Amlodipine
Reading File
Finding Sources
Searching PubMed
amlodipine hypertension
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a thorough answer. Here is a complete pharmacological profile of amlodipine:
Amlodipine
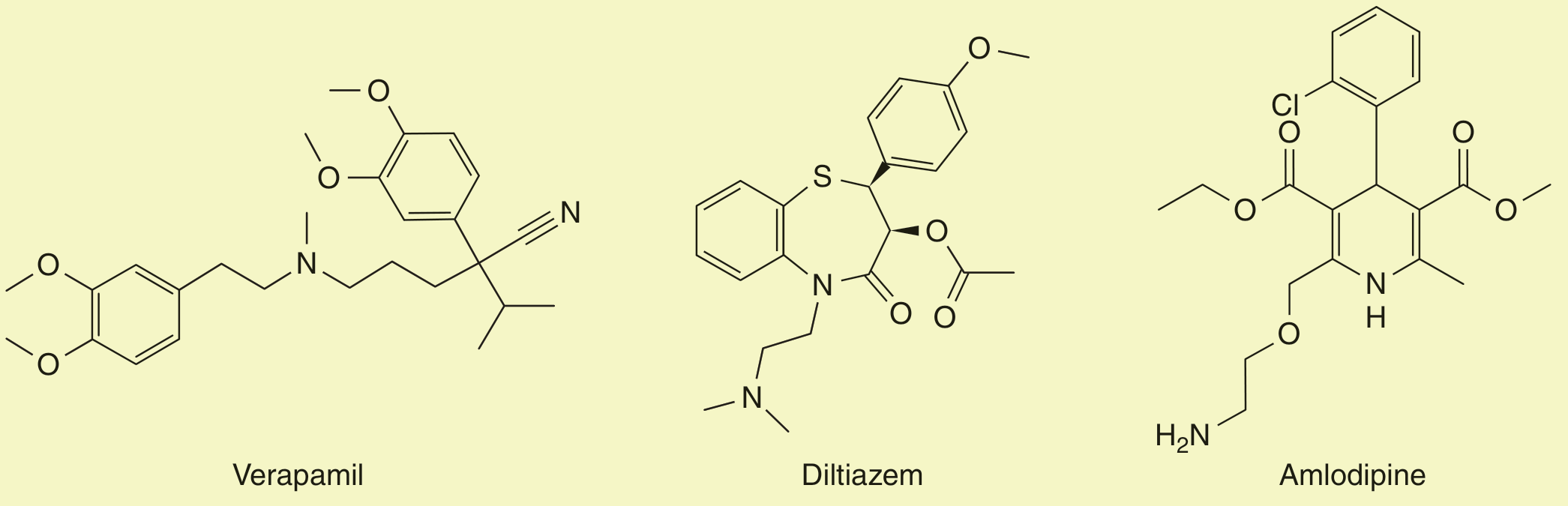
Structures of the three major calcium channel blocker classes. Amlodipine (right) bears a dihydropyridine ring, an aminoethoxymethyl side chain, and a 2-chlorophenyl substituent.
Class & Chemistry
Amlodipine is a dihydropyridine (DHP) calcium channel blocker (CCB). Among the clinically used CCBs - which also include the phenylalkylamine verapamil and the benzothiazepine diltiazem - the DHPs are structurally and pharmacodynamically distinct. Amlodipine is unique within the DHP subclass because it appears to bind to both dihydropyridine and non-dihydropyridine sites on the L-type Ca²⁺ channel, producing peripheral arterial vasodilation without significant activation of the sympathetic nervous system (SNS).
Mechanism of Action
Ca²⁺ channel blockers bind to the α-subunit of the L-type (voltage-gated, "slow") Ca²⁺ channel, reducing Ca²⁺ flux into:
- Vascular smooth muscle - leads to relaxation, arterial dilation, and reduced peripheral vascular resistance (PVR)
- Cardiac myocytes - negative inotropic effect (less prominent with DHPs)
- SA/AV nodal cells - slowed conduction (minimal with amlodipine vs. verapamil/diltiazem)
Because amlodipine acts primarily on vascular calcium channels, it functions almost entirely as an arteriolar vasodilator with minimal direct cardiac conduction effects. This contrasts sharply with verapamil (strongest negative inotrope + chronotrope) and diltiazem (intermediate).
Pharmacokinetics
| Parameter | Value |
|---|---|
| Bioavailability | ~64-90% (almost complete oral absorption) |
| Time to peak (Tmax) | 6-12 hours |
| Plasma protein binding | ~93% |
| Elimination half-life (t½) | 30-50 hours (prolonged in elderly) |
| Onset of clinical effect | ~24 hours |
| Steady state | Achieved after 7-8 days of continuous dosing |
| Metabolism | ~90% hepatic (CYP3A4); 10% excreted unchanged |
| Excretion | Primarily urine (metabolites); no dose adjustment needed in renal impairment |
| Hepatic insufficiency | Reduce dose; 2.5 mg/day starting dose |
The exceptionally long t½ (30-50 h) is what enables once-daily dosing and contributes to smooth, sustained blood pressure control with minimal peak-trough fluctuation. The hypotensive effect can persist up to 5 days after stopping the drug.
Indications
- Hypertension - first-line agent, alone or in combination; particularly effective combined with an ACE inhibitor or ARB. The ASCOT trial showed amlodipine + perindopril was superior to atenolol + hydrochlorothiazide for cardiovascular outcomes. The ACCOMPLISH trial showed amlodipine + benazepril was superior to benazepril + HCTZ.
- Stable angina (effort-induced) - reduces myocardial oxygen demand by decreasing afterload via arteriolar dilation
- Vasospastic (variant/Prinzmetal) angina - directly relaxes coronary arteries, relieving spasm
Dosing
| Population | Dose |
|---|---|
| Adults | 5-10 mg once daily (start 5 mg, max 10 mg) |
| Hepatic insufficiency | 2.5 mg once daily |
| Children 6-17 years | 2.5 mg once daily (max 10 mg/day) |
| Children <6 years | 0.1 mg/kg/dose once-twice daily (max 0.6 mg/kg/24h up to 5 mg/24h) |
Allow 5-7 days before dose adjustments given the drug's gradual onset and long t½.
Adverse Effects
Most are dose-related:
- Peripheral (ankle) edema - the most common adverse effect; caused by precapillary arteriolar dilation and "capillary leakage" rather than fluid retention, making it less responsive to diuretics. Combining with an ACE inhibitor/ARB reduces this via postcapillary venodilation.
- Flushing - due to peripheral vasodilation
- Dizziness / headache
- Palpitations / reflex tachycardia - baroreceptor-mediated sympathetic activation from falling PVR (generally mild with amlodipine due to slow onset)
- Fatigue, nausea, somnolence, abdominal pain
Unlike verapamil and diltiazem, amlodipine does not cause significant bradycardia, AV block, or worsen heart failure (it is safe in HFrEF at standard doses, unlike non-DHP CCBs).
Key Drug Interactions
- CYP3A4 inhibitors (azole antifungals such as fluconazole and ketoconazole; HIV protease inhibitors) - increase amlodipine levels; use with caution
- Cyclosporine, tacrolimus, simvastatin - amlodipine may increase plasma levels and toxicity of these drugs
- Beta-blockers - combination is generally safe and used in angina (no risk of AV block unlike with verapamil or diltiazem)
Contraindications / Cautions
- Known hypersensitivity to amlodipine
- Severe hepatic impairment - dose reduction required
- Unstable angina / acute MI (short-acting DHPs are avoided; amlodipine's long t½ poses less concern but caution is warranted)
- Cardiogenic shock
- Short-acting DHPs (e.g., immediate-release nifedipine) are contraindicated in CAD due to evidence of increased mortality - this concern does not apply to amlodipine given its gradual onset and long action
Comparison with Other CCB Classes
| Feature | Amlodipine (DHP) | Verapamil (PAV) | Diltiazem (BTZ) |
|---|---|---|---|
| Vascular selectivity | High | Low | Intermediate |
| Negative inotropy | Minimal | High | Moderate |
| Heart rate effect | Mild reflex ↑ | ↓↓ | ↓ |
| AV conduction | No effect | Slows | Slows |
| Use in HFrEF | Safe | Avoid | Avoid |
| Drug interactions | Moderate | High | Moderate |
Overdose
In significant overdose, DHP selectivity is lost - amlodipine can affect all calcium channel types, causing:
- Severe hypotension
- Cardiogenic shock
- Noncardiogenic pulmonary edema (occurs in ~50% of severe poisonings)
Management includes high-dose insulin therapy, calcium gluconate/chloride, vasopressors, and lipid emulsion therapy in refractory cases.
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics; Lippincott Illustrated Reviews: Pharmacology; Brenner and Rector's The Kidney (2-Volume Set); Harriet Lane Handbook (23rd ed.); Goodman & Gilman's, p. 633-990
This is a shared conversation. Sign in to Orris to start your own chat.