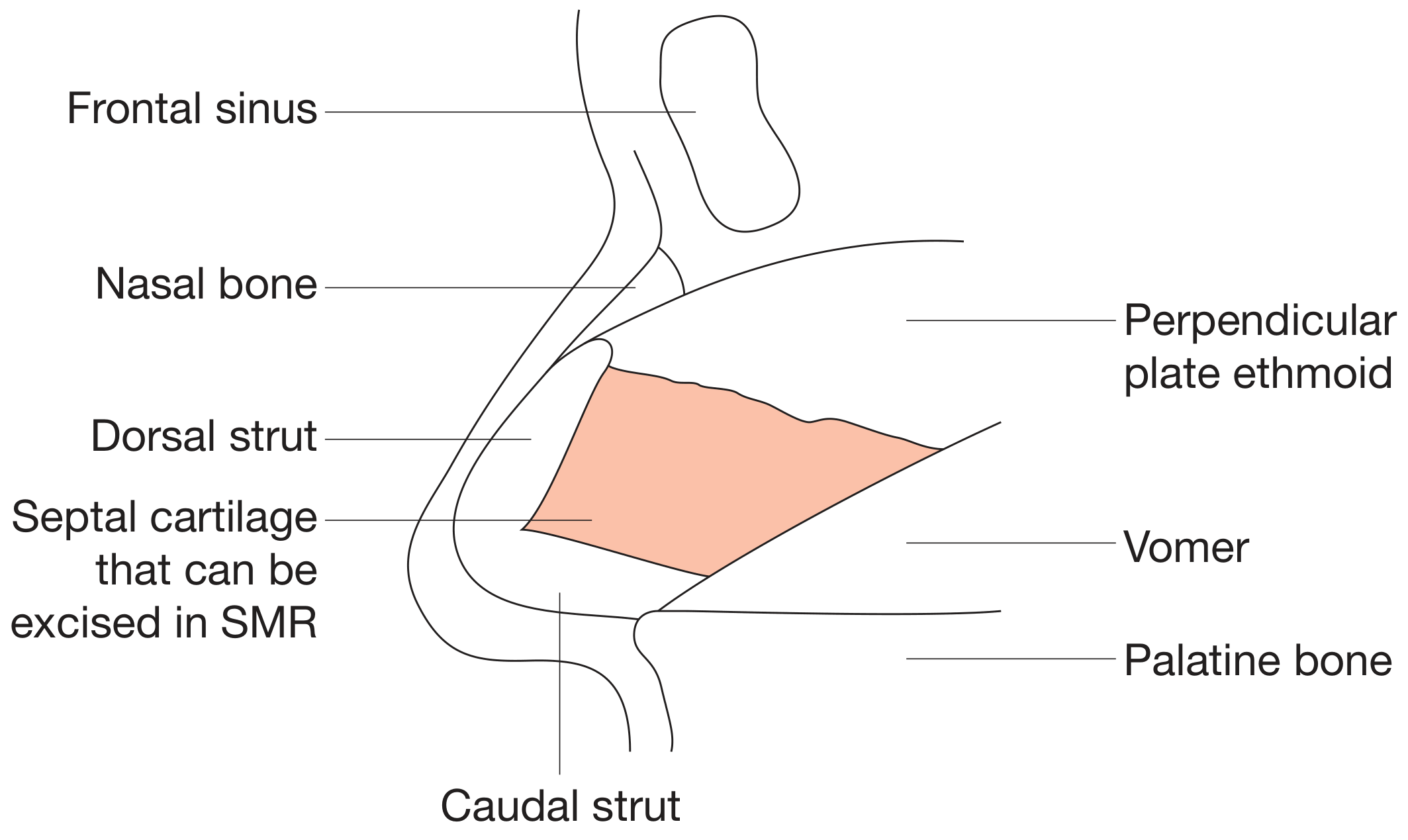
Anatomy of the Nasal Septum
The septum is formed by:
- Cartilaginous part - quadrilateral (septal) cartilage anteriorly
- Bony part - perpendicular plate of ethmoid (posterosuperiorly), vomer (posteroinferiorly), maxillary crest, and palatine bone
- L-strut - the dorsal and caudal arms of the cartilage that provide structural support to the nose; must be preserved during surgery
Etiology
1. Congenital
- Intrauterine moulding of the developing nose
- Birth trauma - forceps delivery or passage through a narrow pelvic canal can cause microfractures of the septal cartilage; healing leads to bending away from the side of injury
2. Traumatic (Most common cause)
- Nasal and midfacial trauma at any age
- Minor trauma in early life can be overlooked; leads to asymmetric cartilage growth due to chondrocyte disruption
3. Developmental (Physiological)
- Unequal growth of the bony and cartilaginous components of the septum during the growth spurt at puberty
4. Racial / Hereditary
- More common in certain racial groups with narrow nasal cavities
Types of DNS (Classification)
| Type | Description |
|---|---|
| Simple deviation | Smooth C-shaped or S-shaped curve to one or both sides |
| Spur | Sharp, shelf-like bony projection arising from the junction of vomer and septal cartilage; often contacts the lateral wall |
| Deviation + spur | Combined deformity |
| Dislocation | Caudal edge of the septal cartilage displaced off the maxillary crest into one nasal passage (visible at the nostril) |
| Thickening | Septum is thickened at the site of an old injury or fracture |
Cottle's areas (I-V) are used to describe the location of the deviation from anterior to posterior. Deviations in areas I and II (anterior) are most symptomatic.
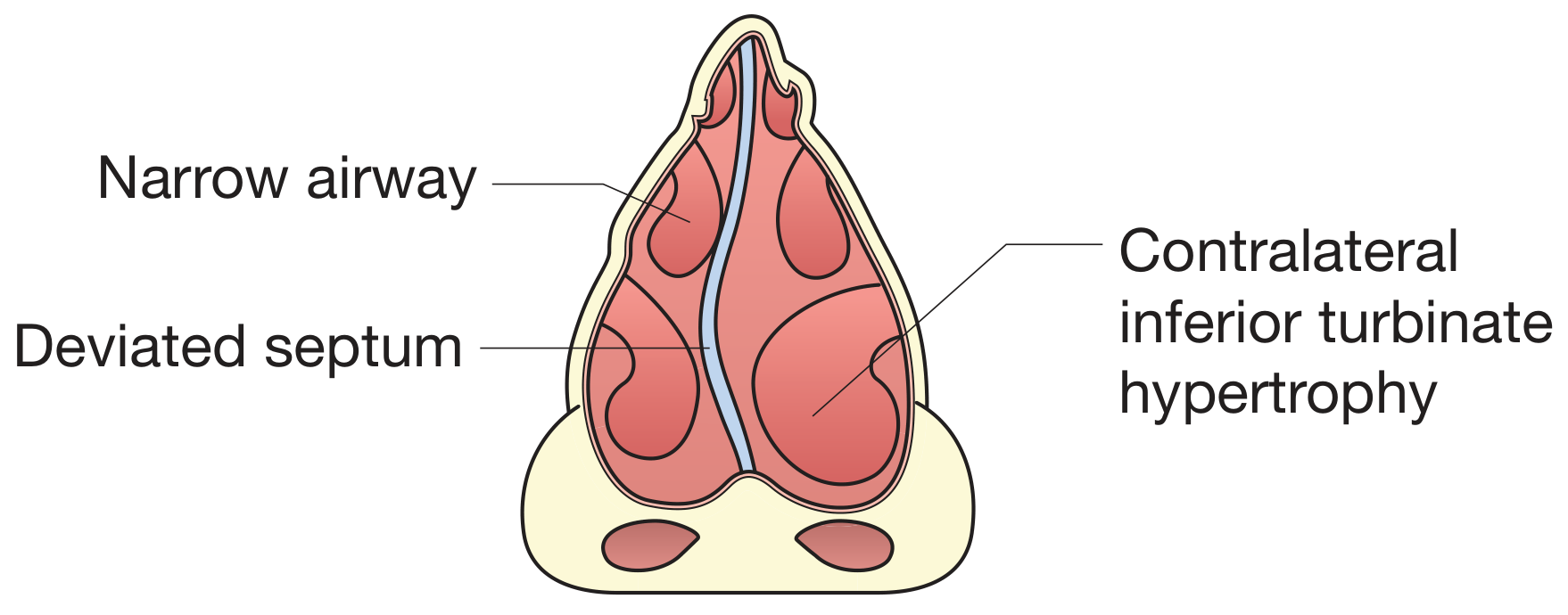
Pathophysiology
Why does the contralateral side block?
Patients with unilateral septal deviation often paradoxically complain of obstruction on the contralateral (wider) side - termed paradoxical nasal obstruction. This is because:
- Increased airflow on the wider (contralateral) side causes excessive evaporation and drying, triggering a reflex mucosal engorgement
- The contralateral inferior turbinate undergoes compensatory hypertrophy to fill the extra space, reducing airflow
Clinical Features
Symptoms
- Nasal obstruction - unilateral or bilateral, often worse on one side
- Nasal discharge - due to impaired drainage from narrowed passages
- Headache - a spur pressing on the lateral nasal wall (contact headache / Sluder's neuralgia) can cause referred pain; also from sinusitis secondary to poor drainage
- Epistaxis - drying and crusting at the apex of the deviation
- Sinusitis - recurrent, due to obstruction of sinus ostia
- Snoring / sleep-disordered breathing - from chronic nasal obstruction
- Anosmia - when deviation blocks the olfactory cleft (rare)
- Mouth breathing - especially in children, with downstream effects (adenoid facies, sleep apnea)
Signs (on anterior rhinoscopy / endoscopy)
- Visible deflection of septum to one side
- Septal spur or thickening
- Contralateral inferior turbinate hypertrophy
- Mucosal congestion, crusting at the convexity
- Externally: nasal deviation, crooked dorsum (in severe cases)
Investigations
- Anterior rhinoscopy - primary assessment
- Nasal endoscopy - better visualization of posterior deviations, spur, and ostia
- CT scan (coronal) - to evaluate sinus disease, plan surgery, and visualize posterior bony deformities
- Cottle maneuver - lateral cheek traction to assess internal nasal valve; however, this gives many false positives; use of a cotton-tipped applicator to specifically lateralize the valve area is more reliable
Treatment
Conservative
- No role of medical treatment for structural DNS
- Treat secondary complications (sinusitis, rhinitis) with appropriate medication
- Nasal decongestants / corticosteroid sprays for symptomatic relief (temporary)
Surgical
1. Submucous Resection (SMR) - Killian's operation
- Principle: Excision of the deviated cartilage and bone while preserving a dorsal and caudal strut of cartilage (L-strut) for support
- Incision: Killian's incision (hemitransfixion) at the caudal edge of the septal cartilage
- Steps: Mucoperichondrial flap elevated > deviated cartilage and bone excised > flap repositioned > nasal pack
- Limitation: Cannot correct caudal or dorsal L-strut deviations. If too much cartilage is removed, loss of dorsal support causes a saddle nose deformity (supra-tip depression or drooping of the nasal tip)
- SMR is now largely replaced by septoplasty
2. Septoplasty (Preferred)
-
Principle: Reconstruction and repositioning of the septum rather than mere excision; the L-strut deviations (most common) can only be addressed by septoplasty
-
Incision: Hemitransfixion (partial or full depending on access needed)
-
Techniques used in combination:
- Cutting/scoring - cartilage scored on the concave side to allow it to spring back to the midline; unreliable alone
- Swinging door technique - caudal excess cartilage excised, septum swung to midline and sutured to anterior nasal spine (PDS 4-0 sutures)
- Grafting - batten grafts used to splint scored segments
- Suturing - mattress sutures to correct minor deformities
- Relocating - osseocartilaginous junction disarticulated to free the cartilage from a deviated bony attachment
-
Endoscopic septoplasty - better visualization especially for posterior deviations; adjunct to functional endoscopic sinus surgery (FESS)
-
Extracorporeal septoplasty - severely deformed septum removed, shaped on a back table, and reimplanted; reserved for extreme cases
-
Paediatric septoplasty - generally deferred until skeletal maturity (age 17-18), as operating on a growing septum risks disruption of nasal growth
Complications of Septal Surgery
| Complication | Notes |
|---|---|
| Septal perforation | Most feared; bilateral mucosal tears at the same site allow cartilage to be devascularized and resorb |
| Saddle nose | Excess cartilage removal in SMR - loss of dorsal support |
| Synechiae (adhesions) | Between septum and lateral wall |
| Hematoma | Between mucosal flaps; requires drainage |
| CSF leak | Rare; if cribriform plate disrupted |
| Infection / abscess | Rare; can be devastating |
| Recurrence | Especially with scoring techniques if inadequately splinted |
| Tip drooping | From loss of caudal strut support |
Septal Perforation (as a complication of DNS surgery)
A hole in the nasal septum causes:
- Turbulent airflow and sensation of blockage
- Nasal crusting and bleeding
- Whistling
- Causes include: iatrogenic (post SMR/septoplasty), trauma, nose-picking, post-septal hematoma, syphilis, tuberculosis, granulomatosis with polyangiitis (Wegener's), chromate salts, cocaine
- Treatment: Closure with local flaps ± cartilage grafts, or septal button (silastic biflanged prosthesis) if surgery is not feasible
Key Exam Points (Dhingra-style)
- DNS is the most common cause of unilateral nasal obstruction
- Paradoxical obstruction = patient complains of blockage on the wider side
- Killian's SMR preserves the L-strut; removing more than this causes saddle nose
- Septoplasty > SMR for L-strut deviations (most common type in practice)
- Minimum age for septoplasty is after skeletal maturity (~17-18 years) to avoid interfering with nasal growth
- Contralateral inferior turbinate hypertrophy is a secondary compensatory change - may need concomitant turbinate reduction
Sources: Bailey and Love's Short Practice of Surgery (28th ed., p. 787); Cummings Otolaryngology Head and Neck Surgery; Scott-Brown's Otorhinolaryngology Head & Neck Surgery (Vol 1, pp. 1185-1192)
Find clinical images of DNS with paradoxical obstruction and compensatory turbinate hypertrophy
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I have all the images needed. Here is the complete visual guide:
Clinical Images: DNS with Paradoxical Obstruction & Compensatory Turbinate Hypertrophy
Image 1 - Schematic Diagram (Coronal Section)
DNS with contralateral inferior turbinate hypertrophy
What to note:
- The septum deviates to the left - creating a narrow airway on the ipsilateral (left) side
- The right inferior turbinate hypertrophies into the wider passage on the contralateral side
- This is the anatomical basis of paradoxical obstruction - the patient complains of blockage on the right (wider) side, because the hypertrophied turbinate reduces that passage back to near-normal resistance
- Bailey & Love's Short Practice of Surgery, 28th ed., p. 787
Image 2 - Endoscopic Views + MRI
Enlarged right inferior turbinate (compensatory) with septal deviation to the left
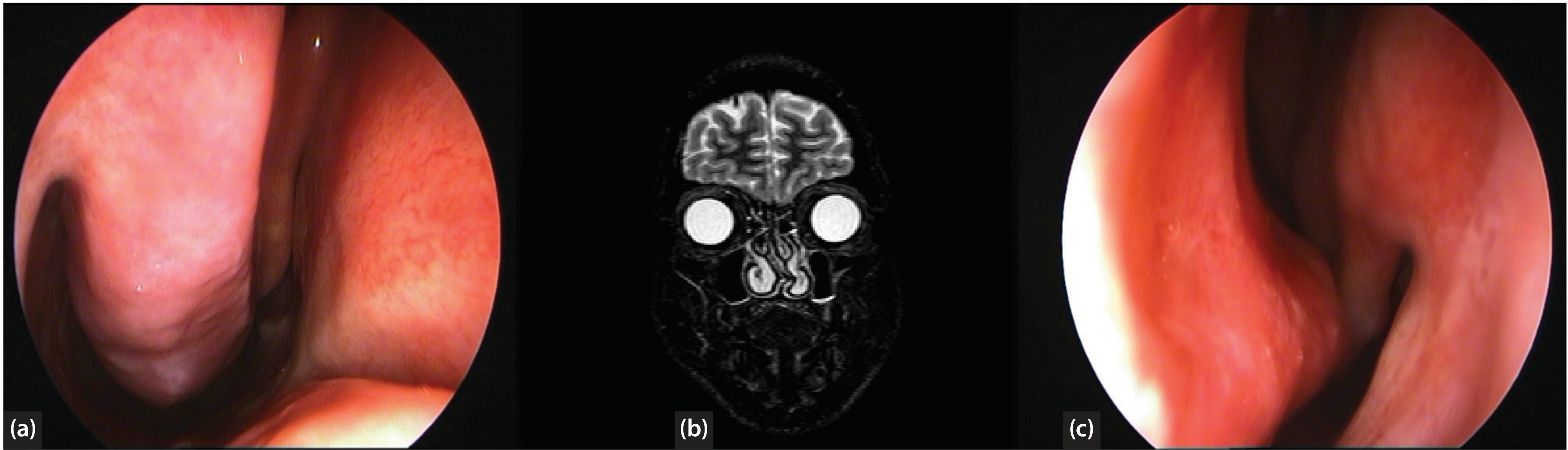
What to note:
- (a) Right nasal cavity - the hypertrophied inferior turbinate bulges medially, almost touching the septum - this is what generates the subjective sensation of obstruction on the "open" side
- (b) MRI (axial) - both inferior turbinates appear as bright bilateral masses; note the asymmetric nasal passages from the deviated septum
- (c) Left nasal cavity - the deviated septum is clearly visible angling into this passage, creating the anatomically narrower side (but the side the patient paradoxically tolerates better)
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1, Figure 105.5
Image 3 - Endoscopic Close-up
Gross enlargement of the inferior turbinate (allergic rhinitis + compensatory hypertrophy)
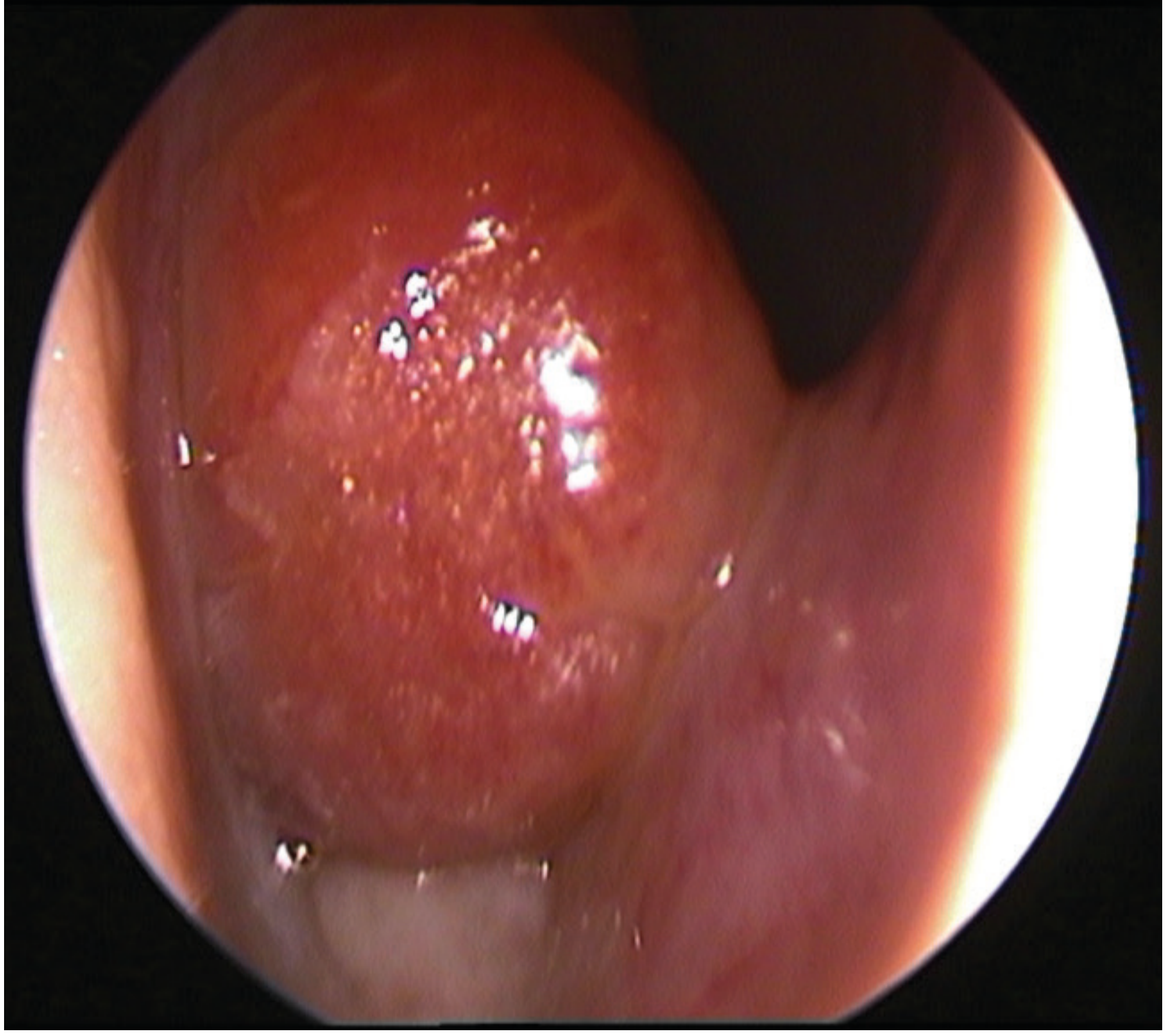
What to note:
- The inferior turbinate is grossly enlarged, hyperaemic (reddened), and fills the nasal passage
- In allergic rhinitis the turbinate can appear pale/purple; here it is erythematous
- Key clinical pitfall - in primary care, this enlarged turbinate head is frequently mistaken for an inflamed nasal polyp
- A turbinate that does not shrink after topical vasoconstriction (e.g. xylometazoline) suggests bony hypertrophy rather than purely mucosal engorgement - this indicates the need for surgical turbinate reduction alongside septoplasty
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1, Figure 105.3
Image 4 - CT Scan (Multi-planar)
Enlarged inferior turbinates - coronal, axial, and sagittal views
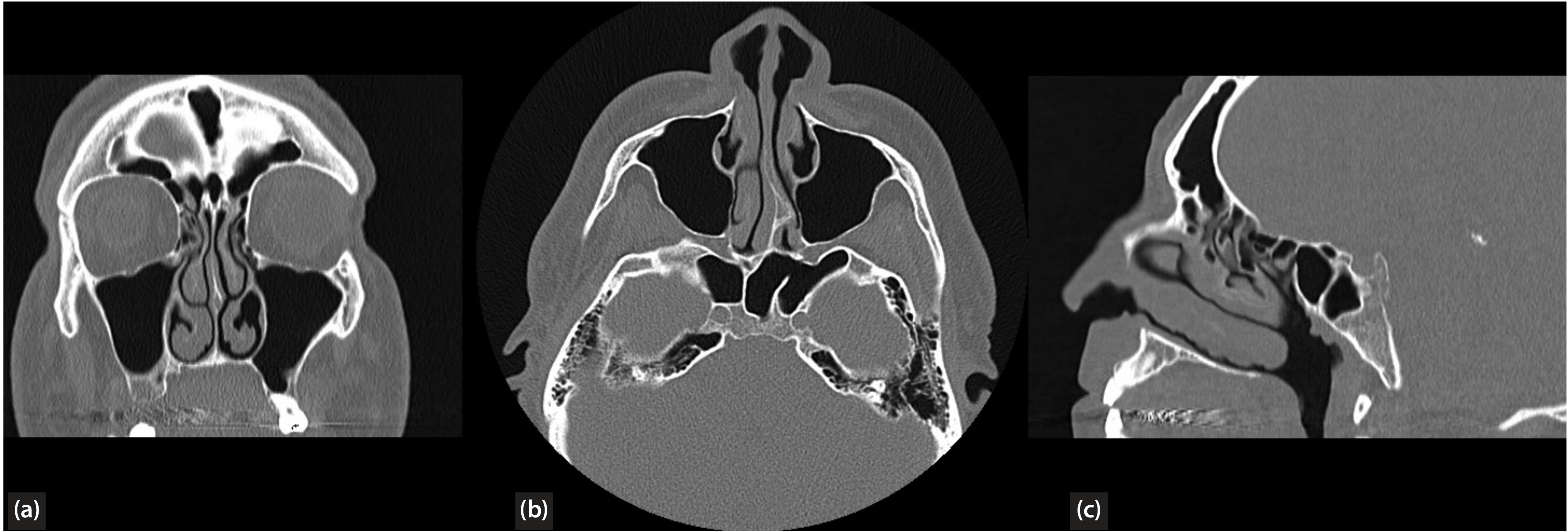
What to note:
- (a) Coronal CT - best plane to assess turbinate size and septal deviation together; clearly shows airway asymmetry
- (b) Axial CT - bilateral inferior turbinate enlargement visible; deviation of nasal septum narrows one passage
- (c) Sagittal CT - shows the full anteroposterior length of the turbinate; posterior end hypertrophy is associated with chronic sinusitis
- CT is the investigation of choice before surgical planning
- Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Vol 1, Figure 105.4
Clinical Summary: The Paradoxical Obstruction Mechanism
"The bony conchal and mucosal hypertrophy is considered compensatory and can be found in the patient with a septum deviated significantly away from the enlarged turbinate. The turbinate mucosa and underlying bone enlarge into the more open nasal passage in pursuit of normalizing nasal airway resistance. Correction of the deviated septum and trimming of the enlarged turbinate are performed together to relieve obstructive complaints. Straightening only the septum without modifying the hypertrophic turbinate will result in obstruction as a result of the large turbinate on the side on which obstruction was not perceived before."
- Cummings Otolaryngology Head and Neck Surgery, p. 570
Surgical implication: Septoplasty alone is insufficient when there is compensatory turbinate hypertrophy - concurrent inferior turbinate reduction (submucous resection of turbinate, radiofrequency reduction, or turbinoplasty) is required, otherwise the patient will develop obstruction on the side that was previously open.
This is a shared conversation. Sign in to Orris to start your own chat.