Tumors of stomach
Reading File
Finding Sources
Finding Sources
Searching PubMed
"gastric cancer" AND "classification"
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive information to write a thorough answer. Let me compile the complete response:
Tumors of the Stomach
The stomach can give rise to several distinct tumor types. About 90% of gastric malignancies are adenocarcinomas. The remainder consist of gastrointestinal stromal tumors (GISTs), lymphomas, neuroendocrine tumors (NETs), and rare others. Each has a distinct biology, clinical behavior, and treatment approach.
1. Gastric Adenocarcinoma
Epidemiology
Since the 1920s, the incidence of gastric cancer has steadily declined, coinciding with widespread refrigeration and reduced food preservation. Despite this, globally it remains the third most common cause of cancer mortality. High-incidence areas include China, Korea, Japan, Chile, and Eastern Europe. In 2023, approximately 27,500 new cases and 11,130 deaths were estimated in the United States alone. Notably, while distal gastric cancer rates have fallen in Western countries, adenocarcinoma of the gastroesophageal junction (GEJ) has markedly increased over recent decades, including in younger patients.
- Harrison's Principles of Internal Medicine 22E, p. 689
Risk Factors
| Factor | Detail |
|---|---|
| H. pylori infection | Present in ~50% of humans; drives chronic inflammation; increases cancer risk especially with high-risk CagA+ strains |
| Diet | High-nitrate foods (smoked, salted, dried); protective effect of fresh fruits/vegetables less robust than once thought |
| EBV infection | Associated with ~10% of gastric cancers; distinct molecular phenotype |
| CDH1 germline mutations | Markedly increase risk for diffuse (signet cell) subtype; prophylactic gastrectomy is an option |
| Pernicious anemia / autoimmune gastritis | Hypochlorhydria promotes bacterial overgrowth and carcinogenesis |
| Prior gastric surgery | Achlorhydria, bile reflux, and H. pylori promote remnant gastric cancer |
| Obesity | Promotes GEJ cancer via reflux; not the sole cause |
| MSI/hypermutation | MLH1 silencing; Gastric-CIMP phenotype |
- Yamada's Textbook of Gastroenterology, 7th ed., pp. 1099-1104
- Harrison's, p. 690
Classification
Lauren Classification (histological - still widely used)
- Intestinal type (~50%): Well-differentiated; malignant cells form glandular-like structures; associated with H. pylori, atrophic gastritis, intestinal metaplasia
- Diffuse type (~33%): Poorly differentiated; cells infiltrate through the gastric wall without cohesion, causing a rigid "leather bottle" stomach (linitis plastica); associated with CDH1/E-cadherin mutations; signet ring cells are the pathognomonic feature
- Mixed/unclassified (~17%)
Intestinal type gastric adenocarcinoma (H&E):
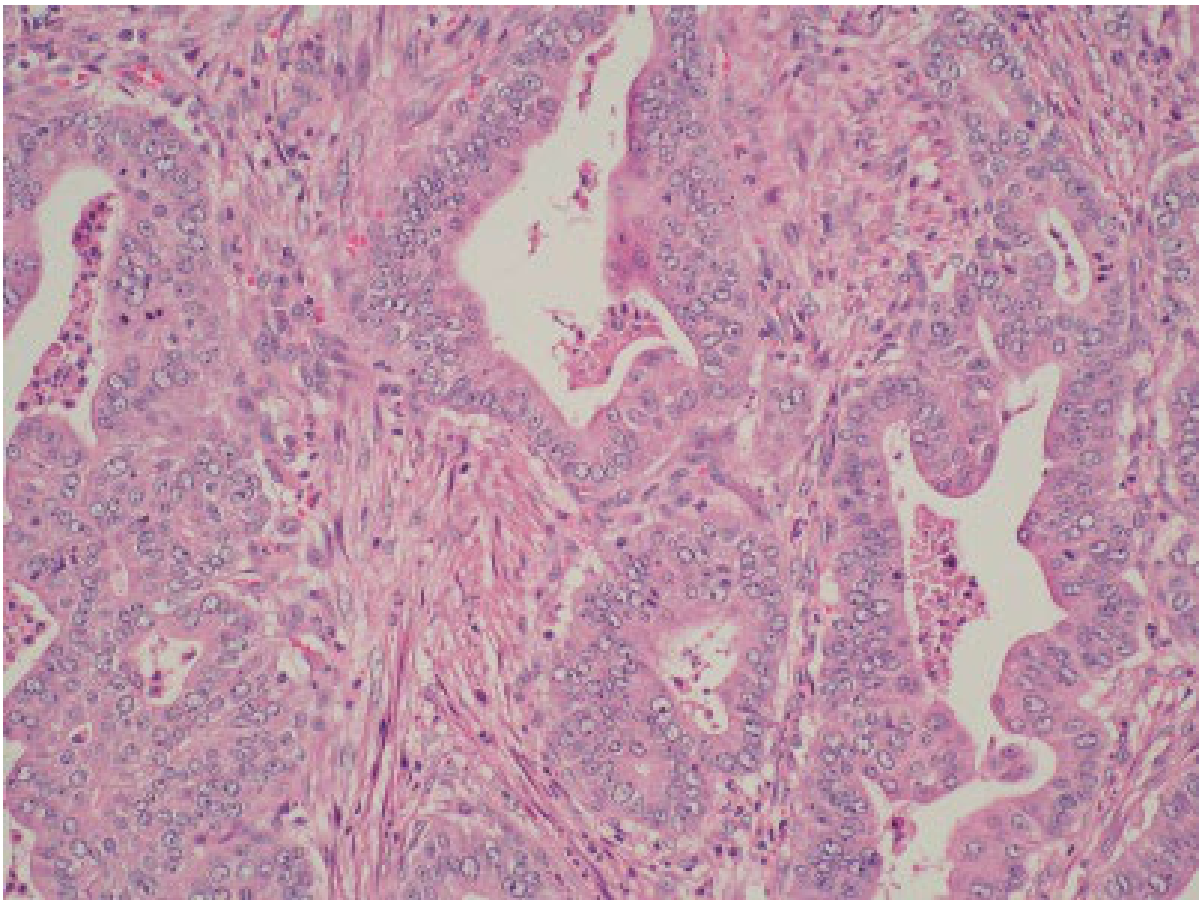
Fig. 52.1 - Intestinal type: glandular structures of varying differentiation within a fibrous stroma (Yamada's Textbook of Gastroenterology)
Diffuse type gastric cancer (H&E):
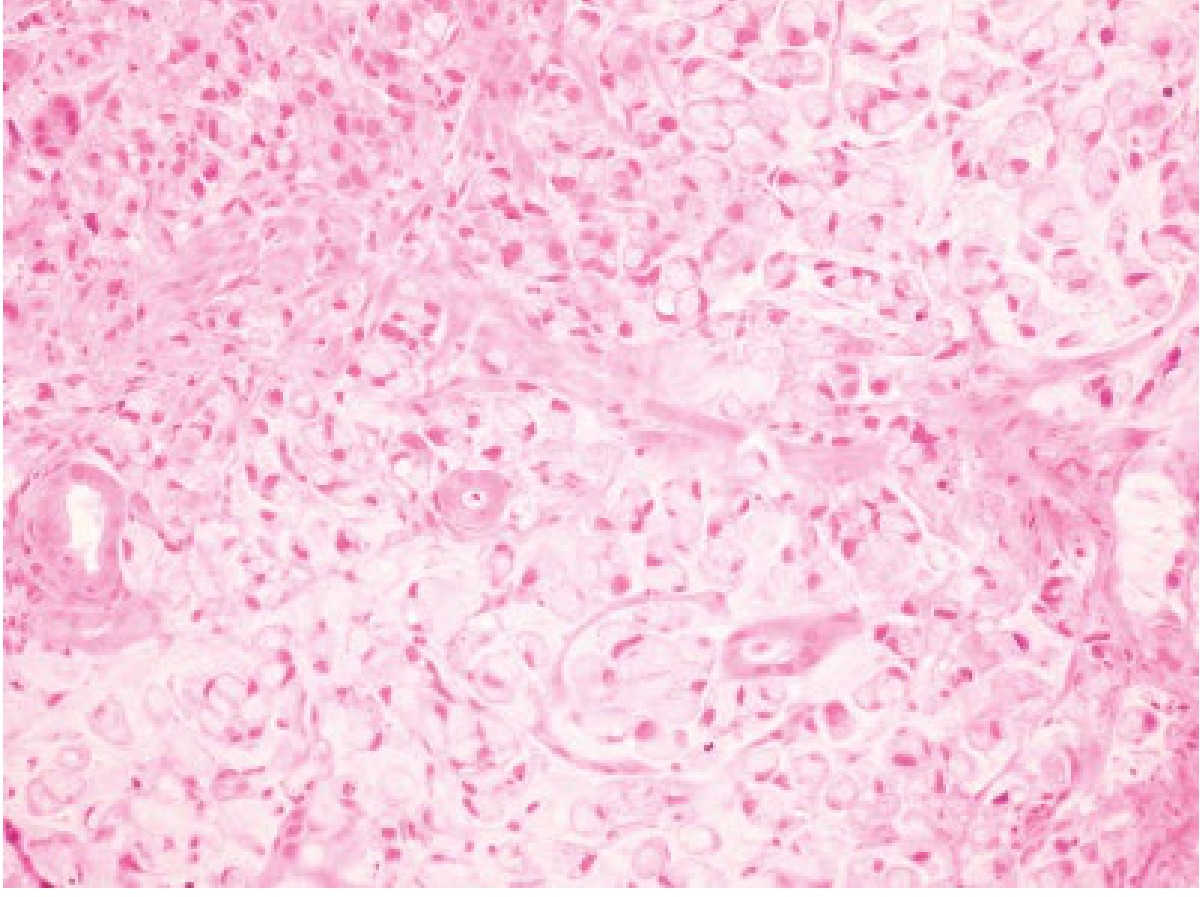
Fig. 52.2 - Diffuse type: lack of cellular cohesion, invasion throughout stroma, signet ring cell morphology (Yamada's Textbook of Gastroenterology)
TCGA Molecular Classification (4 subtypes)
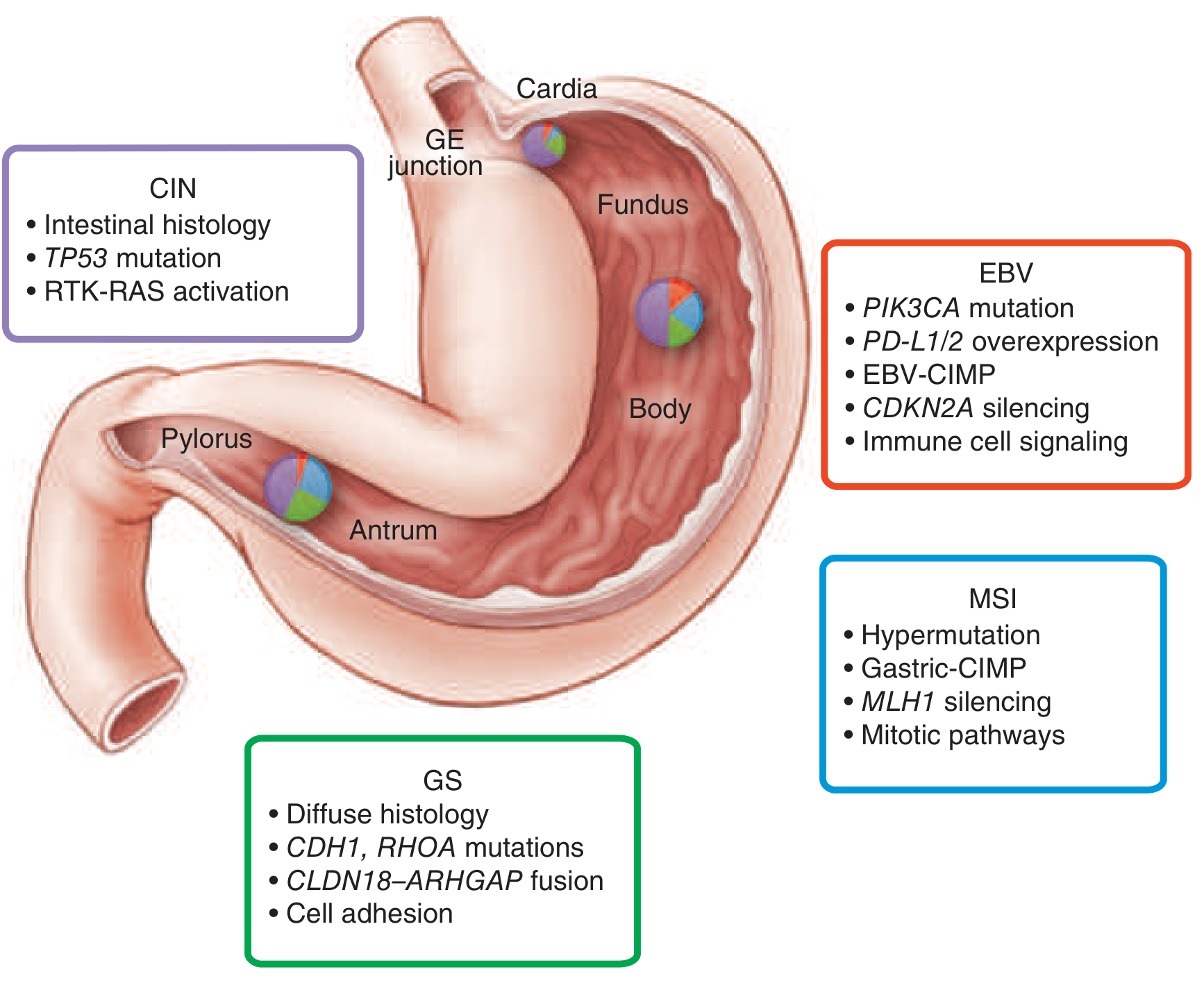
FIGURE 35-2 - Molecular/genomic characterization of gastric carcinoma subtypes (Harrison's Principles of Internal Medicine 22E)
| Subtype | Key Features | Location |
|---|---|---|
| EBV | PIK3CA mutation, PD-L1/2 overexpression, EBV-CIMP, immune cell signaling | Fundus/body |
| MSI (Microsatellite instability) | Hypermutation, Gastric-CIMP, MLH1 silencing | Antrum/pylorus |
| GS (Genomically stable) | Diffuse histology, CDH1/RHOA mutations, CLDN18-ARHGAP fusion, cell adhesion defects | Antrum/pylorus |
| CIN (Chromosomal instability) | Intestinal histology, TP53 mutation, RTK-RAS activation | GEJ/cardia |
Clinical Features
Symptoms:
- Vague upper abdominal discomfort (most common early symptom)
- Hematemesis or melena
- Anorexia and early satiety
- Unexplained weight loss
- Dysphagia/odynophagia (GEJ tumors)
- Iron-deficiency anemia from occult bleeding
Classic physical exam findings (all indicate advanced disease):
-
Virchow's node - left supraclavicular adenopathy
-
Sister Mary Joseph nodule - periumbilical mass (peritoneal spread)
-
Blumer's shelf - pelvic mass on rectal exam
-
Krukenberg tumor - ovarian metastasis
-
Ascites
-
Harrison's, p. 690
Diagnosis & Staging
- Upper endoscopy + biopsy - primary diagnostic tool; intestinal type shows ulcerated mass; diffuse type may show only thickened rugae (initial biopsies often negative - EUS-guided biopsy needed)
- EUS - depth of invasion and regional lymph node staging
- CT chest/abdomen/pelvis - metastatic disease
- Diagnostic laparoscopy - to rule out peritoneal metastases before curative resection
- HER2/ERBB2 testing, PD-L1 CPS, MSI testing - guides targeted/immune therapy selection
Treatment
Localized disease (stages I-III):
- Surgery remains the cornerstone - total or subtotal gastrectomy with D1+ or D2 lymphadenectomy (D2 standard in high-volume centers)
- Perioperative chemotherapy (before + after surgery): platinum + fluorinated pyrimidine (e.g., FOLFOX or FLOT regimen) is standard-of-care
- Preoperative chemoradiation often used for GEJ tumors
- For MSI-high/hypermutated tumors: PD-1/PD-L1 immune checkpoint blockade is increasingly used
- CDH1 germline mutation carriers: prophylactic gastrectomy is an option
Metastatic/palliative disease:
-
Chemotherapy backbone: platinum + fluoropyrimidine (FOLFOX, XELOX)
-
Nivolumab + chemotherapy (CheckMate 649 trial): significantly improved overall survival vs. chemotherapy alone in HER2-negative patients, especially with PD-L1 CPS >5 - now a first-line standard
-
Trastuzumab for HER2-overexpressing/amplified cancers (ToGA trial)
-
DOTATATE-guided therapy for NETs (see below)
-
Harrison's, pp. 692-695
2. Gastrointestinal Stromal Tumors (GISTs)
GISTs are rare mesenchymal tumors arising from the interstitial cells of Cajal (pacemaker cells of the gut wall). The stomach is the most common location (>60% of all GISTs). The majority (>70%) are benign; malignant GISTs metastasize to the peritoneal cavity and liver.
Pathology & Molecular Biology
- CD117 (c-KIT) positive by immunohistochemistry in >95% of cases - the key diagnostic marker
- Other markers: CD34, vimentin, smooth muscle actin
- Molecular driver: activating mutation in KIT receptor tyrosine kinase → ligand-independent constitutive activation of MAPK pathway
- Minority have PDGFRA mutations (mutually exclusive with KIT)
- A subset are "wild type" (no KIT/PDGFRA mutation) - CD117 negativity does not exclude diagnosis
Clinical Presentation
- GI bleeding or anemia (when ulceration occurs)
- Gastric outlet obstruction (distal GISTs)
- Dysphagia (proximal GISTs)
- ~20% found incidentally on endoscopy or imaging
- Patients have increased risk of synchronous and metachronous malignancies
Treatment
-
Surgical resection with curative intent is primary treatment
-
Imatinib (tyrosine kinase inhibitor targeting KIT/PDGFRA): first-line for unresectable, metastatic, or recurrent GIST; also used adjuvantly
-
Sunitinib: second-line after imatinib resistance
-
Prognostic factors: tumor size, location, mitotic index, presence of rupture
-
Resistance develops due to kinase mutations
-
Yamada's Textbook of Gastroenterology, 7th ed., pp. 1099
3. Primary Gastric Lymphoma
Gastric lymphoma accounts for ~5% of gastric malignancies and is the most common extranodal lymphoma site. There is a strong geographic correlation between H. pylori prevalence and gastric lymphoma incidence.
MALT Lymphoma (Low-grade)
Pathogenesis:
- H. pylori infection → chronic gastritis
- Accumulation of CD4+ T cells and B cells in gastric lamina propria
- H. pylori antigens → T-cell activation → IL-2 release → B-cell proliferation
- Progressive genetic rearrangements → IL-2-independent B-cell proliferation
- Cumulative genetic defects → progression to high-grade lymphoma
Key features:
- H. pylori present in 90% of gastric MALT lymphoma cases
- Resembles Peyer patches histologically
- Lymphoepithelial lesions are characteristic (lymphoma cells invading gastric glands)
- Often multifocal
- Less likely to penetrate transmurally or involve lymph nodes vs. high-grade
Treatment:
- H. pylori eradication is first-line antineoplastic therapy
- Complete regression reported in 70-100% of cases with antibiotics
- Median time to complete response: 5 months
- Radiation and chemotherapy for antibiotic failures or H. pylori-negative cases
- About 40% of gastric lymphomas are low-grade MALT type
Non-MALT Lymphomas (High-grade)
-
Most are diffuse large B-cell lymphomas (DLBCL) (previously called "high-grade MALT lymphoma")
-
More aggressive behavior, worse prognosis
-
Other histologies: mantle cell, follicular, peripheral T-cell lymphomas
-
Prognosis closely linked to stage at diagnosis
-
Treatment: chemotherapy (R-CHOP); gastrectomy no longer routinely recommended (chemoradiation preferred over surgery)
-
Mulholland & Greenfield's Surgery, 7th ed., pp. 2342
-
Harrison's Principles of Internal Medicine 22E
4. Gastric Neuroendocrine Tumors (NETs / Carcinoid Tumors)
Gastric NETs represent 7-9% of all gastrointestinal NETs but account for <1% of gastric neoplasms. They are classified by WHO into:
- Well-differentiated NETs (grades 1-3; graded by Ki-67% positivity)
- Poorly differentiated neuroendocrine carcinomas (NECs) - fully malignant
- Mixed neuroendocrine-nonneuroendocrine neoplasms (MiNENs)
Types of Gastric NETs
| Type | Association | Behavior |
|---|---|---|
| Type 1 | Autoimmune gastritis with hypergastrinemia (most common ~70-80%) | Usually small, multiple, benign course; low malignant potential |
| Type 2 | MEN-1 / Zollinger-Ellison syndrome with hypergastrinemia | Less common; intermediate malignant potential |
| Type 3 | Sporadic, no hypergastrinemia | Single large lesion; more aggressive; metastasizes |
Diagnosis & Treatment
- Upper endoscopy + biopsy: initial evaluation
- EUS: depth of invasion, lymph node assessment
- DOTATATE scan (Ga-68 or Cu-64): somatostatin receptor imaging for metastatic disease - guides both staging and PRRT therapy
- FDG-PET/CT: for high-grade NECs
Treatment:
-
Type 1 small tumors: endoscopic resection (EMR/ESD)
-
Larger or higher-grade: surgical resection
-
Small-cell/large-cell NECs: chemotherapy ± radiation (similar regimens to small-cell lung cancer)
-
Metastatic DOTATATE-avid NETs: somatostatin receptor-targeted therapy (octreotide/lanreotide) or PRRT (Peptide Receptor Radionuclide Therapy)
-
Harrison's Principles of Internal Medicine 22E, pp. 695-696
Summary Table: Gastric Tumors at a Glance
| Tumor Type | Frequency | Key Marker / Mutation | H. pylori Link | Primary Treatment |
|---|---|---|---|---|
| Adenocarcinoma (intestinal) | ~60% of gastric Ca | Lauren intestinal; TP53, RTK-RAS | Strong | Surgery ± periop chemo |
| Adenocarcinoma (diffuse) | ~20-25% of gastric Ca | CDH1/E-cadherin, signet ring cells | Moderate | Surgery; CDH1 carriers: prophylactic gastrectomy |
| GIST | ~2-3% | CD117 (KIT), PDGFRA | None | Surgery; imatinib |
| MALT lymphoma | ~4-5% | Lymphoepithelial lesions | Very strong (90%) | H. pylori eradication |
| DLBCL | ~3-4% | B-cell markers | Moderate | R-CHOP chemotherapy |
| Gastric NET (type 1) | ~1% | Chromogranin A, synaptophysin | Indirect (autoimmune) | Endoscopic resection |
| Gastric NET (type 3) | Rare | DOTATATE avidity | None | Surgery; PRRT |
Sources:
- Harrison's Principles of Internal Medicine 22E (2025), Chapter 35 - Tumors of the Stomach, pp. 689-696
- Yamada's Textbook of Gastroenterology, 7th ed., Chapter 52 - Tumors of the Stomach, pp. 1099-1104
- Mulholland & Greenfield's Surgery, 7th ed., Chapter 47 - Gastric Lymphoma, p. 2342
This is a shared conversation. Sign in to Orris to start your own chat.